
Abstract
Introduction
Because of the high risk for development of invasive carcinoma, these patients are often treated surgically by wide excision of the involved areas. This can lead to significant morbidity and compromised quality of life. 3,4
We present a patient with PVL and superficially invasive carcinoma that was treated by a more conservative approach using a carbon dioxide (CO2) laser and close follow-ups, which resulted in decreased morbidity and good-long term quality of life as compared with that of wide surgical excision.
Case Report
A 46-year-old male presented to the oral medicine clinic at the University of California, San Francisco (UCSF) in January 2000 for evaluation of changes affecting his tongue. He was status post allogeneic bone marrow transplant for chronic lymphocytic leukemia, which had been diagnosed and treated in 1994. Following the transplant, he had developed graft-versus- host disease (GVHD) 5 affecting the skin of the neck and abdomen, as well as the oral cavity.
In July 1999, he had had bilateral tongue biopsies at the City of Hope National Medical Center in Los Angeles, which showed invasive squamous cell carcinoma. He underwent right and left partial glossectomy procedures in August 1999. Frozen sections intra-operatively showed carcinoma in situ extending to the margins of the excised tissue, and further tissue was excised, which also showed carcinoma in situ. According to the medical records, as the changes were extensive and margins were likely to show dysplasia or carcinoma in situ, no further tissue was excised during this procedure.
After this procedure, the patient sought consultation with other physicians regarding treatment of the residual extensive tongue lesions. He was given a recommendation of external beam radiation treatment at St. John's Health center department of radiation oncology, and a recommendation of a complete glossectomy at the University of California, Los Angeles.
The patient refused both of the offered treatment options and sought consultation with Dr. Silverman at UCSF, seeking a treatment option that would forgo radiation therapy, and save his tongue. Also, he was scheduled to start a clinical trial of Onyx-15, an experimental oncolytic adenovirus (Onyx Pharmaceuticals Inc., South San Francisco,CA) at MD Anderson Cancer Center in February 2000, for control of oral leukoplakia. 6
At the time of his first visit at UCSF in January 2000, his medications included prednisone, tacrolimus, mycophenolate mofetil, and trimethoprim-sulfamethoxazole.
He reported having been a heavy smoker for ∼15 years (from 15 to 30 years of age) although he had not smoked in 15 years. He had no history of alcohol use and no known drug allergies. He also reported a strong family history of cancer. His father had had prostate, laryngeal, and colon cancer, his mother had had breast cancer, and a brother had had Hodgkin's lymphoma.
On examination, extensive verrucous and nodular changes were seen on the tongue involving almost the entire oral tongue mucosa. The patient also had some scarring from his previous partial glossectomy procedures. His tongue was symptomatic and he had some degree of compromised function (speech and eating). Multiple areas were toluidine blue positive. The initial clinical impression was widespread PVL, and invasive carcinoma needed to be ruled out. The patient was oriented to the findings, and to management approaches.
He returned for a re-evaluation in August 2000, after completion of the Onyx-15 adenovirus rinse study, as there was no improvement in his oral condition, with his closing biopsy showing superficial squamous cell carcinoma. On examination, the clinical findings were unchanged from his previous visit. The clinical impression remained extensive PVL, and invasive cancer needed to be ruled out.
An MRI was ordered to evaluate for deeper invasion and staging. The MRI showed “no evidence for deep space masses or adenopathy that would suggest deeper involvement by known superficial tongue carcinoma.” The final diagnosis was PVL with severe dysplasia and superficially invasive squamous cell carcinoma.
The treatment options were discussed with the patient. He had previously refused a complete glossectomy and he again refused radical surgery. The more conservative option of serial laser procedures was discussed further. These were to be done on an outpatient basis, using local anesthesia, with careful clinical evaluation at each step, and biopsy at each step. The patient was advised that if invasive carcinoma was diagnosed, or developed at a future time, he would need more extensive surgery at that point.
He was scheduled for outpatient procedures involving serial biopsy and excision, and/or vaporization, of the affected areas using a CO2 laser (wavelength 10.6 μm). All laser procedures were performed using local anesthesia consisting of 2% xylocaine with 1:100,000 epinephrine. A CO2 laser set on continuous wave mode (range 4–10 W) was used for vaporization as well as excision of suspicious tissue for biopsy. Biopsies were also performed using dermatologic punch instruments. All procedures were performed by or under the direct supervision of Dr. Silverman or Dr. Chainani-Wu. Vaporization of leukoplakia was performed with margins extending to clinically normal tissue if possible, or limited to a surface area that would result in satisfactory healing without too much postoperative discomfort, and was extended to a depth of at least 5 mm into the muscle. As the final step, the laser was used in a defocused mode over the surgical site. All operative sites were left to heal by secondary intention and without any suturing.
Figures 1A–C show the baseline appearance of the tongue in October 2000, at which time the first laser procedure was performed. The patient had been tapered off immunosuppressant medications by this time. Two punch biopsy specimens measuring 0.5×0.5×0.8 cm were taken from the right lateral tongue, from the most suspicious areas, which were also toluidine blue positive. The CO2 laser was set to a power of 10 W. Vaporization of leukoplakia on the right lateral tongue down to the muscle was completed on two sites, covering an area of ∼1.2 cm each (Fig. 2). There were no postsurgical complications. The patient was prescribed penicillin and hydrocodone with acetaminophen. Subsequent pathological examination of excised tissue showed “severe dysplasia, suggestive of superficially invasive squamous cell carcinoma.” The patient tolerated the procedure well with mild postoperative discomfort, which was well controlled with analgesics.
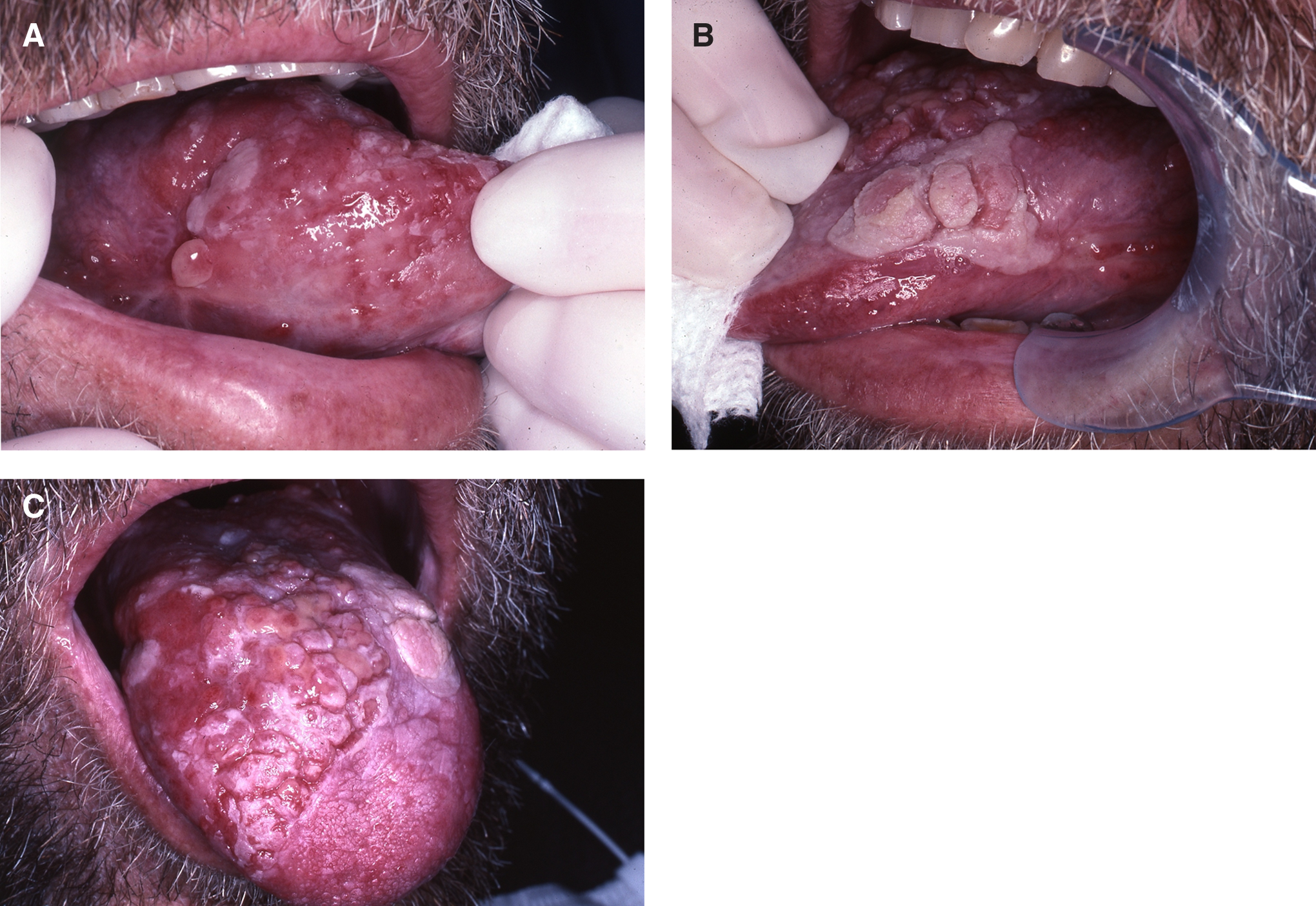
At initial presentation in 2000, extensive verrucous, nodular changes were present involving the
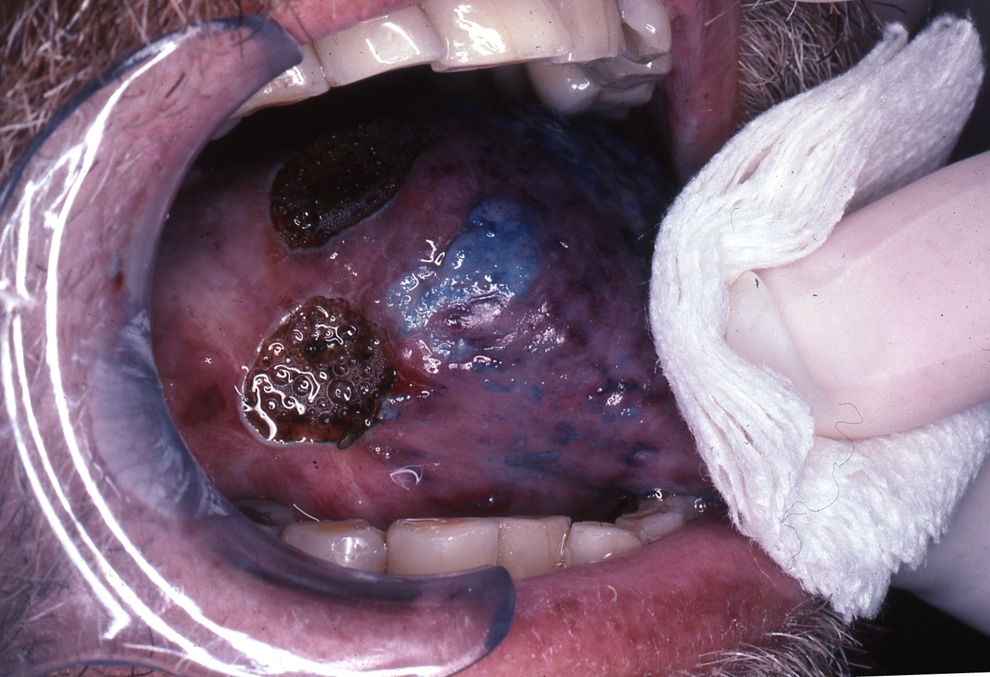
The first surgical procedure of the planned serial laser surgeries was performed on the right lateral tongue, in October 2000. Immediate postoperative view is shown here.
He returned to the clinic 2 weeks later, at which time the changes on the left lateral tongue were treated. A biopsy was performed, and vaporization of leukoplakia on the left lateral tongue, down to the muscle and an area of ∼3×2.5 cm was completed. (Fig. 3A and B). Previous biopsy sites appeared to be healing well, and the patient reported no significant pain or discomfort. Histopathologic evaluation of the biopsy specimen showed “severe dysplasia and possible superficial invasion.”

The procedures were continued, treating the affected areas of the tongue section by section at each visit. The sites to be treated were prioritized based on signs and symptoms. The patient tolerated the procedures well and complained of minimal postoperative discomfort; therefore, larger areas could be treated at a given visit. By February 2001, a procedure to remove changes on the dorsum of the tongue, with vaporization down to the muscle, was completed, covering an area of ∼4 cm long and 4 cm wide at the posterior aspect tapering toward the anterior aspect (Fig. 4A and B). The specimen submitted for biopsy (incisional) revealed “moderate dysplasia and chronic ulcer.” Over the following months and years the patient was followed closely, and laser surgical procedures were performed a total of 22 times, most recently in July 2007. After each procedure, the surgical site was carefully assessed for complete healing at postoperative visits by inspection, palpation, and the use of toluidine blue staining. The tongue showed a definite improvement in appearance following each surgical procedure.
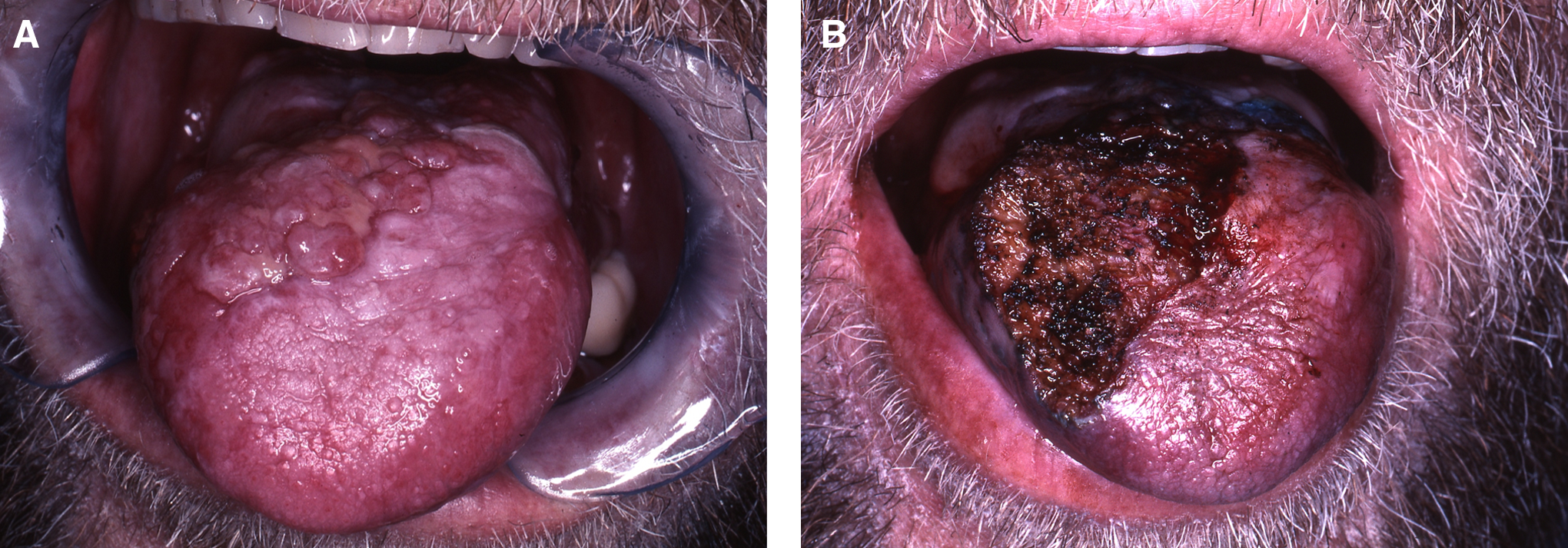
By the time the last surgical procedure was performed in 2007, the patient's oral mucosa appeared significantly more normal, all areas were soft on palpation, and toluidine blue was negative. At the most recent follow up, in January 2012, the tongue continued to be stable and asymptomatic (Fig. 5A–C). The patient has not had any speech or other functional impairment resulting from the multiple laser procedures, as scarring has been minimal. He has been advised that he will need lifelong periodic follow-ups to monitor for any recurrences. His quality of life is very good, and no other malignancies have occurred up to the last follow-up visit.

The appearance of the oral mucosa appears significantly improved at the time of these photographs in 2010, and all areas were soft on palpation and toluidine blue negative. In addition, there was no speech or functional impairment following the laser procedures.
Discussion
Wide surgical excision of oral PVL lesions and superficially invasive carcinoma can lead to significant long-term morbidity, particularly when these lesions are extensive. Speech difficulties and difficulty in swallowing often follow a partial glossectomy and are more severe following a complete glossectomy. Wide resection of other areas of the oral cavity can also result in a decrease in quality of life, as well as anxiety and depression. 3 4,7 –9
In the surgical management of leukoplakia, the use of CO2 laser allows the consideration of a more conservative approach. Advantages of CO2 laser include a bloodless field providing better operative visibility, precise control, and ease of use. However the main advantage of the CO2 laser that impacts long-term morbidity is the decreased postoperative scarring as compared with use of a scalpel. 10,11 This conservative approach also avoids the need for grafting, and conserves function. 12 –14
At this time, the underlying mechanisms to account for the differences seen clinically in wound healing between CO2 laser and scalpel wounds have not been well elucidated; however, some differences in the molecular processes involved have been described, such as differing tissue concentrations of transforming growth factor beta and fibroblast growth factor. 15
In addition to availability of a CO2 laser, the clinical ability to accurately evaluate the lesions of PVL is essential in order to use this more conservative management approach. Clinical evaluation of the lesion by inspection, palpation, and toluidine blue staining, as well as histopathologic examination of biopsies from the most suspicious areas of the lesions, is necessary. Multiple biopsies may be necessary to make an accurate baseline assessment.
This conservative approach is not appropriate for management of invasive cancer. Therefore, if invasive cancer is present at baseline, or develops during follow-up, the cancer would need to be staged and treated accordingly, using wide surgical excision, and if necessary radiation and chemotherapy. Patients with PVL need close follow-up not only because the existing lesions have a risk for malignant transformation but also because there is a risk for recurrence of previously excised lesions as well as development of new lesions over time. At each follow-up, the clinical evaluation helps determine the need for biopsy or surgical removal at that time point. The goal of treatment is to prevent progression to carcinoma or to diagnose malignant transformation at an early stage. Unfortunately, there are no accurate markers that clearly define safe or adequate margins.
Conclusions
This case illustrates the value and benefit of a more conservative treatment approach as compared with wide surgical excision for PVL, which may demonstrate areas of superficially invasive carcinoma. This approach requires greater skills in clinical evaluation of oral premalignant or malignant changes, and training and experience is required to develop these skills. Because of the decreased long-term morbidity and improved quality of life, it is a valuable treatment option for patients with PVL.
Footnotes
Author Disclosure Statement
No competing financial interests exist.