
Abstract
Introduction
Laser technology 2 and ozone application 3 are alternative approaches to the elimination of microorganisms from a root canal system. Ozone (O3) is a powerful oxidizing agent 4 that has been used in the water industry to eliminate bacteria. Its properties could also be useful in dentistry. 5 Ozone is currently being discussed in dentistry as a possible alternative antiseptic agent. Recent investigations have reported antimicrobial effects on oral pathogens from both gaseous and aqueous forms of ozone. 5 Aqueous ozone has been shown to be a powerful antimicrobial agent against bacteria, fungi, protozoa, and viruses. This suggests that oral microorganisms might be inactivated by aqueous ozone at different doses. Ozone in liquid form shows the lowest toxicity when compared with all known antiseptics. 6 These properties indicate that aqueous ozone could be useful in dentistry. The use of aqueous ozone for the treatment of endodontic infections has also been suggested by some authors. 7,8
Laser systems may have antimicrobial effects that could aid in the reduction of bacteria in root canals. 9 Recent studies 9 –12 have investigated the disinfecting ability and the safe availability of different types of lasers. For example, the efficacies of KTP (a type of laser with a frequency doubled that of Nd:YAG) and Er:YAG lasers, have been shown to be useful for photothermal disinfection in root canals. In light of this information, this in vitro study was performed to assess the antibacterial effects of two different types of lasers and aqueous ozone in human root canals infected by Enterococcus faecalis.
Materials and Methods
Eighty freshly extracted single-rooted human mandibular premolar teeth without caries or restorations were selected. Informed consent was obtained from the patients before the research began, and the study was approved by the Local Ethics Committee on Human Research of Cumhuriyet University (April 10, 2012). Following the extractions, digital radiographs were taken from buccal and approximal directions to determine the number and morphology of the canals.
Following the removal of surface remnants, the extracted teeth were kept at +4°C in a 0.9% saline solution until experimentation. The coronal portions of the teeth were removed just below the cement–enamel junction by using sterile diamond discs under cool water to obtain standardize lengths of 14–16 mm for each root. Then, the root canals were accessed with #15 K-File hand tools, and the paths of the root canals were determined. A file was inserted into each root canal until it became visible at the apical foramen. Then, the file was withdrawn 1 mm and the working length was established. The root canals were respectively instrumented by using ProTaper (Dentsply, Tulsa Endodontics, OK) rotary Ni-Ti instruments SX, S1, S2, F1, F2, and F3 that were mounted on an electric handpiece by the crown-down technique. The canals were irrigated with 1 mL of 5.25% solution of NaOCl after the use of each file. The root canals were finally irrigated with 17% ethylenediaminetetraacetic acid (EDTA), 5.25% NaOCl, and distilled water for 5 min to remove the smear layer, and then all of the samples were dried with paper points. Vials in which the samples had been stored were placed in an autoclave and sterilized for 20 min at 121°C. A threefold nail polish was applied on all root surfaces, including the apical foramina. The vials' rubber caps were also sterilized using ethylene oxide.
Microbiologic procedures
E. faecalis (ATCC 29212) strains were revived in the liquid nutrient media (brain-heart infusion broth, Acumedia Manufactures, Inc., Lansing, MI) and were incubated at 37°C for 24 h. Prior to each experiment, 0.5 McFarland turbidity was set with a Kristal Spec™ device, and McFarland standard number 0.5 was used to improve the blood agar plates in order to obtain the bacterial growth in 1.5×108 colony-forming units (CFU/mL). The value of 10 μL of bacterial culture was transfered to the mechanically expanded lumen of the root canal using a sterile micropipette and then kept at 37°C for 24 h. In order to control bacterial growth, sterile paper points (Dentsply, Maillefer) were placed in the root canals inoculated with bacteria. The paper points were in place for 5 min and soaked with the broth. The paper points were then placed in sterile Eppendorf tubes containing 0.5 mL brain–heart infusion broth (Merck 1.13825). After 15 min, 50 mL of liquid medium was taken with a sterile micropipette from Eppendorf that mixed with vortex and inoculated onto solid media (blood agar plates), which split before and after the disinfection.
Control and experimental groups
NaOCl (negative control)
Infected root canals were irrigated for 3 min with 5.25% NaOCl.
Er:YAG laser
The root canals were irradiated at 2.0 W (100 mJ, 20 Hz) with an Er:YAG laser device (Smart 2940D, DEKA, Calenzano, Italy) emitting pulsed infrared radiation at a wavelength of 2940 nm. The Er:YAG laser beam was delivered through an articulated arm. A handpiece was used in the noncontact and focused mode. The root canals were irradiated in a sweeping fashion with a water flow of 5 mL/min for 3 min by the Er:YAG laser.
KTP laser
The root canals were irradiated at 2.0 W (100 mJ, 20 Hz) with a KTP laser (SMARTLITE D, DEKA, Calenzano, Firenze, Italy). Throughout the laser treatment, the fiber tip (diameter of 200 μm) was applied with a spiral motion, starting 1 mm short of the apex and then moving coronally for 5 sec, interleaved with 15 sec recovery intervals for each irradiation. This process was repeated nine times (total time: 3 min).
Aqueous ozone
Aqueous ozone was obtained with a custom-made ozone generator (TeknO3zone, Izmir, Turkey
Bacterial evaluation
A sample counting of bacteria E. faecalis (ATCC 29212) was performed to ensure standardization, and the examples with CFU values<1.5×108 CFU/mL were excluded. After the irrigation, the logarithms of the CFU counts were calculated. The data were statistically analyzed with one-way analysis (SPSS 14.0) of variance (ANOVA) and Tukey post-hoc (0.05).
Results
The mean±standard deviation together with their statistical comparisons and median and bacterial reduction (%) values that were obtained from all groups are shown in Table 1. Cross-sectional images of E. faecalis on blood agar plates with the samples obtained from root canals before and after irrigation are shown in Figure 1.
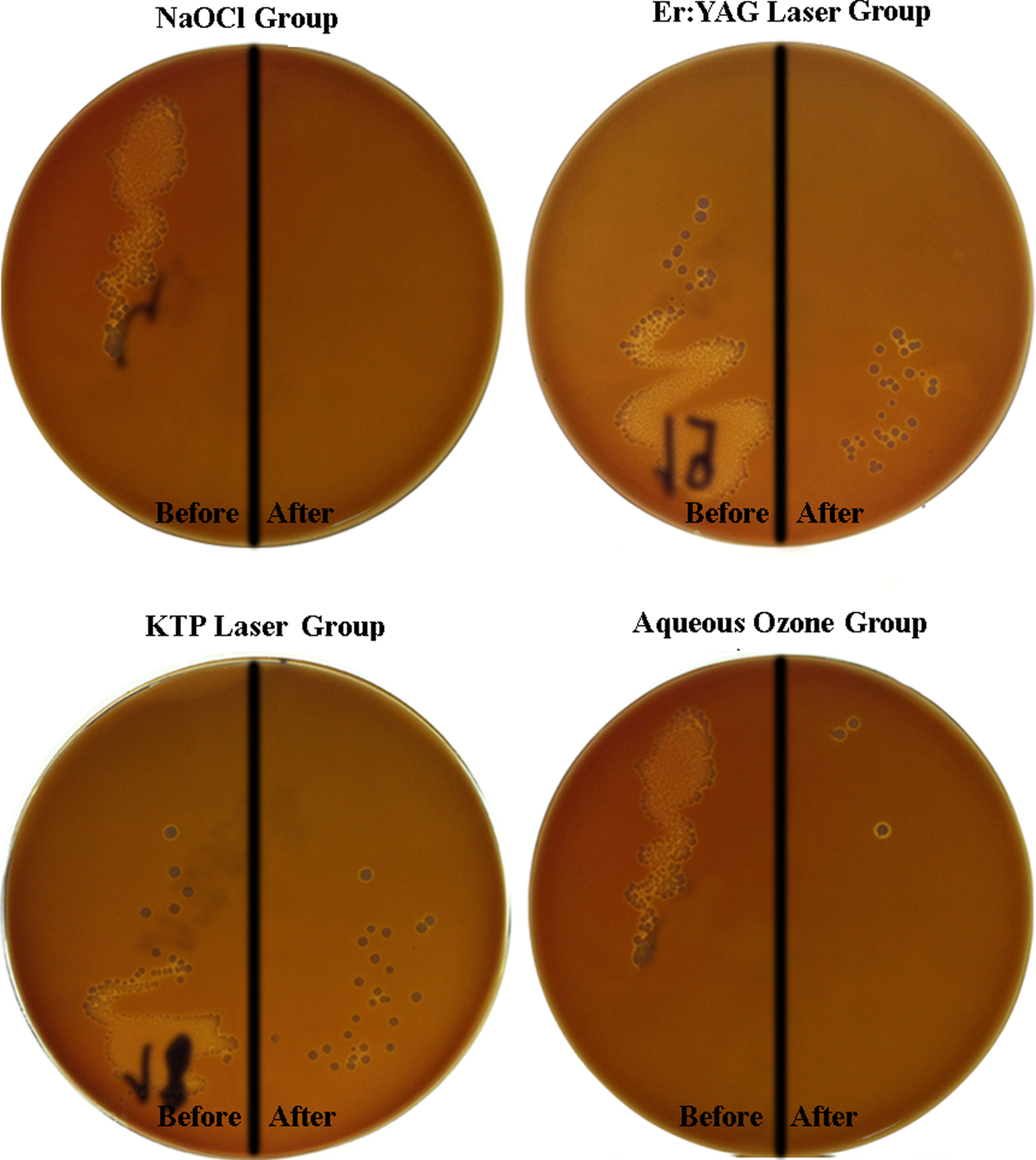
Cross-sectional images of Enterococcus faecalis on blood agar plates of samples obtained from root canals before and after irrigation.
By the one-way ANOVA, F=128.401, p=0.000, p<0.05, n=20 specimens per experimental condition.
Values with different superscript letters are statistically significant (p<0.05, Tukey's test).
CFU, colony-forming units.
NaOCl.
Er:YAG laser.
KTP laser.
Aqueous ozone.
The results indicated that there is statistically significant differences among the NaOCl and other all groups (p<0.05). Although there were statistically significant differences among aqueous ozone and laser groups (Er:YAG and KTP) (p<0.05), there was no statistically significant difference between Er:YAG and KTP laser (p>0.05).
Although the aqueous ozone group showed the highest antibacterial effect among the experimental groups, the NaOCl group displayed the highest antibacterial effect among all groups.
Discussion
A survey of the literature shows that no study compares the antibacterial effect of laser systems with aqueous ozone in human root canals. This study was performed to evaluate the antibacterial effect of these two alternative methods of root canal disinfection that have specifically drawn attention recently. A 3 min application period was preferred for all groups to resemble an actual clinical application period.
E. faecalis is a facultatively anaerobic, gram-positive coccus. It has been implicated in persistent root canal infections 11 and has been used in several previous studies to evaluate the efficacy of endodontic irrigants, especially because of its high level of resistance to a wide range of antimicrobial agents. 13 This microorganism plays a major role in post-treatment disease, and it will be advantageous if alternative ways can be sought to successfully eradicate it from the root canal system.
Irrigation is one of the most important steps in endodontic treatments, and a variety of irrigants have been used in endodontics to eliminate or reduce the number of bacteria invading the root canals. 14 NaOCl is currently the most commonly used irrigant in endodontics and is recommended as an effective solution in the treatment of infected root canals because of its well-known bactericidal and antimicrobial actions. 15,16 However, it has been shown that microorganisms such as E. faecalis are resistant to NaOCl, especially at low concentrations. 17 The results of some studies showed that 5.25% was the most efficient concentration of NaOCl assessed, and that it killed the bacterial cells in<2 min. 18,19 Consistent with the results of these studies, 19,20 a 5.25% NaOCl solution destroyed all of the E. faecalis inoculated in the root canals.
In recent years, using ozone for endodontic treatments has gained popularity as an alternative approach to root canal disinfection. In particular, the antimicrobial efficacy of aqueous ozone has been investigated in a few studies. 7,8,20,21 For example, Nagayoshi et al. 7 examined ex vivo the effect of aqueous ozone against E. faecalis and Streptococcus mutans in bovines. Root canals were irrigated for 10 min with 4 mg/L aqueous ozone. A significant decrease in the amount of remaining bacteria was observed when the root canals were disinfected with aqueous ozone. Hems et al. 8 also studied the antibacterial effect of gaseous and aqueous ozone against E. faecalis in root canals, and a reduction in bacteria was detected after an application of aqueous ozone for 4 min. In another study, Cardoso et al. 20 evaluated the effectiveness of aqueous ozone in the elimination of E. faecalis and Candida albicans from root canals. They found a significant reduction in the number of microorganisms. Finally, Estrela et al. 21 investigated the antimicrobial efficacy of aqueous ozone and NaOCl in human root canals inoculated with E. faecalis. Their results showed that aqueous ozone was not sufficient for the complete inactivation of E. faecalis after 20 min.
In the present study, the antibacterial effect of aqueous ozone against E. faecalis was investigated in human root canals. The most crucial differences from the other aforementioned studies 7,8,20,21 are the increase in the ozone concentrations (16 ppm) in the aqueous ozone and the decrease in the application time (3 min). Consequently, although the data obtained from this study showed a significant reduction of E. faecalis in the root canals, the bacteria could not be completely eradicated. These results are the same as results of the aforementioned studies. 7,8,20,21 As a result, the use of aqueous ozone as the only irrigation solution has not been proven to be an equivalent alternative irrigation solution to NaOCl. Laser systems have played a significant role in root canal sterilization in recent years. The Nd:YAG, 11 –13 KTP, 22 and Er:YAG 9,11,12 lasers systems were investigated for use in root canals, and showed remarkable results in bacterial reduction. In particular, the Er:YAG laser has been used with water cooling on hard dental tissues. 9,11,12 It is possible that different results could be obtained without water application; however, that approach may jeopardize the integrity of the surrounding tissues because of the detrimental effects of heat 23 and the porous structure of the dentin surface 24 generated by the laser. Bergmans et al. 25 aimed to define the bactericidal effect of an Nd:YAG laser with 1.5 W against E. faecalis in root canals for 20 sec. As a result, the Nd:YAG laser caused a significant reduction in the remaining bacteria, but it still did not provide complete sterilization. Moreover, Yasuda et al. 11 evaluated the bactericidal efficacy of the Nd:YAG and Er:YAG lasers in experimentally infected bovine and human root canals. They used 1.0 W for 30 sec. As a result, the Er:YAG laser showed higher bactericidal effects than the Nd:YAG laser. In another study, Meire et al. 12 compared the in vitro antimicrobial action of Er:YAG and Nd:YAG lasers' irradiations on different microorganisms associated with endodontic infections (e.g., E. faecalis) for 60 sec. According to their study, the Er:YAG laser irradiation was superior to irradiation with the Nd:YAG laser for inactivating microorganisms. Dos Santos Antonio et al. 26 explained the bacterial (E. faecalis) reduction after intracanal irradiation with the Er:YAG laser using 1 W of irradiation. The remaining bacteria were counted immediately, and 48 h after laser irradiation. There was an immediate 99.95% reduction in bacteria and the reduction was 84.52% after 48 h. In contrast, Kuştarci et al. 22 evaluated the antimicrobial activity of a KTP laser and gaseous ozone in experimentally infected root canals. The KTP laser achieved a significant reduction but did not completely sterilize the root canals. In the previously mentioned studies, 11,25,26 the complete elimination of bacteria could not be achieved with the parameters used in their studies. Referring to the aforementioned results, the irradiation power (2.0 W, 100 mJ, 20 Hz) was raised and standardized for both the Er:YAG and KTP lasers. In the present study, although the Er:YAG laser caused a higher reduction of bacteria than the KTP laser, there was no statistically significant difference between these two systems. Neither the Er:YAG laser nor the KTP laser could destroy all of the bacteria in the root canals. In the aforementioned studies, 11,12 the Er:YAG laser showed higher bactericidal effects than the Nd:YAG laser. These results were in accordance with our results.
Aqueous ozone had a stronger antibacterial effect than the Er:YAG and KTP lasers in root canals. As a result, aqueous ozone was better than both of these laser systems for disinfection. Within the limitations of the present study, it can be concluded that although aqueous ozone holds promise as an alternative disinfecting agent, its antibacterial efficacy is not as great as the traditional sodium hypochlorite irrigation methodology. Root canal disinfectants are expected to possess multiple properties such as good antibacterial ability, biocompatibility, and low toxicity. Each specific system has its own advantages and disadvantages in that respect. Even though the results of the present study showed no superiority of aqueous ozone compared with sodium hypochlorite, different results are also likely to be obtained with different combinations of irrigation and disinfection strategies. Therefore different methodologies can be tested to enhance the antibacterial action of aqueous ozone.
Conclusions
Within the limitations of this in vitro study, it can be concluded that aqueous ozone had a stronger antibacterial effect than the Er:YAG and KTP lasers in infected root canals. Moreover, although aqueous ozone showed a remarkable antibacterial effect, it did not show efficacy equal to traditional NaOCl against E. faecalis. Furthermore, the KTP and Er:YAG lasers did not differ in their antibacterial activity.
Footnotes
Acknowledgment
The study was financed by the Scientific Research Unit of Cumhuriyet University (CUBAP) in Sivas, Turkey.
Author Disclosure Statement
No competing financial interests exist.