
Abstract
Introduction
W
As a modality of rehabilitation, low-level laser therapy (LLLT) has been suggested for clinical use. 4 LLLT can improve the repair process of injury tissues, and reduces inflammation and pain. 4 Previous studies using cellular and animal experiments have revealed that LLLT is associated with improved bone healing, and that clinical trials in humans are warranted. 5 –7 Several cellular studies have reported that LLLT positively affects bone cells, 6,7 but to date, studies on the clinical use of LLLT are lacking. In an animal study, Lirani-Galvao et al. demonstrated that LLLT increased osteoblast activity and bone density by boosting the activation of osteoblasts in later stages of bone repair. 8,9 Based on these results, it is reasonable to presume that LLLT can reduce the time required for a fracture to heal. The use of LLLT may have bone-healing utility for CFB patients.
The wavelengths of LLLT range from 600 to 1000 nm with power densities from 1 mW/cm2 to 5 W/cm2, and treatment times typically range from 10 sec to 10 min, although certain studies have introduced wavelengths and treatment times outside of these ranges. 9,10 The outcomes of LLLT depend upon irradiation parameters (wavelength, power density, and pulses) and irradiation time, often referred to as the“dose,”and expressed as energy (J) or energy density (J/cm2). In a review study conducted by Bjordal et al., no substantial effects of LLLT were reported because the energy delivered was inappropriate; the dose was either too high or too low. 10 LLLT at wavelengths between 810 and 830 nm, and dosages between 6 and 10 J, was recommended to induce anti-inflammatory effects to treat orthopedic diseases. 11 Studies have suggested that a laser wavelength of 830 nm can deeply penetrate tissue, and that satisfactory absorption can be achieved, thereby inducing favorable clinical results. 10,11 However, based on our research, no studies investigating the effect of LLLT on bone fractures in humans have been performed. Therefore, the therapeutic outcomes of applying LLLT (830 nm; 9.7 J/cm2) to CBFs in the human wrist and hand were examined in this study.
Methods
Patients diagnosed with wrist and hand fractures were recruited and referred to the Division of Orthopedics at Da-Chien Hospital in Miaoli, Taiwan. The orthopedist confirmed that no wounds had occurred over the fracture site, and then classified the fractures as grade II trauma injuries based on the Abbreviated Injury Scale. 12 This clinical research proposal was confirmed and approved by the hospital. The inclusion following criteria were used to select patients: (1) the patients had been diagnosed with a CBF, but had not been treated by undergoing an operation or splinting; (2) the fracture was discovered in the phalanges, or the metacarpal, carpal, distal ulna, or distal radial bones; and (3) the patient had never received LLLT before. The Research Ethics Committee of the Institutional Review Board for Human Subjects Research approved all of the study protocols (No. DC-ETHICS-97090701). After being informed of the study in detail, all of the participants gave informed consent for treatment. The participants were recruited between July 2009 and August 2011, and their injuries were classified according to the gradation of fractures defined by the Orthopaedic Trauma Association. 13 During the 4-week study, the participants were instructed to cease taking all anti-inflammatory drugs, and other treatments, such as physical therapy and taking Chinese medicine, were also disallowed.
Study design
The experiments were conducted on a double-blind basis, and the participants were randomly assigned to one of two groups. The participants in the laser group received LLLT. In this group, a laser device (Painless Light PL-830, Advanced Chips & Products Corp., USA) was used to emit a laser beam focused on an area of 370 mm2 using two inbuilt laser diodes. The distance between the inbuilt laser diodes in the output head was 2.5 cm. The device specifications are shown in Table 1. The treatment dose, expressed as energy density, was 9.7 J/cm2. The laser device made direct contact with and irradiated the skin of the fracture site, ensuring that the input dose was stably sent into the unit area. The participants in the placebo group, in which there was no laser output, received sham laser treatment emitted onto the fracture site. The participants did not know whether they were receiving the laser or sham laser treatments during the study.
Clinical assessments were performed by a physician. Using radiographic images, a physician palpated potential suitable sites for exposure to the treatment. A belt was used to hold the output head of the laser device above the fracture site (Fig. 1), and the area of each site was irradiated using a treatment dose of 9.7 J/cm2. The laser device was equipped with a timer, which monitored and automatically turned off the power after 600 sec, after which an audible signal was issued to alert the participant that the treatment session had ended. The treatment was administered to the wrists or hands of the participants in both groups for 600 sec per fracture site by a physical therapist, once a day, 5 days a week. Each treatment course lasted 2 weeks. The only difference between the treatments for the placebo and laser groups was that the placebo treatment employed the laser device without generating a laser output. The laser devices, which were provided by the study investigator to the physical therapist, appeared identical. Although the physical therapist was informed which laser devices were used to treat which groups, the physical therapist was not informed that the sham laser device did not generate an energy output, to avoid psychological effects. Assessments were conducted before and after LLLT, and at the 2-week follow-up. The assessment devices included a digital prehension device and a digital imaging system, calibrated using commercial agents (Good Line Corporation and General Electric Company, Taiwan) at the beginning of the study. The physician and physical therapist did not know whether the participants were members of the laser or placebo groups.
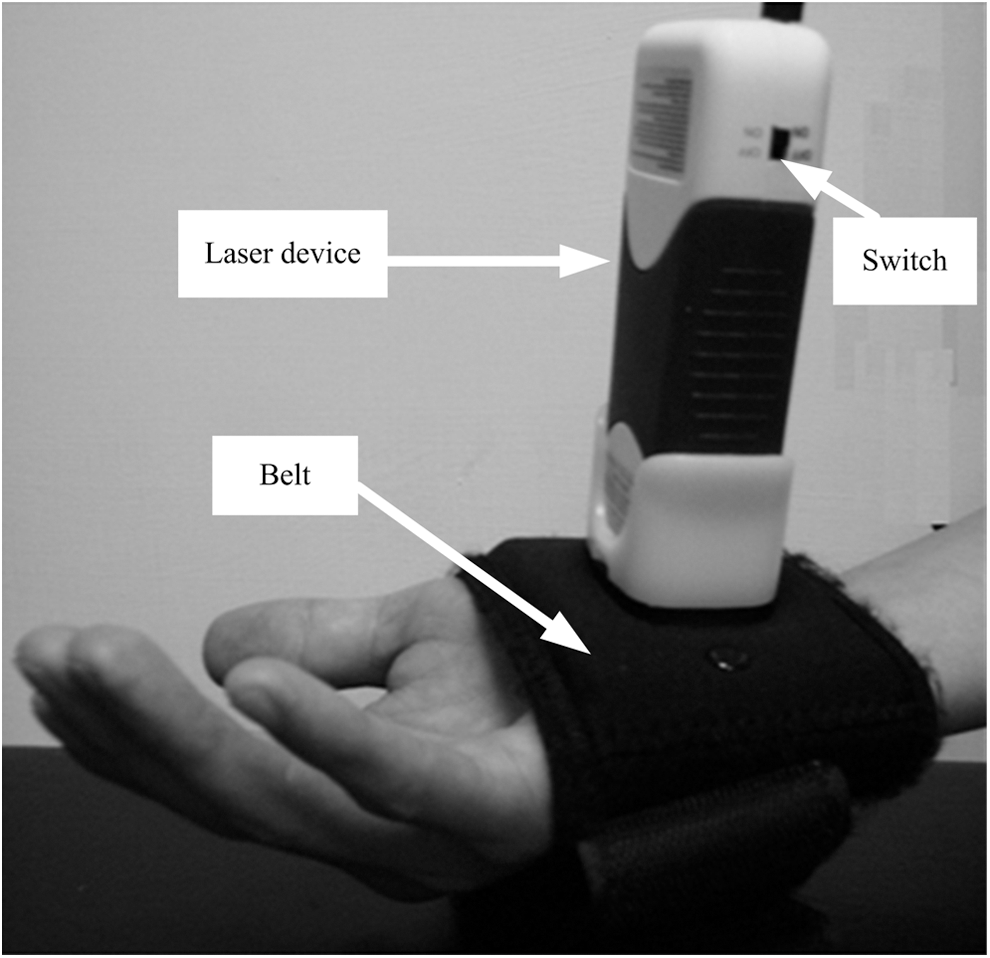
A belt was used to hold an output head of the laser device (average power 60 mW, peak power 8 W, 10 Hz, 600 sec, and 9.7 J/cm2 per each fracture site) above the fracture site. After the clinical assessments performed by a physician, a physical therapist applied low-level laser therapy (LLLT) to the fracture site.
Assessments
Pain measurement
The fracture site of each participant was identified based on radiographs and physical examinations. Thereafter, the physician manually and gently pressed the fracture site to measure the intensity of the participants' pain, and participants were asked to assess their pain by using a visual analog scale (VAS).
Quick Questionnaire for Disabilities of the Arm, Shoulder, and Hand (Quick DASH)
Quick DASH is a standardized measure used to record the physical function of and the symptoms exhibited in a patient's upper extremies. 14 It is a useful tool for assessing the therapeutic outcome of patients with traumatic hand injuries, and has strong reliability and validity for assessing the functional ability of wrists and hands. 14,15 The self-report questionnaire contains 11 items for evaluating the difficulty of specific activities, of which 4 items address the patient's ability to work, and 4 items concern the patient's ability to play sports. Each item is measured based on a five point response scale. The total scores are calculated using [(the sum of n responses/n)−1]×25, where n is equal to the number of completed responses. The total scores range from 0 (no disability) to 100 (most severe disability).
Hand and finger grip strength
The strength of each participant's finger grip was assessed based on the power of their tridigital pinch, which was measured individually, using the Jamar Hydraulic Pinch Gauge (Lafayette Instrument Company, USA). Hand grip strength was measured using the Jamar Hydraulic Hand Dynamometer (Lafayette Instrument Company, USA). Participants sat in a chair, keeping their elbows flexed at 90 degrees (approaching the chest). 16 The mean scores of both groups for these five separate measurements were recorded, with a rest interval of 5 min between each measurement.
Radiographic signs of bone healing
Anteroposterior and lateral views of the injury were examined using radiography. The radiographic image in Fig. 2 shows a participant's right wrist and hand before and after LLLT. To assess the progress of healing, the fracture site of each participant was evaluated using a digital imaging system (Nu Film Versions 4.05, Thinking System Corporation, USA). The radiographic signs of bone healing were evaluated using two parameters. 17 The first parameter was the fracture line (FL), and healing was determined to have occurred if the FL present in the original fracture was absent. The second parameter indicating healing was detectable cortical bridging (CB), defined as the formation of calluses and the gradual disappearance of the interruption of the cortex at the fracture site. The radiographic measures were evaluated and recorded by the same physician in each case, and the same physician calculated the differences between the measurements.
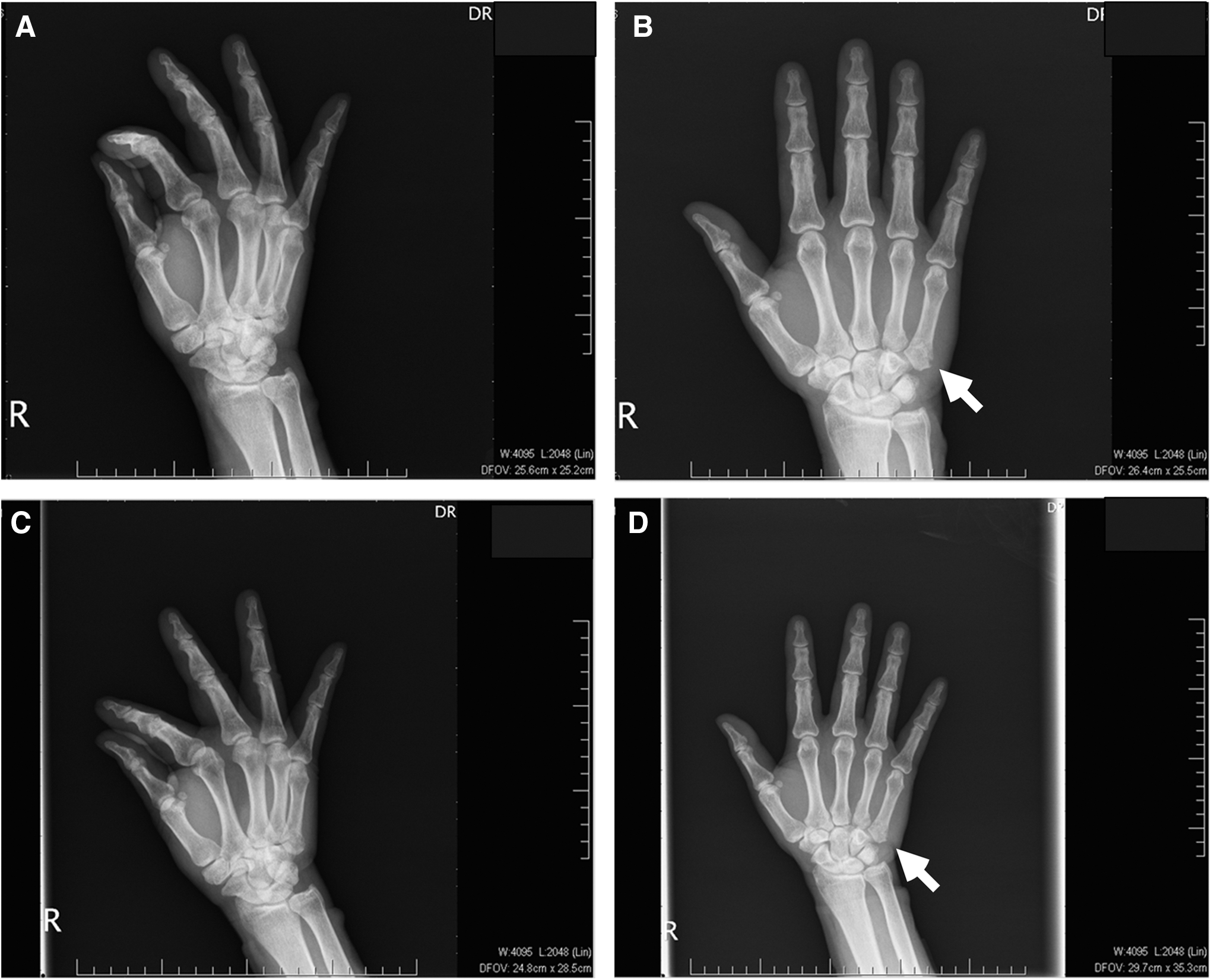
In laser group, this closed bone fracture (CBF) patient sustained a noncomminuted fracture of the metacarpal bone of the right hand. Anteroposterior
Statistical analysis
The SPSS 13 software package was used to analyze the data. An independent-sample t test was used to examine differences between the groups, including age, onset of fracture, VAS scores, quick DASH results, and hand and finger grip strength. These continuous variables were also analyzed using repeated measures analysis of covariance (RMANCOVA) before and after LLLT, and at the 2-week follow-up. The Pillai's trace test was also used for a multivariate approach, and the post-hoc test was used to enable multiple variable comparisons. Categorical variables, including the ratios for sex, affected side, and the percentages of absent FL and detectable CBF, were analyzed using the McNemar test. All of the statistical tests were two tailed, and p values<0.05 were considered statistically significant.
Results
A total of 50 participants (29 men and 21 women) with CBFs in the wrist or hand were included in this study. The average age of all the participants was 32.66±7.70 years, and the average onset of all the fractures that had occurred was 6.54±1.29 days. The demographic data and fracture conditions of all participants are shown in Tables 2 and 3. No participants in either group withdrew during the study.
FL, fracture line; CB, cortical bridging; OTA, Orthopaedic Trauma Association.
As shown in Table 4, no significant differences in VAS scores, quick DASH results, or hand and finger grip strength were observed between the two groups before treatment. However, after treatment and at the follow-up, significant differences emerged between the groups (p<0.05). As shown in Figs. 3 and 4, significant changes were observed in the LLLT group measures of VAS, quick DASH, and hand and finger grip strength before and after treatment and at the follow-up. In the placebo group, significant differences were observed in VAS and finger grip strength measures before and after treatment (p<0.05); however, at the 2-week follow up, only the VAS scores significantly changed after the patients received treatment (p<0.05).
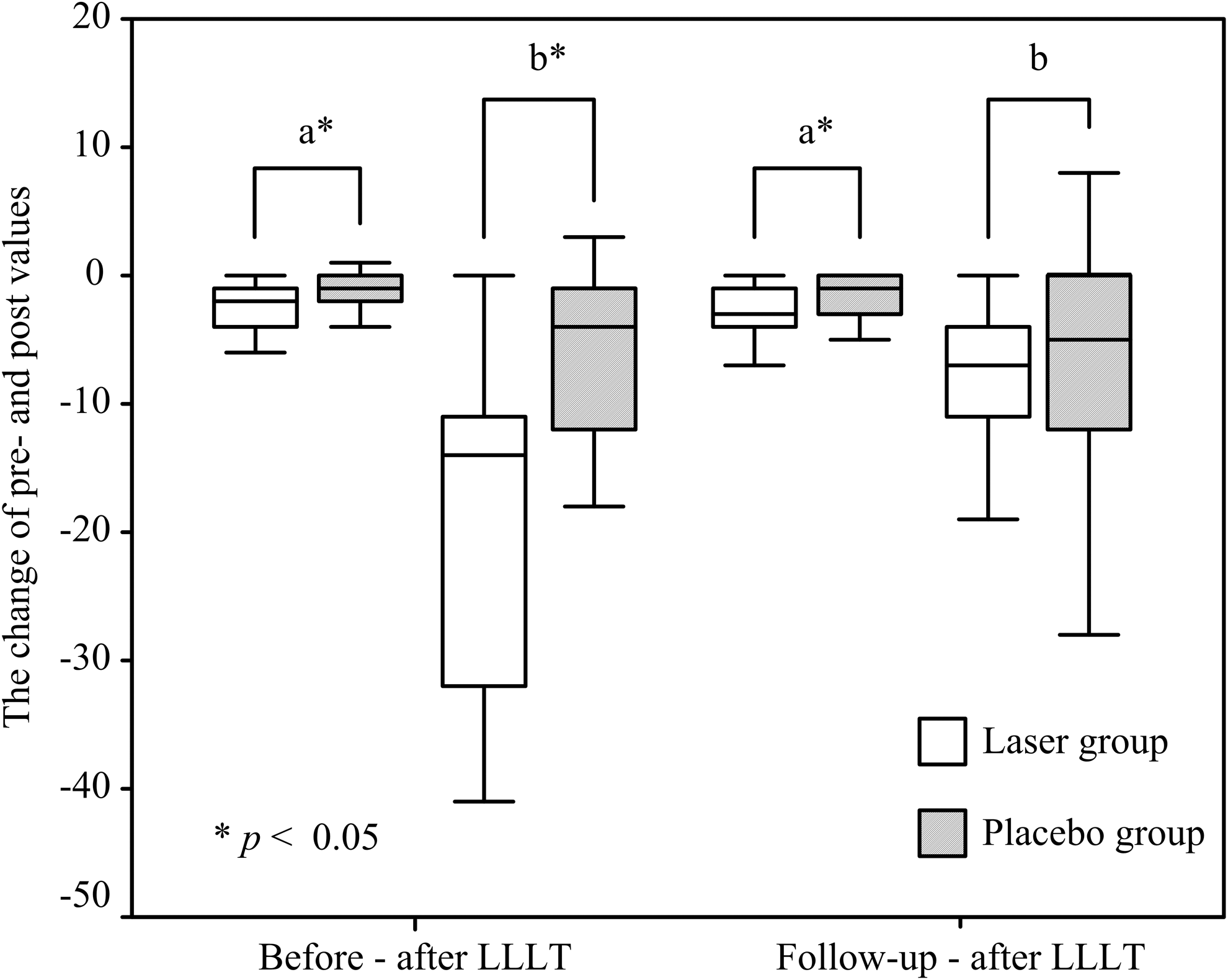
The changes in visual analog scale (VAS) (a) and Quick Questionnaire for Disabilities of the Arm, Shoulder, and Hand (Quick DASH) (b) in both groups.
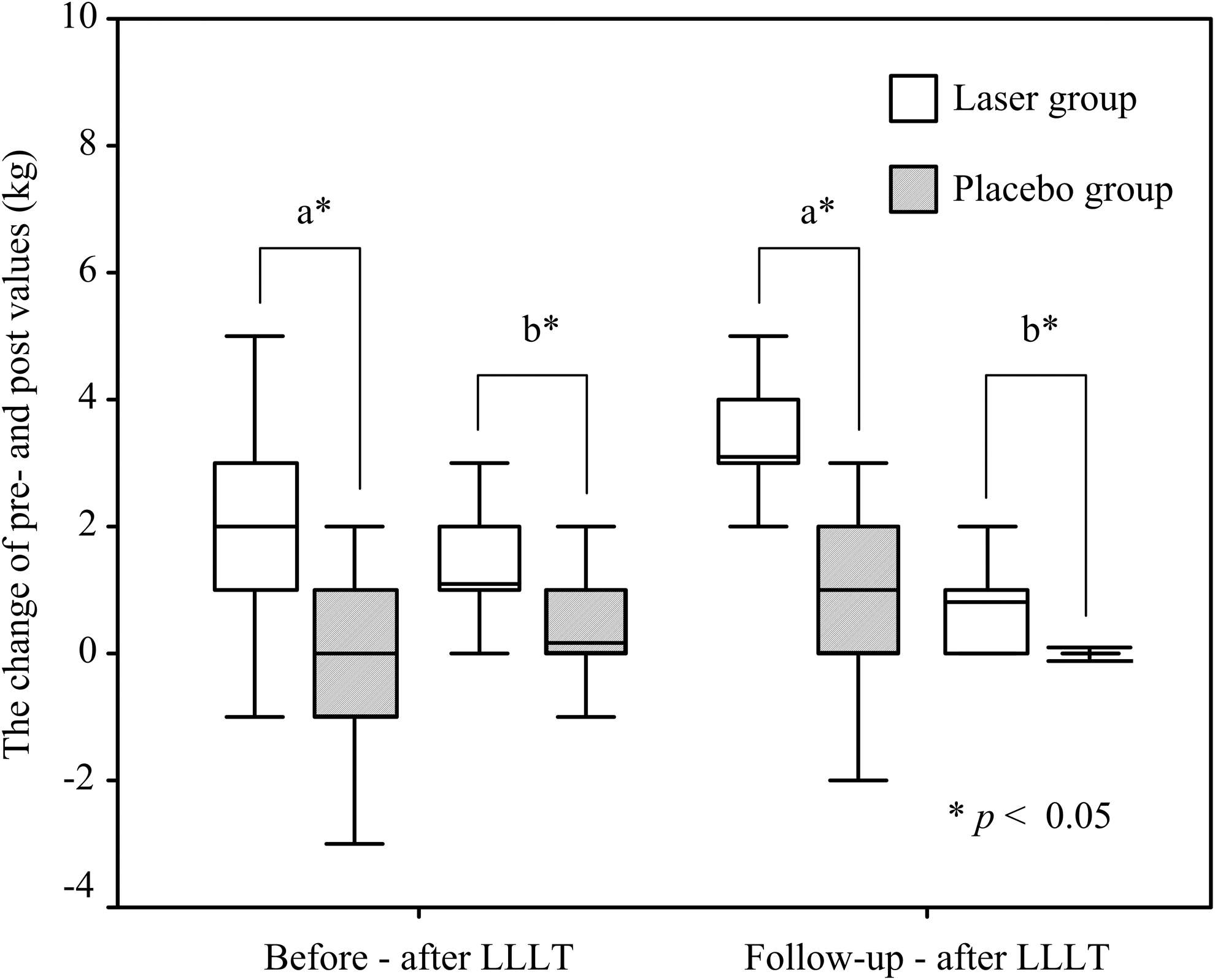
The changes in the hand grip strength (a) and finger grip strength (b) in both groups.
VAS, visual analog scale; Quick DASH, Quick Questionnaire for Disabilities of the Arm, Shoulder, and Hand.
Laser group vs. placebo group, p<0.05.
Before vs. after treatment, p<0.05.
After treatment vs. follow-up, p<0.05.
Follow-up vs. before treatment, p<0.05.
Before the treatment, no significant differences in the percentages of absent FL and detectable CB were observed between the groups, as shown in Table 3. In the laser group, an FL was still present in 24 participants after treatment and at the follow-up. Only one participant exhibited an absence of FL, as depicted in Fig. 2. Similarly, in the placebo group, FLs remained visible in all of the participants after treatment and at the follow-up. Therefore, we observed no significant differences between the groups regarding absent FL percentage after treatment (laser group: n=24, 96%; placebo group: n=25, 100%) and at the follow-up (laser group: n=24, 96%; placebo group: n=25, 100%).
The between-group differences in detectable CB were statistically significant (p<0.05), and the laser group exhibited a greater increase in detectable CB after treatment and at the follow up compared with that of the placebo group. After treatment, detectable CB was observed in 76% (n=19) of the laser group participants and 32% (n=8) of the placebo group participants. At the follow-up, these figures increased to 92% (n=23) for the laser group and 48% (n=12) for the placebo group. Therefore, a group comparison between the results of the post- and follow-up treatments indicated that LLLT was correlated with a significant increase in the percentage of participants with detectable CB (p<0.05).
Discussion
We employed a diode laser with a wavelength of 830 nm, an energy density of 9.7 J/cm2, and an average power of 60 mW in this study. Diode lasers are commonly used in clinical and household settings. Studies on rats have also revealed that administering 830 nm LLLT using a diode laser accelerated the bone healing process and initiated a positive bone-tissue response. 18 –20 Renno et al. administered 830 nm LLLT using a diode laser at a dose of 10 J/cm2 to proliferating osteoblasts on a glass-ceramic scaffold, which reduced the osteoblast cell growth. 21 The photobiological effects of LLLT using a diode laser were determined by the wavelength and the dose. In this study, 830 nm LLLT using a diode laser (9.7 J/cm2) was used to treat CBFs in wrists and hands, and the experimental results indicated that the treatment provided effective pain relief and improved the muscle strength and functional ability of patients.
The mechanism by which LLLT relieves the pain of bone fractures remains unclear. 11,22 Da Cunha et al. argued that analgesia was caused by the decreased synthesis of precursors, and suggested that LLLT penetrated soft tissue in vivo to decrease prostaglandin (PGE2) levels and inflammation. 23 Despite the lack of knowledge on the exact mechanism by which it operates, LLLT is often used in clinical settings because it can relieve pain. Brosseau et al. demonstrated that LLLT relieved pain and exerted beneficial effects on acute and chronic musculoskeletal diseases. 24 Bjordal et al. used LLLT to treat patients with degenerative arthritis for a brief period, and then compared the results with the outcomes of control patients who received either electrical stimulation or no treatment; 25 they observed that LLLT produced a pain-relieving effect for up to 4 weeks after treatment. The effects of LLLT are more satisfactory than those of other treatment modalities.
This study revealed that the pain of acute fractures was significantly reduced after LLLT. A significant difference in the VAS scores was observed in both the laser and placebo groups after treatment and at the follow-up, compared with those at the baseline. However, only the laser group demonstrated significant improvement in the Quick DASH results and hand and finger grip strength measures after treatment. Beneficial effects, such as bone tissue recovery and pain relief, resulted from irradiating the CBF site with LLLT. Improvements in hand functional ability and hand or wrist strength might be attributable to these results.
A significant increase in the percentage of detectable CB was observed among the laser group participants after treatment (76%), and a similar increase was also detected at the follow-up (92%). This effect might have been caused by an increase in metabolism and improved blood circulation surrounding the fracture site, which resulted from LLLT. Several studies have also reported that LLLT affects bone cell proliferation, 5 –7,26 and increases intracellular calcium by activating adenosine triphosphate. 27 In their study on Wistar rats, Nicola et al. reported that LLLT accelerated the process of resorption after a fracture had occurred, and initiated bone formation at the femurectomy site. 28 Similarly, Trelles and Mayayo observed that LLLT administered to the fractured tibias of rats facilitated vascularization and formation of osteocytes. 29 Studies in which the effect of LLLT on human bone fractures is investigated are lacking, but we believe that administering LLLT soon after a CBF occurs can improve callus formation. In addition, the radiographic records for the laser group indicated that most of the fracture lines were not healed. Although LLLT might increase the activity of osteoblasts after a fracture occurs, this could not be easily determined based on the gross and radiographic images.
One prior study revealed that LLLT produces a stimulatory effect on osteoblasts in contrast to the inhibitory effects of high-energy laser irradiation. 30 Hamajima et al. studied the effects of 830 nm LLLT administered at the early stage of fracture healing and observed that the osteoglycin gene expression in osteoblasts was stimulated, and that cellular proliferation and differentiation were promoted. 31 Barbos Pinheiro et al. administered LLLT to rats 5 days after a surgical fracture was created, and observed that bone volume and osteoclast activity areas significantly increased compared with those of the control group. 32 In addition, they observed that the osteoblast activity area enlarged within 15 days after the surgery. Trelles and Mayayo also administered LLLT every other day to rats to treat fractured tibias, and observed that bone cells were regenerated within 24 days after the surgery. 29 In another study, Nicola et al. used a laser to treat rats with fractured femurs, 28 but did not observe the formation of bone cells after 8 days of using laser irradiation. Bashardoust Tajali et al. conducted a meta-analysis to examine the effects of LLLT on bone healing in animals, 5 and suggested that at least 14–21 treatment sessions of LLLT were necessary to yield beneficial effects. 5 However, we observed that 10 sessions of LLLT facilitated bone healing and pain relief, and improved hand functional ability and strength in human patients.
The positive effects of LLLT in treating CBF have yet to be conclusively proven. The results of this study are based on a specific set of parameters of LLLT (830 nm, average power 60 mW, peak power 8 W, 10 Hz, 600 sec, and 9.7 J/cm2; 600 sec per fracture site) administered to CBFs. Following the methods used by Bjordal et al., we used a treatment wavelength of 830 nm and a dosage of 9.7 J/cm2. 11 The selection of the LLLT frequency varied between treatments. In clinical use, administering pulse waves at a frequency of 2–10 Hz is recommended. 9 However, the appropriate frequency for inducing biological effects has still not been conclusively determined. The specific dose of LLLT used in this study to treat CBFs yielded positive results. However, this study is limited by the small sample size; many patients were disinclined to participate because of the possibility of receiving placebo treatments. Conducting further randomized controlled trials is necessary to investigate the influence of LLLT using various parameters (e.g., wavelengths, dosages, frequencies) on bone healing after a CBF occurs.
Conclusions
LLLT provided pain relief, ameliorated symptoms, and induced healing effects, including improvements in physical function and grip strength in the wrist or hand, after the occurrence of a CBF. The therapeutic effects of LLLT on human bone healing have not been well established, possibly because of insufficient radiographic evidence. Further studies are required to validate the findings of this study.
Footnotes
Author Disclosure Statement
No competing financial interests exist.