
Abstract
Introduction
A factor analysis found that the development of dental fear is associated more strongly with the subjective experiences of pain and trauma than with objective dental pathology. 1,2 Although pain is blocked by local anesthesia, the use of a conventional high-speed handpiece for bone removal can frighten the patient, and the noise and vibration of rotary instruments can cause discomfort and dental anxiety. The erbium-doped yttrium aluminum garnet (Er:YAG) laser produces much less noise, vibration, and pressure than does a high-speed handpiece during dental procedures, thereby minimizing the need for local anesthesia. 4,5
The State–Trait Anxiety Inventory (STAI) is a brief self-rating scale for the assessment of state and trait anxiety in adults. This instrument was introduced by Cattell 6 and has been further elaborated by Spielberger. 7
Because the STAI measures anxiety as a feature of the general population, scores are expected to be distributed normally. State anxiety refers to subjective and transitory feelings of tension, nervousness, and worry produced by the activation of the autonomous nervous system at a given moment. 8,9 Trait anxiety refers to “relatively stable individual differences in anxiety proneness as a personality trait,” that is, in the tendency to perceive and respond to stressful situations with an elevated intensity of state anxiety reactions. 8
The aim of this study was to investigate preoperative anxiety and postoperative comfort in patients undergoing apicectomy procedures performed using conventional instruments or an Er:YAG laser.
Patients and Methods
This prospective study was conducted in the Department of Oral and Maxillofacial Surgery, Dentistry Faculty, Marmara University. The study protocol was approved by the local institutional review board (protocol number: 2012/7), and all patients provided written informed consent. Twenty-eight consecutive healthy patients who divided into two subgroups (group A, Er:YAG laser treatment, n=14; group B, treatment with conventional handpieces, n=14) were enrolled in this study. All patients with an average socioeconomic level and at least high school educated were ≥18 and ≤45 years of age, and each had one anterior maxillary tooth with a related periapical lesion ≤1 cm2 radiologically. With the patient under local anesthesia, a Partsch's incision was made, and a mucoperiosteal flap was elevated. Necrotic teeth with apical lesions were removed. In group A, apicoectomies were performed using an Er:YAG laser (2940 nm, Lightwalker; Fotona Ltd., Ljubljana, Slovenia). Patients in group B were treated with conventional surgical handpieces. Wounds were sutured with 4-0 polyglactin, and sutures were removed 1 week later. All the operations were performed by the same operator and measurements were made by another clinician. The operator was blinded to the evaluation of the STAI and questionnaire scores during the whole study.
Patients completed Spielberger's STAI preoperatively (Fig. 1). The STAI-trait (STAI-T) and STAI-state (STAI-S) subscales consist of 20 items each, with scores for each item ranging from 1 (“not at all”) to 4 (“very much); higher subscale scores indicate greater trait or state anxiety. Subjects indicate to what extent a given item represents their state. To control for positive or negative set, half of the questions are formulated in terms of positive emotions and the other half refer to negative emotions. The scaling of the positively formulated questions is reversed when computing the total score. Patients also completed a postoperative questionnaire (PQ) (Fig. 2) comprising eight yes/no questions, which was prepared by the research team to evaluate the effect of the surgical approach (Er:YAG laser vs. conventional instruments) on patients' comfort during surgery. Each question was answered on a scale of 0 to 3, with 3 indicating the greatest level of discomfort. Total PQ scores were used to calculate PQ values (Table 1). Patients' demographic data were also collected. Differences in questionnaire scores according to sex were evaluated by independent samples t tests. Other questionnaire data were evaluated by one way analysis of variance using SPSS software (version 7.5 for Windows; SPSS Inc., Chicago, IL).
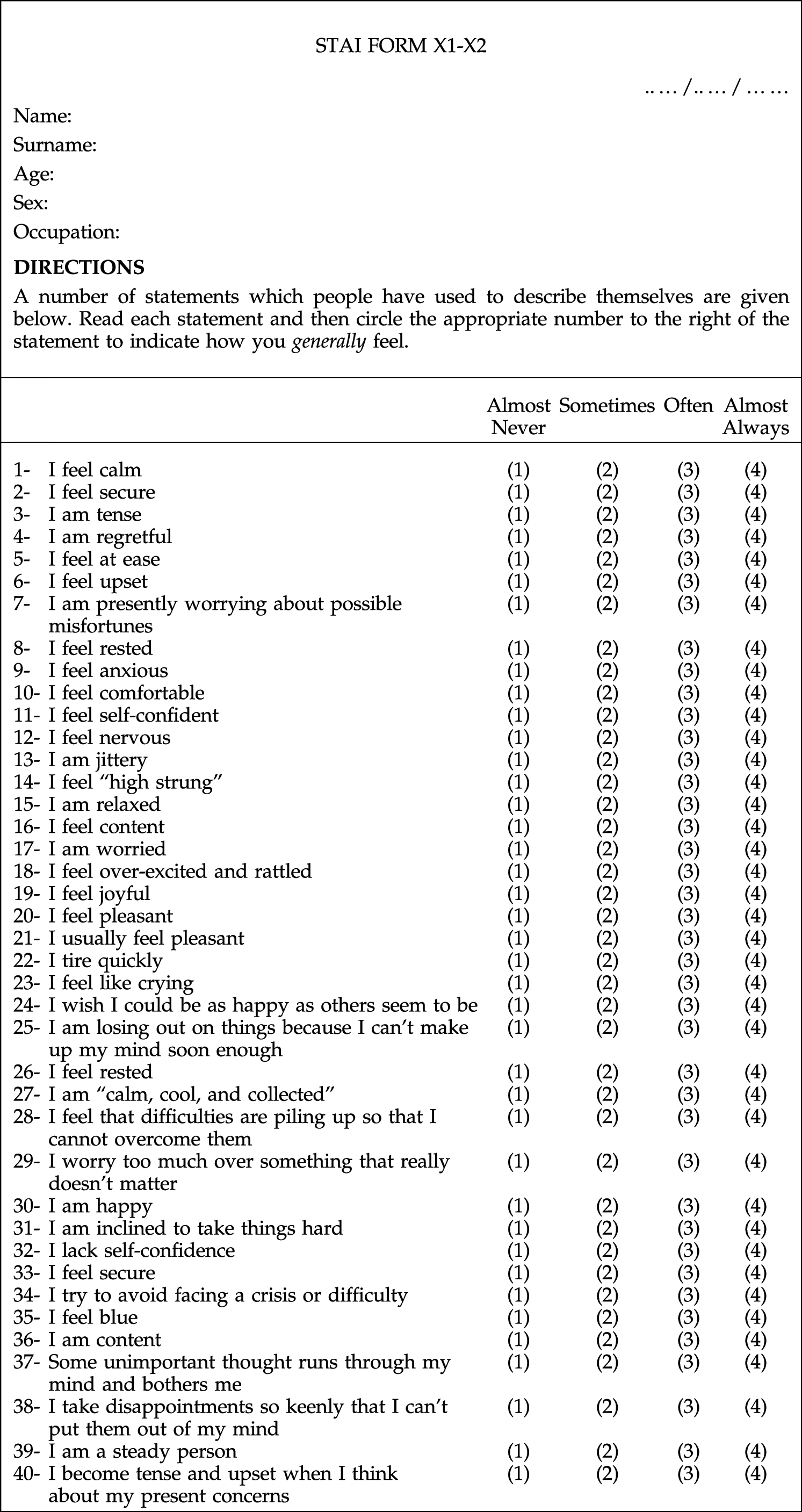
Self evaluation questionnaire form.

Postoperative questionaire form.
PQ, postoperative questionnaire.
Results
The mean age of the 28 patients (16 men, 12 women) in this study was 35.4 (range, 29–44) years (group A, mean=36.8 years; group B, mean=34 years). No significant difference in age or sex was present between the two treatment groups. All operations were performed successfully, with no intraoperative or postoperative complication. The postoperative course was uneventful in all patients, with no adverse event occurring at any time during healing.
Mean STAI-S and STAI-T scores were 46.29±12.513 and 31.29±12.513, respectively, for patients treated with an Er:YAG laser and 50.14±16.16 and 35.14±16.16, respectively, for patients treated with conventional instruments. The means and standard errors of STAI-S and STAI-T scores in the total population are shown in Table 2. Total PQ scores and mean PQ values were 35 and 0.57, respectively, in group A and 58 and 1.29, respectively, in group B. Although STAI-S and STAI-T scores were lower in the Er:YAG laser group than in the conventional instruments group, the differences were not statistically significant.
STAI, State–Trait Anxiety Inventories; con. ins., conventional instruments.
Discussion
Patients who experience anxiety during dental visits have reported that the worst experiences occurred early in their lives. The identification of anxiety can be rather difficult; many dental practitioners are aware of dental anxiety and its potential effects on their practices but admit readily to a surprising lack of confidence about their ability to identify and manage the condition. 1 –3,10 –12 Patient perception is a very important motivator in the dental profession. Milgrom et al. 13 reported that direct conditioning and modeling were important predictors of dental anxiety originating in childhood.
Spielberger's STAI was initially developed to assess anxiety in adults, and has been used extensively in research and clinical practice. This self-report instrument measures state and trait anxiety separately. The presence and intensity of state anxiety may fluctuate over time, whereas trait anxiety denotes “relatively stable individual differences in anxiety proneness” 7 and refers to a general tendency to respond with anxiety to perceived threats in the environment.
STAI-S scores increase in response to physical danger and psychological stress and decrease as a result of relaxation training. Consistent with the trait-anxiety construct, psychoneurotic and depressed patients generally have high STAI-T scores. STAI scores can be interpreted directly, with high subscale scores indicating greater trait or state anxiety. 9
The laser used in the present study is pulsed, and causes an audible sound that may provoke a frightened response in patients. The ultimate question is whether lasers will provide fewer negative stimuli than do dental drills. Laser systems were shown to offer distinct advantages over conventional surgical procedures, such as decreased bleeding tendency, less tissue trauma, reduced scar formation, and bacteriostasis. 14 –16
Previous studies have investigated several types of laser in efforts to identify an alternative to conventional high-speed handpiece preparation. The Er:YAG laser has shown potential in the removal of caries, tooth structures, and bone, with minimal thermal effects on the hard and soft tissues. 16,17 Hibst and Keller 18 –21 investigated the ablation efficiency of the Er:YAG laser and its thermal effects on dental hard tissues and dental restorative materials. They found that this laser could cut dental hard tissues without causing a significant thermal effect. Boj et al. 22 used an erbium, chromium, yttrium, scandium, gallium, and garnet (Er, Cr:YSSG) laser to treat 49 pediatric patients (33 restorations, 16 oral surgeries). At the end of treatment, the patients indicated the degree of pain felt on the Wong–Baker face pain scale. Scores were higher in children undergoing surgery than in those undergoing cavity preparation. 22 Liu et al. 16 reported that cavity preparation with the Er:YAG laser was a good option for frightened pediatric patients, because it produces less pain and has acceptable efficiency compared with conventional mechanical preparation. In our study, mean STAI-S scores were lower in patients treated with the Er:YAG laser than in those treated with conventional instruments.
Bone reduction with conventional rotary cutting instruments, especially in hard bones and in the maxilla, causes patient discomfort because of the high-pitched noise and vibrations conducted through bone. Conventional handpieces may produce a frightening sound and bur vibrations that increase dental anxiety and may induce patients' head and body movements. The Er:YAG laser has been reported to produce a minimum level of noise. 5 The high PQ scores and values we observed in group B were consistent with the findings of previous studies.
Conclusions
The Er:YAG laser offers several advantages over conventional rotary instruments in dental care, such as the absence of mechanical vibration, lack of pressure, and force sense. The results of the present study do not confirm a strong effect on patient anxiety. Although the STAI scores were lower in the Er:YAG group, this is not statistically significant. Therefore, use of the Er:YAG laser alone cannot contribute to the resolution of dental anxiety.
Footnotes
Author Disclosure Statement
No competing financial interests exist.