
Abstract
Introduction
From July 2003 to August 2007, 87 LDH patients underwent PLDD at our institution with an Nd:YAG laser (SLT Company of Japan), and among them, 42 cases were followed up continuously for >3 years. The present study was initiated to evaluate the efficacy of PLDD in the treatment of LDH and identify its relationship with age.
Methods
The entry criteria were as follows: (1) low back pain associated with lower extremity pain, (2) focal signs showing nerve root compression, (3) clinical manifestation and imaging diagnosis being consistent, (4) imaging findings showing one or more lumbar disc protrusions with or without disc extrusion, and (5) no responsiveness to conservative treatment for at least 3 months or having a relapse. Patients with free herniated disc, >50% reduction of disc height, bony spinal stenosis, hypertrophy of ligamentum flavum, or lateral recess stenosis were excluded.
A total of 42 patients met the study criteria, including 25 males and 17 females with an mean age of 45.2 years (range, 19–71 years). All the patients were diagnosed as having LDH combined with various medical history, physical examination, and imaging findings: L4/5 in 5 cases, L5/S1 in 4 cases, L3/4 associated with L4/5 in cases, L4/5 associated with L5/S1 in 26 cases, and multiple LDH (L3/4, L4/5, L5/S1) in 5 cases. The symptom duration ranged from 3 months to more than >6 years. Tthe patients were divided into two groups according to age, 19 cases in the ≤45-year-old group and 23 cases in the >45-year-old group.
Surgical technique
The patient was placed in a lateral position with the affected side up. Preoperatively, we used C-arm radiograph to confirm the surgical disc and select a skin entry site 8–12 cm lateral from the midline). After routine disinfection and sterilization, the skin and subcutaneous tissue were infiltrated with a local anesthesia (1% lidocaine, 0.5 mL).
Under fluoroscopic guidance, an 18-gauge needle was then inserted into the affected disc from a dorsolateral direction through the “safe triangle.” The needle position was made midway and parallel to the endplates, with the needle tip past approximately one third of intervertebral space (lateral view) and located at the midline (anteroposterior view) (Fig. 1). Then, a 400 μm optical fiber with the proximal end connected to a Nd:YAG laser (1064 nm) was inserted into the hollow needle, and the distal part of the fiber extending past the needle tip by 5 mm. We began the laser procedure after confirming the correct needle position again under fluoroscopy. The laser power was set at 13.5 W with pulses of 1 sec and pauses of 1 sec, and the total amount of laser energy delivered was 500–800 J for each treated disc.
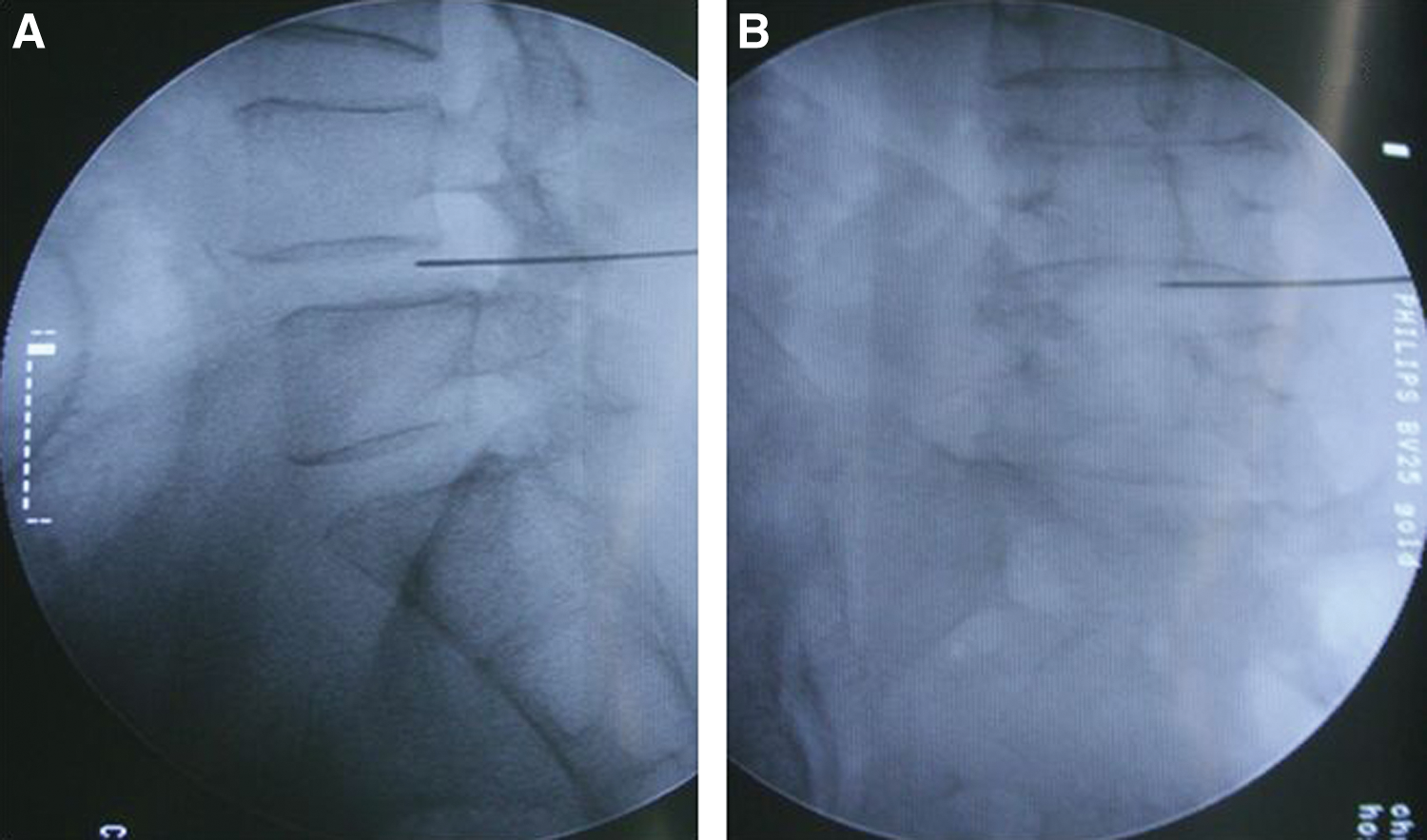
The proper needle position was made in midway between the endplates and parallel to the disc axis, with the needle tip past approximately one third of the intervertebral space on the lateral view
For six affected discs which had lost ∼30% of disc height, we chose two or more sites in the annulus fibrous to deliver laser energy so as not to result in thermal injury on adjacent cartilage endplates. For four affected discs with greater disc herniation (≥6 mm), we withdrew the treating needle three times during the laser procedure in order to be as posterior as possible to ablate the herniated part of the disc, but making sure that the needle tip was always past the annulus. Patients' intraoperative response should be monitored strictly. Because of the use of local anesthesia, the surgeon could communicate with the conscious patient, then adjust the laser parameters such as laser power, pulse duration, and total amount of energy, appropriately.
After the PLDD, bed rest was recommended for 2 h. Patients could return to sedentary work 7 days later, and all patients were encouraged to wear a bandage for 3 weeks. Antibiotics were not required after treatment.
Evaluation criteria
The patients were evaluated with Japanese Orthopaedic Association (JOA) Scores before and after surgery. Follow-up visits were scheduled at 1, 3, 6, 12, 24, and 36 months after the PLDD. Follow-up results were graded as excellent, good, fair, and poor according to improvement rate (IR) of JOA scores (Table 1). The highest lumbar JOA score is 29; therefore the IR can be calculated by the following equation:
IR, improvement rate; JOA, Japanese Orthopaedic Association.
Statistical analysis
The improvements of favorable outcomes among different follow-up time and the difference in favorable outcomes between the two groups were analyzed by Fisher's Exact test. All p values of<0.05 were considered statistically significant.
Results
Eighty affected discs in 42 patients were treated successfully with no adverse reactions and complications in this study. All of the patients were followed up continuously for >36 months. Postoperative MRI of the lumbar spine showed a more or less retraction of the herniated discs in 10 cases (Fig. 2). Based on the improvement rate of JOA scores, the excellent or good improvement of the 42 patients at 1-, 3-, 6-, 12-, 24-, and 36-month follow-up were, respectively, 19 (45.24%), 28 (66.67%), 30 (71.43%), 32 (76.19%), 34 (80.95%), and 32 (76.19%). The favorable (excellent or good) outcomes significantly improved from 45.24% at 1 month follow-up to 66.67% at 3-month follow-up (p<0.05). There was no significant difference in favourable outcome at 3-, 6-, 12-, 24-, and 36-month follow-up (p>0.05).
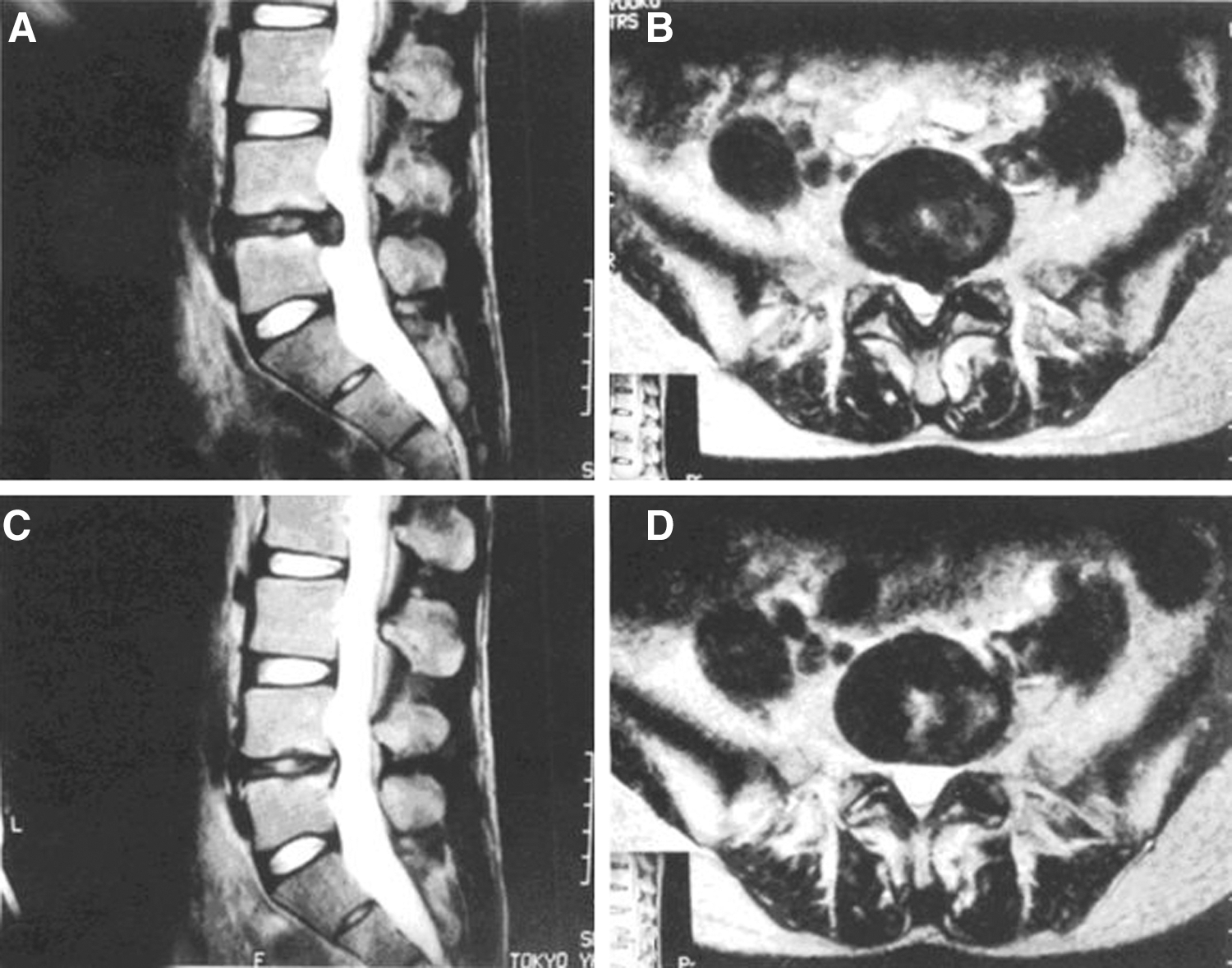
Preoperative MRI of lumbar spine showed L4/5 herniated
The preoperative lumbar JOA scores in the two groups were not different (p>0.05), and no between-group differences were noted in favorable outcome at the same follow-up time (p>0.05) (Table 2).
PLDD, percutaneous laser disc decompression.
Discussion
After the beginning of the 21st century, the rapid development of minimally invasive spine surgery has provided more and more surgical options for surgeons and patients. 8 Among the alternative therapies, PLDD has proven to be an ideal treatment of LDH. 3 –7 With continuous researching, this technique is becoming more and more mature and is now widely used in all over the world.
To our knowledge, this is the first report of continuous follow-up results over 3 years regarding PLDD in the treatment of LDH. According to the follow-up results, we can design a curve to show the variation tendency of the PLDD efficacy, and then provide identifiable ground for further treatment. In this study, the favorable outcome significantly improved from 45.24% at 1-month follow-up to 66.67% at 3-month follow up. Patients improved significantly in a short time after the PLDD, which can be explained by two primary factors as follows.
Laser irradiation vaporized a small amount of nucleus pulposus (NP) in the affected disc, which resulted in an immediate reduction of the intradisc pressure, thus resulting in gradual withdrawal of disk compression on the nerve root. 9 A series of tests made by Choy 10 –12 proved that a small reduction of the volume of NP could result in a marked fall (>50%) of intradisc pressure. Decompression in the herniated disc could cause more or less retraction, 13 but postoperative imaging findings such as in Fig. 2 of this article were not common in reality (no more than 20%).
In addition to treating nerve root compression like other minimally invasive techniques, PLDD also reduced the inflammatory factors with the generation of heat by laser irradiation. Radiculopathy has been attributed to the production of chemical factors such as phospholipase A2 (PLA2) and prostaglandin E2 (PGE2) that resulted from the degenerative discs. 14,15 Iwatsuki 16 proved by animal experiment that the levels of chemical factors were significantly reduced and the nerve conduction velocities were significantly faster after laser radiation.
Comparing the follow-up results at 6 and 3 months, the favourable outcome still improved to a certain extent, but the difference was not significant. The variation tendency of the PLDD efficacy shows that it flattens out gradually at 6 months after PLDD. Qi 17 studied the histopathological changes of discs treated with PLDD and found that it would take 3 months for postoperative repair of the treated discs and no histopathological changes discovered after 3 months. Research by Choi 18 demonstrated that laser irradiation resulted in localized irreversible volume reduction in NP which was thought to be responsible for the long-term effects of PLDD. It provided an important information that worrying about a low success rate in the short term (<3 months) after PLDD is not necessary. If patients have to receive another invasive therapy because PLDD was not effective, we usually suggest it should take place no less than 6 months after PLDD.
Because the water content of NP decreases with age and PLDD is based on the concept that the intervertebral disc is a water-filled balloon, it is usually believed that PLDD is more effective in younger patients than in older patients. But this hypothesis remains to be confirmed by basic and clinical science studies. In this study, there was no significant difference in PLDD efficacy of the two groups of different ages. We analyze that the reasons might be as follows. (1) Strict respect for entry criteria, which is one of the most important premises to achieving a favourable outcome for patients of different ages. Overemphasizing the selection criteria certainly will narrow the indications for PLDD. However, we should know that PLDD, as is the case with all the alternative therapies, is not the gold standard for LDH, and that no technique is a panacea for all lumbar disc pathology. (2) Individualized surgical operations according to each patient's own condition and laser dosages vary with each case. 19 Readers can review the “Surgical technique” part of the Methods section. Laser parameters are very important for treatment outcome, so the surgeon should be perfectly familiar with the performance of laser parameters. From this perspective, PLDD is considered an experimental procedure. (3) Too few cases in this study may be a potential cause for the “negative result.” The mean age of our cases was 45.2; therefore, we chose 45 years of age as the dividing line to identify the relationship between PLDD efficacy and age. Too few cases may result in an imbalance of age distribution. Obviously, we need to gather more cases as time go by to further study this problem.
Conclusions
The clinical outcome with PLDD improved significantly within 3 months, and can be maintained at a high level over 3 years. The efficacy of treatment with PLDD is fairly good for both selected younger and older patients.
Footnotes
Acknowledgment
The authors thank Nurse Lihua Huang for establishing a detailed memoire that was used to follow up patients.
Author Disclosure Statement
No competing financial interests exist.