
Abstract
Introduction
Evidence for the benefits of good glycemic control, as monitored by glycated hemoglobin measurements, has been developed in the 35 years since they were introduced to the point at which HbA1c assays play central roles in patient management, clinical guidance and audit, and clinical trial design. 8 HbA1c has been shown to be an effective screening tool for the detection of type 2 diabetes mellitus. 9 Recently, an association of glycated hemoglobin with the complexity of the coronary artery disease has also been shown even in non-diabetic adults. 10 HbA1c is a measure of erythrocyte hemoglobin glycation, and as erythrocytes have an ∼120 day life span, HbA1c reflects mean glycemia for the previous 3 months (weighted to the most recent month). There are several conditions that confound the HbA1c measurement, such as hemolytic anemia (lowers HbA1c) or aplastic anemia (raises it), but in most circumstances, HbA1c is a valid index of glycemia. 11 Even though many other parameters such as plasma fructosamine, 12 plasma glycated albumin, 13 –15 serum 1,5-anhydro-D-glucitol, 16,17 and urinary myoinositol 18 have been tried to asses glycemic control, glycated hemoglobin has been widely accepted for this purpose. The recommendation is to measure HbA1c every 3–6 months, and treat to a target level of<6.5–7%. If these recommendations were successfully followed in most people with diabetes, long-term complications, especially microvascular complications, would be markedly reduced. 7,11
Different methods have been developed for the estimation of glycated hemoglobin, which include cation exchange high performance liquid chromatography (HPLC) method, 19,20 latex agglutination immune assay, 21 isoelectric focusing of globin chains, 22 electrophoresis, immune turbidimetric assays, 23 and boronate affinity chromatography. 24,25 An International Federation of Clinical Chemistry (IFCC) reference method based on electron-spray ionization-mass spectrometry or capillary electrophoresis for the calibration of HbA(1c) and HbA(0) was also employed in Europe. 26 An electrochemical biosensor for fructosylvaline for glycosylated hemoglobin detection based on core-shell magnetic bionanoparticles modified gold electrode was developed by Chawla and Pundir. 27 Recently, they further improvised by developing a biosensor based on immobilization of fructosyl amino acid oxidase onto ZnO nanoparticles-polypyrrole film for the amperometric estimation of HbA1c. 28
However, these methods suffer from one or more disadvantages. Many of the chromatographic methods involve the use of two buffers, the first to elute unbound material from the resin in such a way that does not cause the desorption of the specifically bound material. A second buffer, used at a different pH or ionic strength, or containing a competitive inhibitor, is needed to elute the specifically bound material. The temperature, pH, ionic strength, or presence of a competitive inhibitor is needed to elute the specifically bound material. Moreover, the methods are nonautomated or only semiautomated, and require several different steps and several vessels.
Berger et al. 29 have explored the feasibility of measuring blood glucose concentration by near-infrared Raman spectroscopy. Recently, Barman et al. 30 have reported a Raman spectroscopy-based sensitive and specific detection method for the estimation of glycated hemoglobin. Because of its high chemical specificity, Raman spectroscopy has been considered to be a promising technique for noninvasive disease diagnosis. However, during Raman excitation,<1/1,000,000 photons undergo spontaneous Raman scattering, and such weakness in Raman scattered light often requires highly efficient collection of Raman scattered light for the analysis of biological alterations. Berger 31 has explored the usage of laser technology for glucose monitoring. However, laser technology involves very expensive instrumentation, which cannot be afforded by all small hospitals.
Hence, there is a need for a glycated hemoglobin assay that is easy to perform, free from interferences, cost effective, and relatively insensitive to experimental variables (such as pH and temperature), and that measures glycated hemoglobin accurately and with precision.
Ultraviolet/visible (UV/VIS) absorption spectroscopy has been used in the clinical laboratory for many years. 32 The technique has appeal, as it is almost universal in its application. 32 Absorption spectroscopy is usually performed with molecules dissolved in a transparent solvent, such as aqueous buffers. The absorbance of a solute depends linearly on its concentration and, therefore, absorption spectroscopy is ideally suited for quantitative measurements. 32 The wavelength of absorption and the strength of absorbance of a molecule depend not only on the chemical nature but also on the molecular environment of its chromophores. Absorption spectroscopy is therefore an excellent technique for following ligand-binding reactions, enzyme catalysis, and conformational transitions in proteins and nucleic acids. 32,33 Spectroscopic measurements are very sensitive and nondestructive, and require only small amounts of material for analysis. 32,33 In the present study, we have employed this sensitive direct spectroscopic technique for the estimation of glycated hemoglobin in hemolysate samples of normal individuals and diabetic patients, which does not involve the use of external dyes or reagents. The optic fiber based instrument used in the present technique for recording absorption spectra of glycated hemoglobin (HbA1c) fulfills the abovementioned requirements and may be employed as a supplementary technique to other techniques that already exist.
Material and Methods
Sample collection and handling
The blood samples of individuals with normal glycemic status and confirmed diabetic patients, for the estimation of glycated hemoglobin, were collected from the Clinical Biochemistry Laboratory, Kasturba Hospital, Manipal. India. The hemolysates were prepared by employing the method described in the textbook of clinical biochemistry by Teitz. 34
The samples were allowed to stand at room temperature in upright position for ∼30 min. The clear plasma thus obtained was discarded. Then, for 1 mL of cells, 3 mL of 0.9% NaCl was added to wash the cells. Next, the sample was centrifuged at 3000 rpm for 5 min and the supernatant was discarded. The procedure of adding 0.9% NaCl and centrifuging and discarding the supernatant was repeated several times. To 1 mL of packed cells left behind, 1.5 mL of deionized water was added, with constant mixing in vortex for 5 min, and centrifuged 3000 rpm for 5 min. The supernatant hemolysate was used for analysis. In the present study, we used 30 samples (age range, 30–60 years; mean age, 45 years) with HbA1c (%) in the range 4–15.5%. An ion exchange HPLC set up (VARIANT™ II TURBO link fully automated Hemoglobin A1c testing program, Bio-Rad Laboratories, Inc., Hercules, CA) was used to obtain reference values. The lyophilized human red blood cell (RBC) hemolysate calibrator used was from Bio-Rad.
Experimental setup
Ocean Optics CHEMUSB4-UV-VIS single beam spectrophotometer used for recording absorbance of glycated Hb (HbA1c %) samples is shown in Fig. 1. The CHEMUSB4-UV-VIS consists of a USB4000 spectrometer with a combination deuterium tungsten halogen light source and 1 cm cuvette holder and high-speed electronics. The spectrophotometer covers a 190–880 nm range, has an optical resolution of 1.0 nm (full width at half maximum [FWHM]) and captures 3648 wavelengths in<1 sec. It sees changes as small as 0.01 absorbance units. The light source (Fig. 1, far right) sends light via an input fiber into a cuvette in a cuvette holder (Fig. 1, bottom center). The light interacts with the sample. The output fiber carries light from the sample to the spectrometer (Fig. 1, top center) connected to the computer (Fig. 1, far left). The excitation end of the fiber was held perpendicularly to the surface of the cuvette at a distance of 1–2 mm, which was optimal to attain the best absorption intensity, and the distance between the fiber tip and the cuvette surface was the same for all spectral recordings. All absorption spectra were recorded with consistent experimental procedures (in terms of software parameters and amount of HbA1c sample taken in the cuvette).
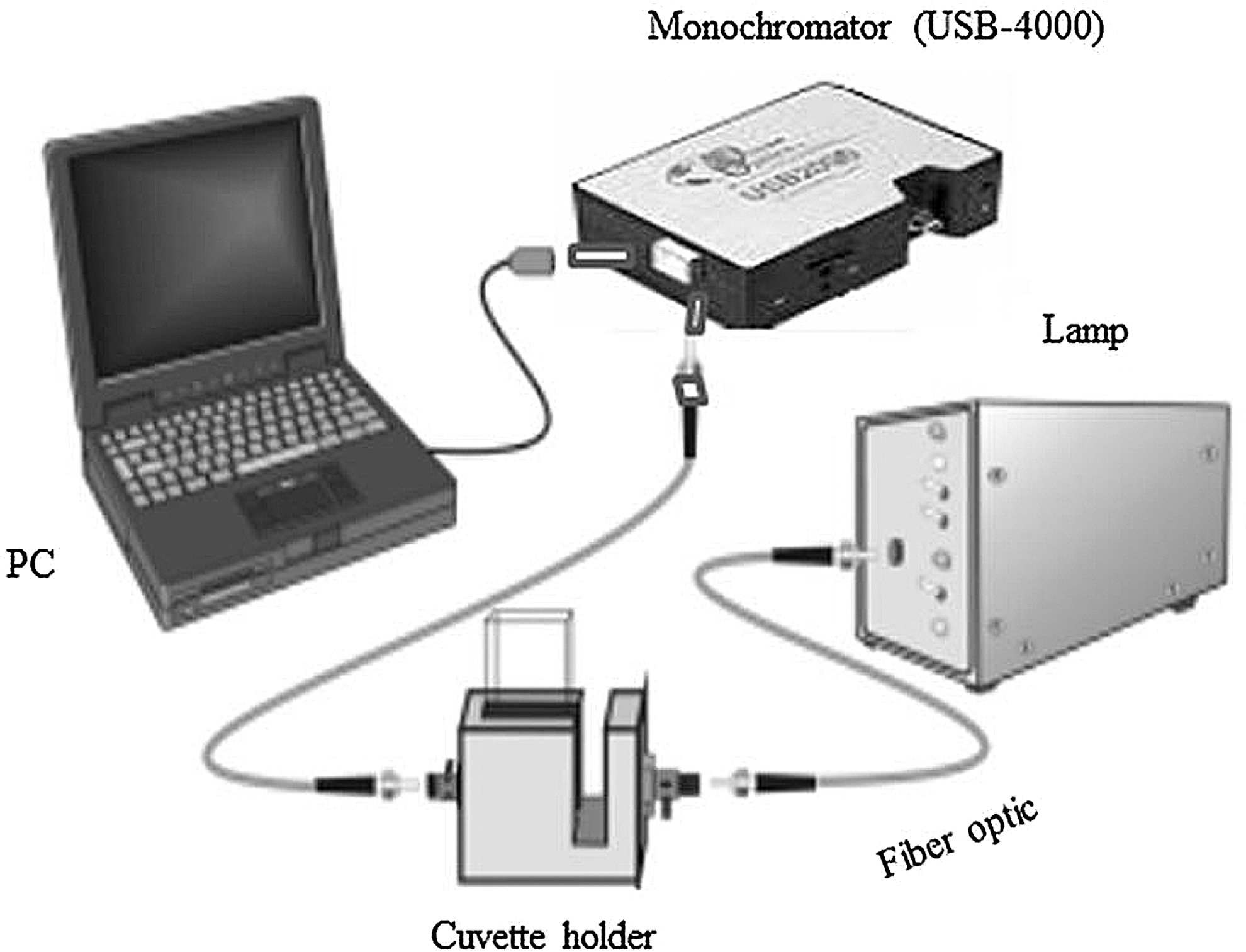
Ocean Optics CHEMUSB4-UV-VIS single beam spectrophotometer used for recording absorbance spectra of glycated Hb (HbA1c %).
Results
The sensitivity and detection limit of the experimental setup was checked by recording absorption spectra of lyophilized human RBC hemolyzed calibrator.
Figure 2 shows the overlaid absorbance spectra of lyophilized human RBC hemolyzed calibrator recorded in the UV-Vis region (190–880 nm). The curves marked 1, 2, 3, and 4, respectively, correspond to 10.2%, 7.5%, 5.4%, and 2.7% of glycated Hb. Each spectrum was baseline corrected to remove the background interference. The inset of Fig. 2 shows a baseline corrected absorbance spectrum of lyophilized human RBC hemolyzed calibrator (5.4%). Five peaks marked P1 (288 nm), P2 (344 nm), P3 (415 nm), P4 (546 nm), and P5 (578 nm) corresponding to glycated hemoglobin were identified. The intensity of these five peaks varied in proportion to the variation of the concentration of lyophilized human RBC. Area under the curve in the spectral range (250–800 nm) of each baseline corrected absorption spectrum was correlated/compared with its corresponding HBA1c (%) value obtained through ion exchange HPLC. A plot of concentration versus “area under the curve” of absorbance spectra of lyophilized human RBC hemolyzed calibrator is shown in Fig. 3. A linear trend line added to these points showed very good fitting with R2 value of 0.9603, which signifies that the parameter “area under curve” is a suitable parameter for the estimation of HbA1c (%).
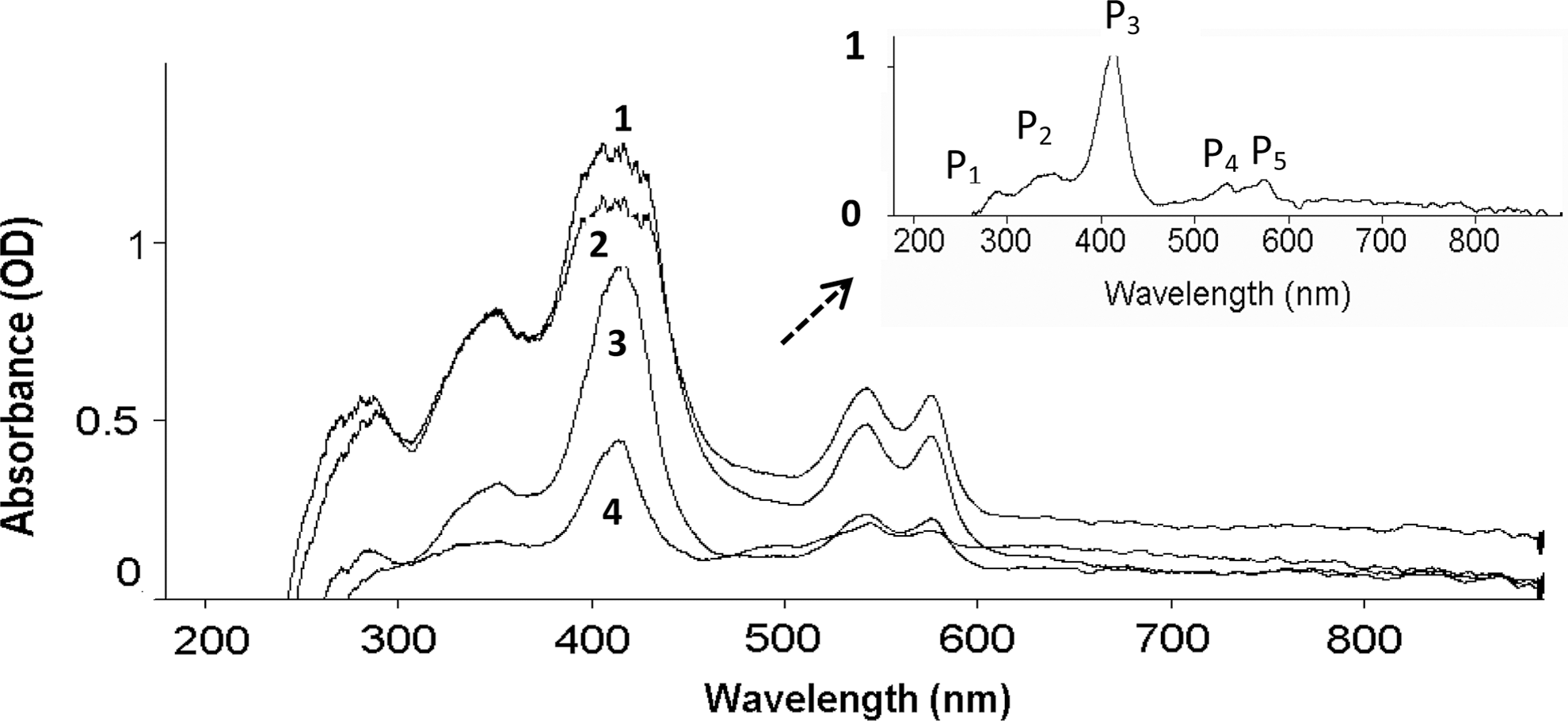
Typical overlaid absorbance spectra of lyophilized human red blood cell (RBC) hemolyzed calibrator recorded in the UV-Vis region (190–880 nm). The curves marked 1, 2, 3, and 4, respectively, correspond to 10.2%, 7.5%, 5.4%, and 2.7% of glycated Hb. A baseline corrected absorbance spectrum of lyophilized human RBC hemolysed calibrator (5.4%) is pictured in the inset.
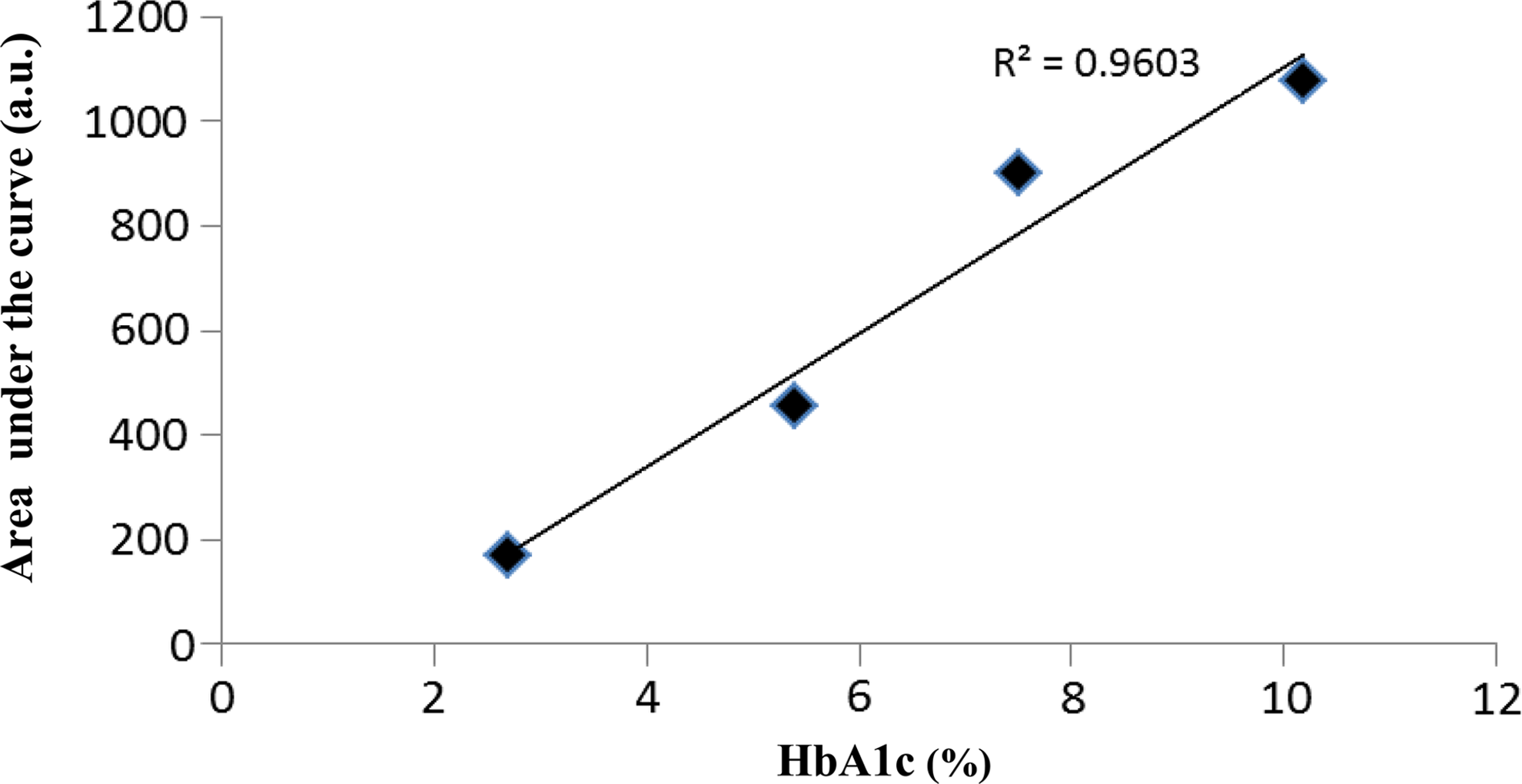
Concentration versus “area under the curve” of absorbance spectra of lyophilized human red blood cell (RBC) hemolyzed calibrator.
Discussion
In the conventional ion exchange, HPLC technique used for the estimation of HbA1c, the hemoglobins are separated based on their ionic interactions with the cartridge material, and the separated hemoglobins then pass through the flow cell of the filter photometer, where changes in the absorbance of a single peak at 415 nm (P3) is measured and the area under the curve of this single peak is used for the estimation of HbA1c (%). However, in the present absorbance technique, as a deuterium-tungsten (DT) lamp provides broad band excitation, the changes in the absorbance of other derivatives of glycated Hb (P1, P2, P4, P5) are also considered for the estimation of HbA1c, which we believe is more accurate than using the single peak area for the estimation of glycated Hb. Also, in ion exchange HPLC technique, normal total hemoglobin concentration corresponds to a total area of ∼2.5 million μV/sec. For some high total area, high HbA1c samples (e.g., 15% or 140 mmol/mol HbA1c with 5 M total area), the HbA1c peak may elute outside of the established retention time window. In such cases, samples are to be diluted further, ∼2.5 M total area, and rerun. However, in the present absorption spectroscopy technique, HbA1c samples>50% also can be determined in a single run. There is no upper limit for the total area as such. In addition to this, samples with HbA1c as low as 1% can be estimated by this technique.
In the present study, we standardized the absorption spectroscopy technique for the estimation of HbA1c using a patient's sample with HbA1c value of 10.4%. The sample was diluted to minimize the Rayleigh scattering effect. The sample was diluted in a stepwise manner using saline as the diluent until the absorbance spectral pattern of the sample matched with the absorbance spectrum of lyophilized human RBC hemolyzed calibrator with HbA1c value 10.2%. To achieve this, the sample was diluted 1:4 (i.e., for 0.5 mL blood+2 mL saline). The same dilution technique was employed for all the samples for the analyses. A typical overlaid absorbance spectra of (a) lyophilized human RBC hemolyzed calibrator HbA1c (10.2%) and (b) a diabetic patient's hemolysate sample with HbA1c value of 10.4% is shown in Fig. 4. The areas under the curves of these two spectra were also equal without any significant difference.
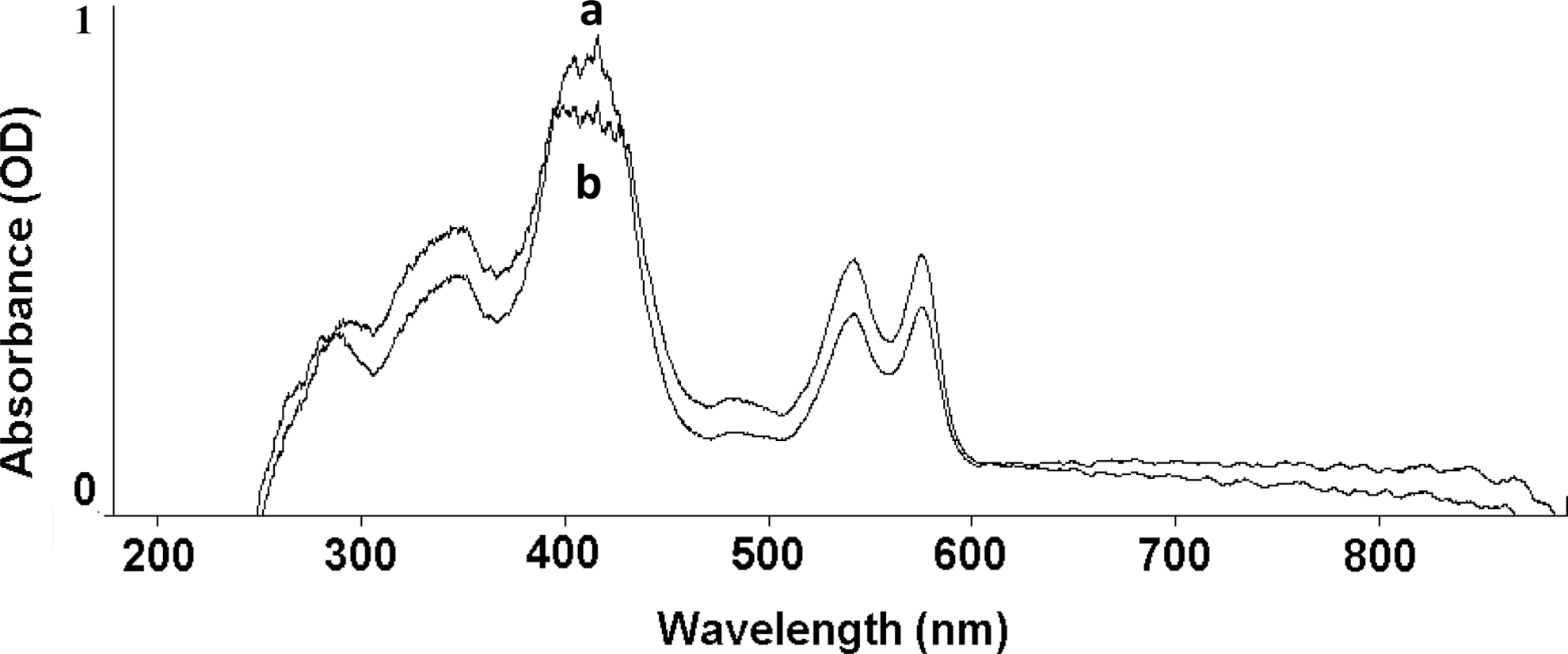
Typical overlaid absorbance spectra of
The overlaid absorbance spectra of normal and diabetic hemolysate samples with HbA1c values in the range 5.2% (lower-most curve) to 15.2% (top-most curve) are shown in Fig. 5. From Fig. 5, it is clearly evident that the “area under the curve” of each absorbance spectrum reflects the quantity of HbA1c (%) present in the sample. A comparison of HbA1c measurement by HPLC and the absorbance spectroscopy method is shown in Fig. 6.
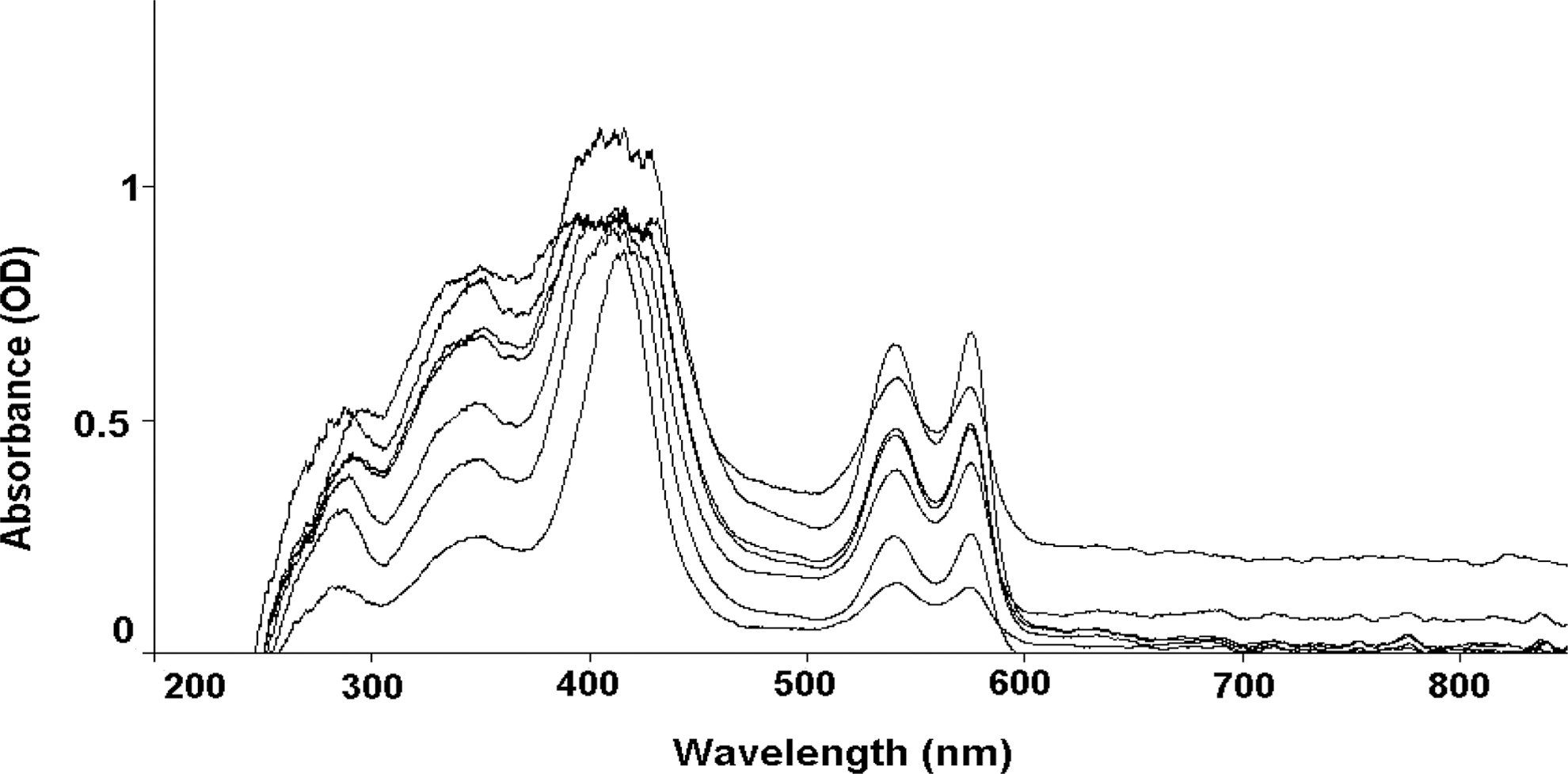
Overlaid absorbance spectra of normal and diabetic hemolysate samples with HbA1c values in the range 5.2% (lower-most curve) to 15.2% (top-most curve).
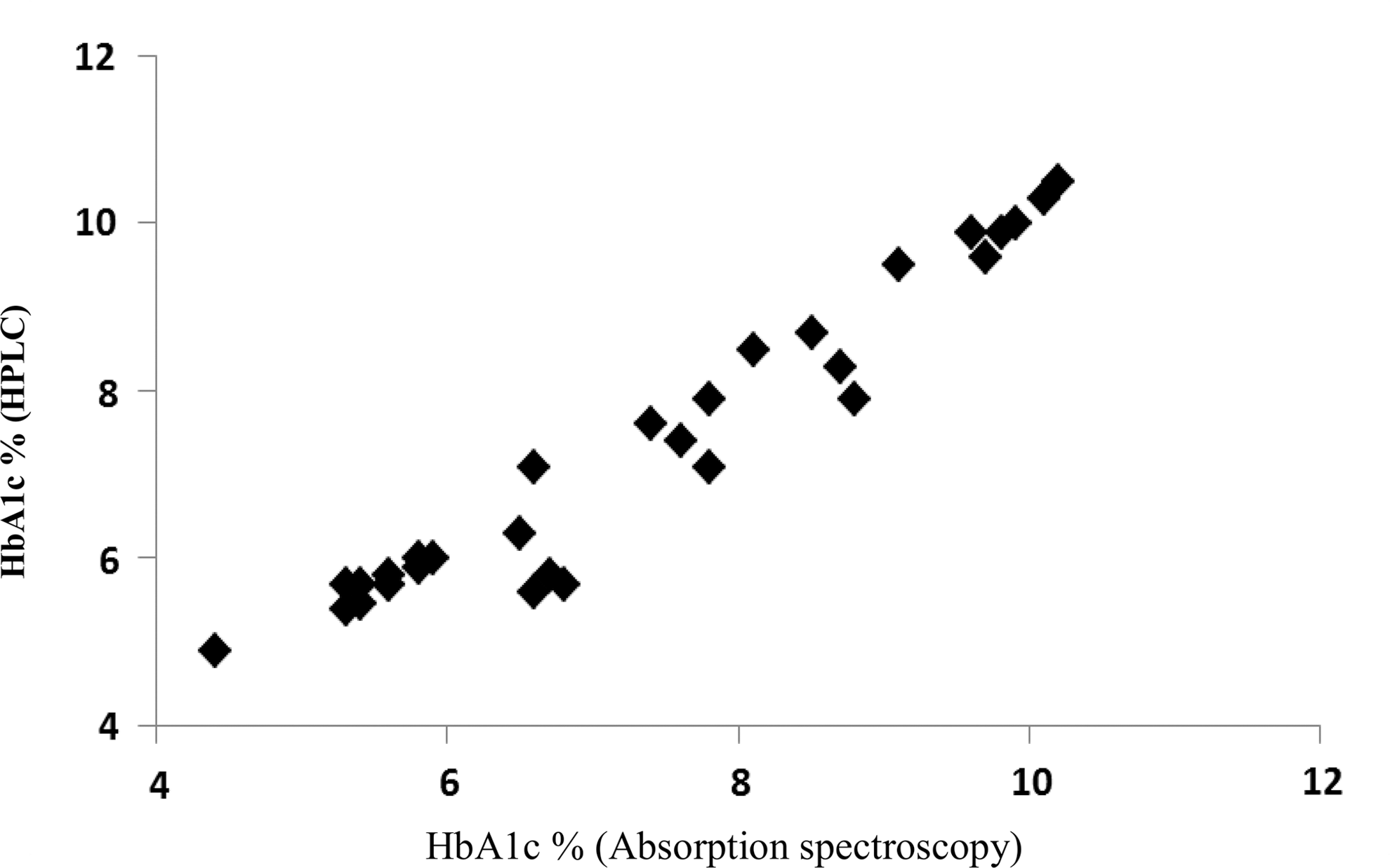
Comparison of HbA1C (%) measurement by the high performance liquid chromatography (HPLC) and the absorbance spectroscopy method.
From Fig. 6, it is obvious that HbA1c (%) values calculated by “area under the curve” in the present absorption spectroscopy technique are close to the values estimated by the standard HPLC technique with a correlation coefficient of 0.967. The mean glycated Hb (±SD) values by HPLC and absorption spectroscopic technique were found to be 7.36±1.746 and 7.34±1.783, respectively. The statistical analysis was performed by SPSS software. This significant correlation clearly shows that the present absorption spectroscopic technique is quite good in the estimation of HbA1C in the hemolysate samples. Hence, it can be used as a supplementary technique to the other conventional techniques used for the estimation of glycated hemoglobin.
Conclusions
This pilot study (with a limited number of samples) was conducted to check whether it is possible to employ a simple direct absorption spectroscopic technique for the estimation of glycated hemoglobin levels in the hemolysate samples. A good correlation (R2 =0.967) between HbA1c values measured by absorption spectroscopic method and standard HPLC method supports the validity of absorption spectroscopy for the estimation of glycated Hb (HbA1c). As light delivery and collection are compatible with optical fibers, absorption spectroscopic information can serve as a powerful tool for assessing the state of a diabetic patient, and for the estimation of HbA1c. It appears that absorption spectroscopy, therefore, may be utilized as a supplementary technique to the existing methods used for the same purpose. As the technique is quick, and has a high rate of success, it is attractive for real-time applications. As the absorption technique involves inexpensive instrumentation and needs a small quantity of the sample, it is more suitable in primary healthcare centers and low budget private clinics for the diagnosis and management of diabetes. However, to optimize the use of a spectroscopy method in disease detection and treatment, it is important that the information provided by the optical signals are properly understood and implemented. Hence, the technique can be further optimized when a sufficient number of samples is available for the study and, therefore, the sensitivity and specificity of this technique can be improved further.
Footnotes
Acknowledgments
The authors thank Manipal University, Manipal, India for supporting this study.
Author Disclosure Statement
No competing financial interests exist.