
Abstract
Introduction
Antibiotic resistance has become a global problem, with some strains of bacteria that are nearly untreatable. 6 –8 Emerging patterns of resistance have stimulated interest in the search for new strategies.
Riboflavin (vitamin B2) and its byproducts are redox-active chromophores found in enzymes and photoreceptors. 9 These compounds are photoreactive and photodecompose with exposure to UV and visible light. They have the potential for use as high efficacy antimicrobial agents with low toxicity and low probability of inducing protein damage. The chemical mechanism for the rapid photodecomposition of riboflavin and how to protect it has been extensively studied. 10 –12 Riboflavin is capable of interacting with and damaging nucleic acids of pathogens after UVA exposure. Damage may occur by direct electron transfer, production of electrophilic singlet oxygen, or generation of hydrogen peroxide with formation of hydroxyl radicals. 12 Both pathogen DNA and RNA are affected in the absence of oxygen. This strategy has been proven in pre-clinical investigations to be effective against bacteria, intracellular HIV-1, West Nile virus (WNV), and porcine parvovirus. 11,12
The therapeutic efficacy of using riboflavin solutions and UVA light at 365 nm and 3 mW/cm2 for ulcerative keratitis has also been investigated in multidrug-resistant clinical isolates. 13 The combination of riboflavin and UVA was effective against oxacillin-resistant Staphylococcus epidermidis (ORSE), penicillin-resistant Streptococcus pneumoniae (PRSP), pan-resistant Pseudomonas aeruginosa (PRPA), oxacillin-susceptible S. epidermidis (SE), MRSA, oxacillin-susceptible S. aureus (SA), and susceptible P. aeruginosa (PA).
Strategies that would improve the ability to deliver riboflavin and photoactivate it in a broad range of tissues and clinical scenarios were sought. The absorbance spectra of the flavin chromophores riboflavin and lumiflavin in water demonstrate a peak at 450–455 nm. 14 Other investigators have demonstrated that blue light photoradiation is capable of inhibiting bacterial growth in vitro. 15 –18 Previous work with derivatized collagen solder formulations demonstrated that high concentration preparations could be cast into films for subsequent sectioning into strips for application to the weld site. 19 –23 Collagen is biocompatible and bioabsorbable, and can be used as a carrier for biologically relevant molecules and chromophores.
Preliminary studies were undertaken using this patented collagen technology impregnated with flavin chromophores to optimize the application of a precise dose and controlled release of the antimicrobial agent. 24,25 In vitro studies were undertaken to determine whether visible light activation of collagen-embedded and non-embedded flavin mixture exhibited bactericidal activity. Strains of MRSA, SA, Escherichia coli, and PA were cultured using standard Mueller Hinton and Poloxamer biofilm culture models. Photoirradiation of collagen-embedded and non-embedded flavin mixtures at 455 nm was bactericidal on these strains of bacteria in both standard culture and biofilm models. 24
Pilot studies using an acute infection model were conducted to investigate the potential for wound decontamination. 25 Treated animals received 1×1 cm collagen-flavin composite wafer implants after having incisional wounds infected with MRSA, SA, E. coli, or PA. The wounds were irradiated at 455 nm (300–500 mW output, 1 cm spot diameter) for 15 min using a diode laser 10 min after implant insertion. This pilot study demonstrated that photoradiation at 455 nm after placement of collagen-embedded flavin mixture inhibited bacterial growth in an acutely infected wound model.
The present studies were undertaken to verify the observations from the pilot in vitro and in vivo studies as well as to determine whether multiple treatments and treatment of chronic wounds were feasible and effective using this treatment paradigm.
Materials and Methods
Flavin-collagen composite film preparation
Collagen films were prepared using Conversion Energy Enterprise's patented methods. 26 Purified, telopeptide-poor type I collagen was modified using an acylating reagent such as glutaric anhydride. The degree of derivatization is selected so that the modified collagen remains soluble at physiologic pH. Following chemical modification, the collagen solution was lyophilized. Films were prepared by dissolving collagen solids in flavin solutions. The collagen concentration ranged from 30% to 50%, and flavin concentration varied between 0.5% and 1%. The resultant viscous solution was centrifuged at elevated temperature and poured into molds. After molding, thin films were extracted from the mold, weighed, and cut to shape and size. The composite films (photoactivated collagen-embedded flavins [PCF]) were vacuum packaged in opaque packaging, terminally sterilized by standard electron beam methods, and stored at 4°C until use.
The experimental protocols described subsequently were conducted in accordance with the Public Health Service Policy on Humane Care and Use of Laboratory Animals and were reviewed and approved by the Institutional Animal Care and Use Committee (IACUC) of the Rochester General Hospital.
Infected pressure ulcer model creation
Pressure ulcers were created on the dorsum of 40 BALB/C mice weighing ∼35 g each (Charles River, Wilmington, MA), according to the technique developed in our laboratory. 27 Briefly, animals were lightly anesthetized using a 50:50 mixture of CO2 and O2 for ∼50–60 sec. The dorsal hair was shaved and the area was cleansed with 70% isopropanol after depilation with Nair™. A template was used to mark the location of the magnetic plates to assure a consistent placement on each animal. The skin was gently pulled up and placed between two round ceramic magnetic plates that were 12 mm in diameter and 5.0 mm thick, with an average weight of 2.4 g and 1000 Gauss magnetic force (Magnetic Source, Castle Rock, CO). The resultant “pinch” procedure left a 5.0 mm skin bridge between the two magnets. The underlying carnosis muscle was also captured between the magnets, and sustained ischemia-reperfusion injury. This process created 50 mm Hg pressure between the two plates. A single ischemia-reperfusion cycle (I/R) consisted of a period of magnet placement for 12 h followed by a release or rest period of 12 h. Three I/R cycles were used in each animal to initiate decubitus ulcer formation. Animals were not immobilized, anesthetized, or otherwise treated during the I/R cycles. The animals were allowed food and water ad libitum. The animals resumed normal activity within a few minutes of magnet placement and were able to tolerate the additional weight of the magnets without any difficulty. Ulcers, which are typically fully formed at 3 days, were generally 11 mm in diameter. (Fig. 1). The animals were anesthetized with IP xylazine and pentobarbital prior to inducing infection and/or treatments as described subsequently.

Formed pressure ulcer. The appearance of the formed pressure ulcer after three ischemia/ reperfusion cycles is shown.
The ulcers and surrounding skin were covered with Tegaderm™ (3M Healthcare, St. Paul, MN) and then inoculated with 0.1 mL of a solution containing 1×105 colony-forming units (CFU) per milliliter of MRSA (ATCC, Manassas, VA) in 0.9% saline using a syringe and 25 gauge needle (Figs. 2 and 3). The inoculated fluid was permitted to reabsorb for a minimum of 10 min.
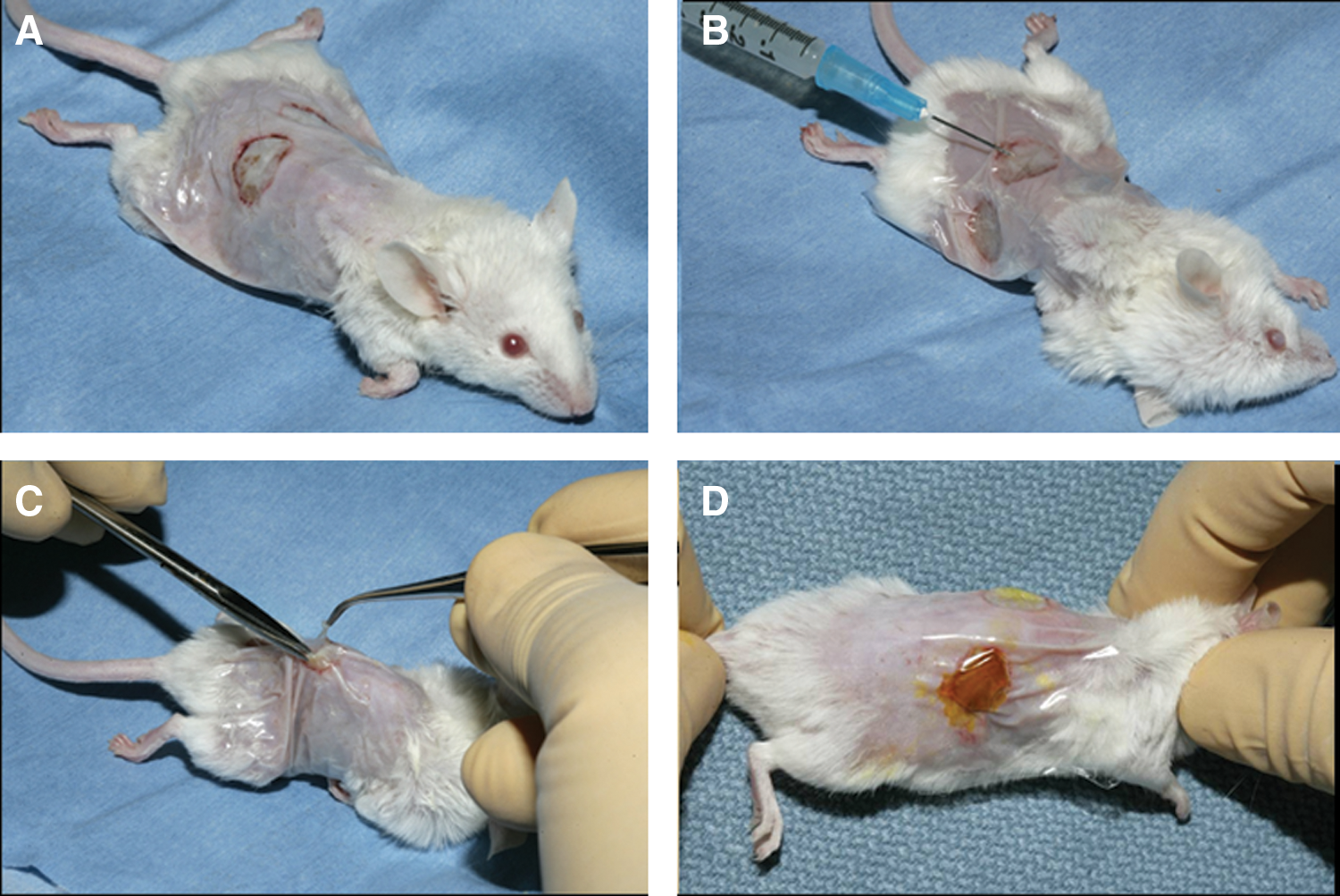
Wound infection and treatment technique.
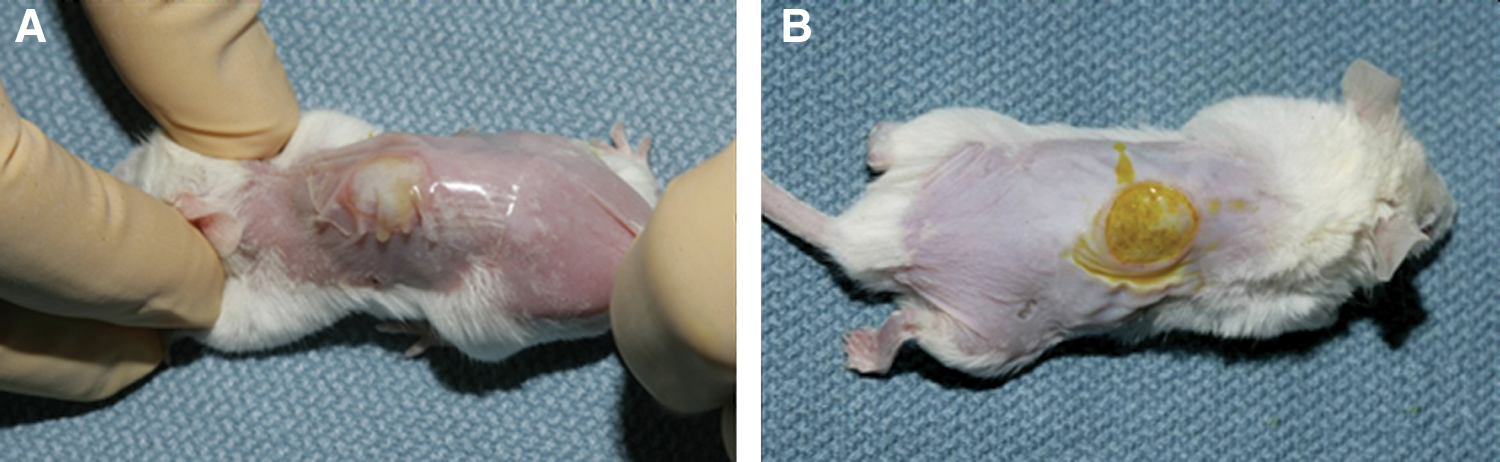
Appearance of wounds after infection.
Single treatment experiment 1
One wound from each animal was treated using the collagen composite films and photoradiated using a blue light source (PCF+R, n=12) or photoradiation alone (R, n=11). Composite dressing-treated wounds received 1×1 cm dressings, which were applied by excising the Tegaderm overlying the ulcer, placing the composite over the wound, and again covering the wound with Tegaderm (Fig. 4). The wounds were irradiated at 455±5 nm (350 mW output, 1 cm spot diameter) for 15 min using a diode laser (Conversion Energy Enterprises, Spring Valley, NY) 10 min after dressing placement. The animals were recovered and individually caged. Control group wounds (C, n=11) were handled similarly, but did not receive the implant or photoradiation. Animals were euthanized at 24 h post-therapy with xylazine and pentobarbital overdose. Cultures were obtained using a sterile cotton tip applicator to sample the wound exudate. Quantitative wound bacterial counts (CFU/g tissue) were determined to measure bactericidal efficiency. One wound from each animal served as a control.

Wound with photoactivated collagen riboflavin (PCRB) dressing placement. The appearance of a pressure ulcer wound is shown after the PCRB has been replaced and the lesion has been again covered with Tegaderm™.
Multiple treatment experiment 2
A daily treatment regimen was investigated based on the basic infected pressure ulcer model used in experiment 1. Wounds were treated using PCF and photoradiated (PCF+R) or were untreated (C). Composite dressing-treated wounds received 1×1 cm PCF films, applied by excising Tegaderm overlying the ulcer, placing PCF over the wound, and covering the wound with Tegaderm. Wounds were irradiated at 455±5 nm (350 mW, 1 cm spot diameter, 15 min) using a diode laser (Conversion Energy Enterprises, Spring Valley, NY) 10 min after dressing placement daily (PCF+R). The PCF+R wounds received 0, 1, 2, or 3 treatments at 24 h intervals (n=8/group). Control wounds received neither PCF nor photoradiation (C). Wounds were cultured daily for 7 days. Cultures were obtained using a sterile cotton tip applicator to sample the wound exudate immediately prior to redressing and treating the wound as per the treatment group parameters described (Fig. 5). Animals were euthanized on day 7 by xylazine and pentobarbital overdose and quantitative bacterial counts (CFU/g tissue) were determined.
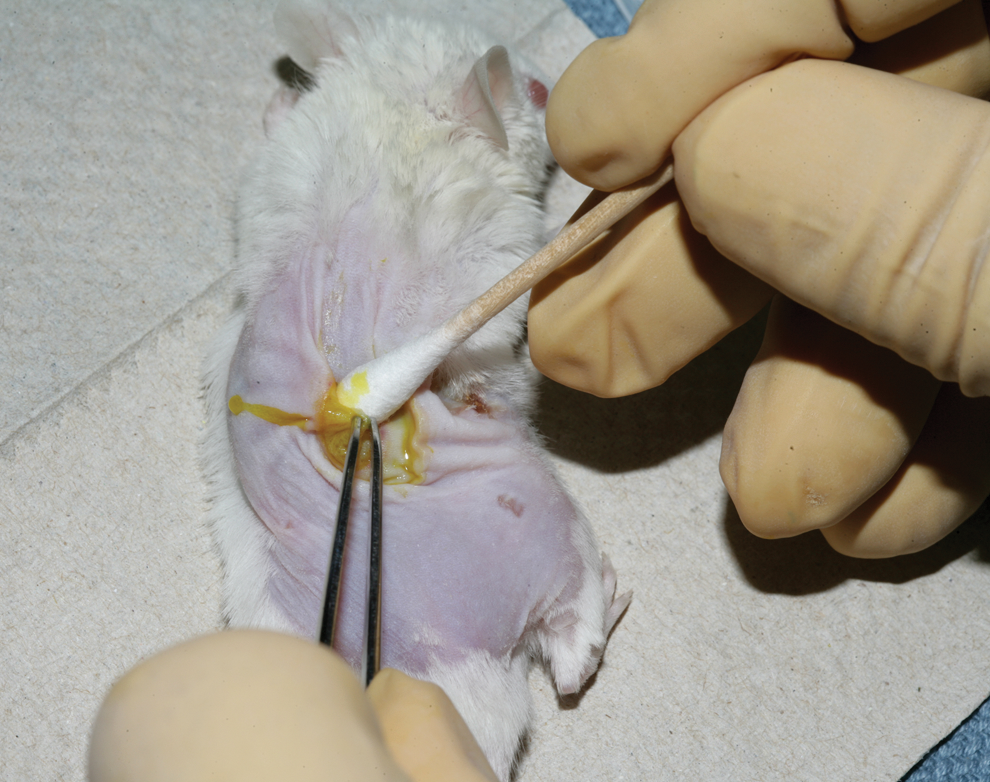
Wound culture method. Quantitative wound cultures are performed by collecting wound exudate with a sterile cotton tip applicator after the overlying Tegaderm™ has been removed.
Quantitative culture technique
Quantitative wound bacterial counts (CFU/g tissue) were determined to measure bactericidal efficiency. The wound area was measured and the exudate was collected by sterile cotton swab (cotton tip applicator [CTA]) after the Tegaderm was carefully removed (Fig. 5). The CTA was submerged in 2.0 mL of physiological saline or trypticase soy broth and repeatedly compressed to release the absorbed wound exudate fluid from the swab. Serial dilutions of the resultant bacterial suspension were constructed from 1:1 to 1:106 for each sample, and 10 μL was inoculated and spread onto Columbia –CNA agar plates containing 5% sheep blood (Fisher Scientific, Pittsburgh, PA) and incubated at 37Co for 24 h. Plates for the serial dilutions were counted if they contained between 30 and 300 colonies. The final number of CFU, expressed as CFU/cm2 of the wound area, was calculated.
Table 1 provides a summary of the experimental design for both the single and multiple treatment studies. Statistical analysis of the results was determined using ANOVA and t test for two samples with unequal variance.
PCF, photoactivated flavin collagen composite film; MRSA, methicillin-resistant Staphylococcus aureus; CFU, colony-forming units.
Results
The results for the single treatment regime after wound infection with MRSA are demonstrated in Fig. 6. The composite dressing plus photoradiation (PCF+R) resulted in a statistically significant reduction in bacterial counts at 24 h post-treatment as compared with untreated controls (C) (p<0.0001). However photoradiation alone (R) was no different from untreated controls (p=0.24). These results confirm those obtained in the pilot study using the incisional wound model. 25 A single PCF+R treatment resulted in a 2 log reduction in bacterial counts at 24 h post-therapy.
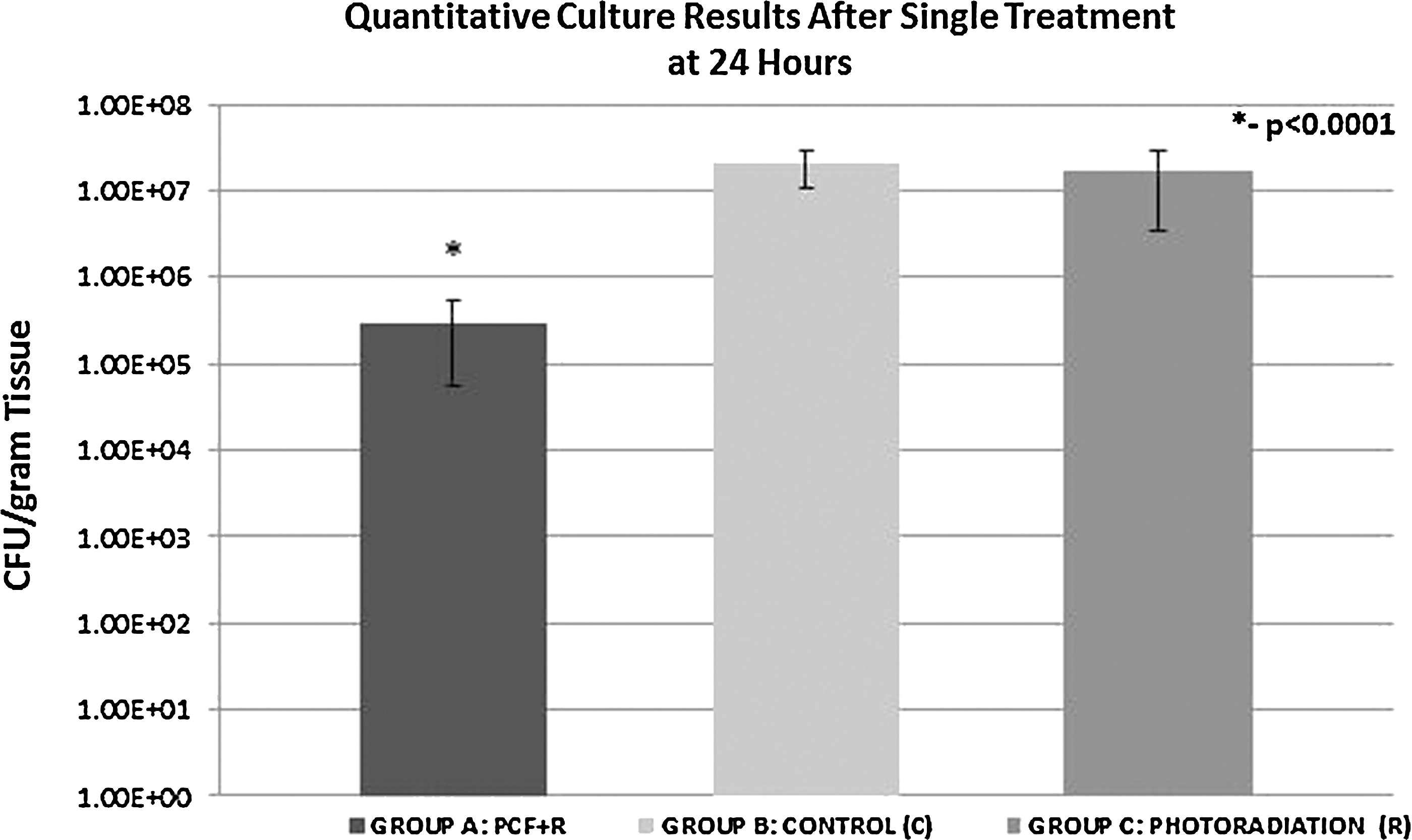
Quantitative culture results at 24 h after single treatment, Use of photoactivated collagen-embedded flavins (PCF) plus photoradiation (PCF+R) resulted in a statistically significant reduction in bacterial counts at 24 h as compared with untreated controls (*p<0.0001). Counts for wounds treated with photoradiation alone (R) were no different from those of untreated controls (C) at 24 h (p=0.24).
The results for the multiple (daily) treatment study are shown in Figs. 7, 8, and 9. PCF+R resulted in statistically significant 2–3 log reduction in bacterial counts as compared with untreated controls (C) (p<0.001). As expected, the antibacterial effects increased with the number of treatments administered. This effect was most pronounced in the group receiving three daily treatments. The results at 72 h are shown in Figs. 7 and 8. The antimicrobial effects of PCF+R therapy persisted for several days post-therapy (p<0.05) as demonstrated by quantitative wound culture performed at 168 h (day 7) as is shown in Fig. 8. Figure 9 plots the rate of reduction of bacteria at day 7 versus the number of treatments given.

Quantitative wound culture results days 1–3 after multiple treatments. Quantitative wound culture results are shown for the first 72 h after wound infection and treatment. Treatment with photoactivated collagen riboflavin (PCRB) plus photoradiation resulted in statistically significant 2–3 log reduction in bacterial counts (p<0.001). Antibacterial effects increased with the number of treatments (p<0.002).

Quantitative culture results at 7 days after multiple treatments. Quantitative wound culture results at 168 h demonstrate that treatment with photoactivated collagen riboflavin (PCRB) plus photoradiation results in persistent reductions in bacterial counts (p<0.05) for several days after the last treatment. The effect increases with the number of treatments provided.
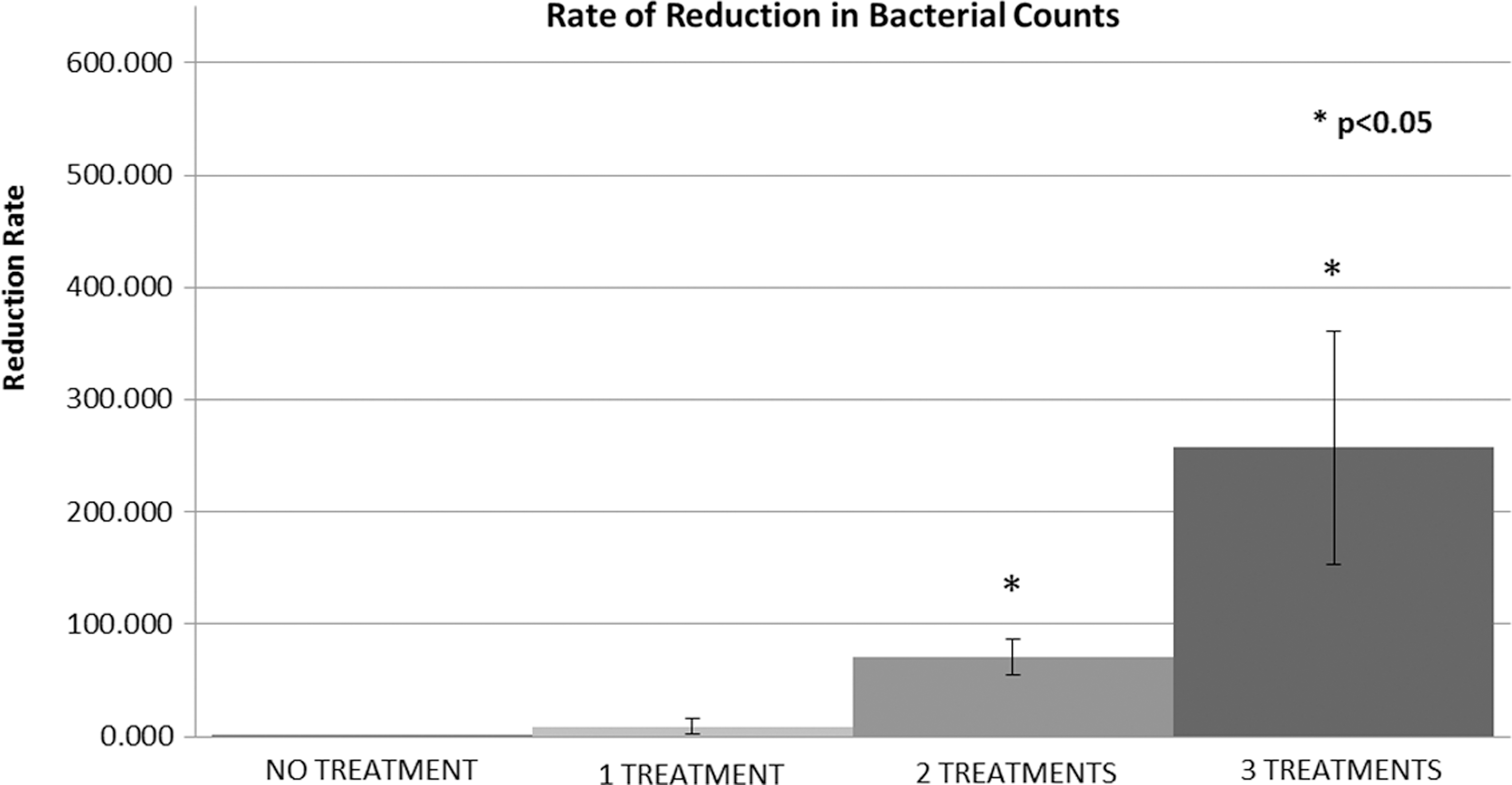
Rate of reduction in quantitative bacterial counts following multiple treatments. The rate of reduction in wound bacterial counts is shown. The rate of reduction is statistically different between treatment groups (p<0.05).
Discussion
The increasing incidence of antibiotic resistance threatens our ability to successfully manage acute and chronic wounds. Nosocomial infections are a global problem that will require innovative and cost-effective solutions. The spectrum of pathogens that are responsible for nosocomial infections continues to change over time. 28,29 Antibiotic-resistant strains of both gram-positive and gram-negative microorganisms are being increasingly isolated from infections in hospitalized and postoperative patients as well as from the environment. 30
Emerging evidence indicates that microbial populations colonize wounds and tissues in biofilms. These thin layers of microorganisms adhere to the surface of an organic or inorganic structure, together with their secreted polymers. They are the predominant phenotype of nearly all bacteria in their natural habitat, whether pathogenic or environmental. Current estimates suggest that >65–80% of infections are caused by bacteria growing in biofilms. 31 –33 Biofilms have demonstrated the ability to persist in concentrations of antibiotics and biocides that typically inhibit and completely destroy planktonic cells. 31 The same strain of bacteria can be two- or threefold more resistant to antibiotics if part of the biofilm community. 32,33
Pressure ulcers represent a chronic wound with an eschar that presents a nidus for bacterial proliferation and rapid formation of a biofilm. Chronic infections are fundamentally different than acute infections, and different interventional approaches are necessary to treat these biofilm infections more efficiently. We have shown that photoactivated flavin-impregnated collagen films are capable of significantly reducing bacterial contamination and that this effect increases with successive treatments. The experiments reported herein are the first to our knowledge to utilize the murine pressure ulcer model as a platform to investigate infected or contaminated pressure ulcers in a small animal model. We have demonstrated that these wounds can be reproducibly formed, infected, be treated, and nondestructively monitored over time. Future studies should be undertaken to expand these initial observations and to determine the optimal frequency of treatments that would be required to result in reduction of bacterial counts to zero or near zero.
It is believed that the antimicrobial properties of light-exposed riboflavin and its flavin byproducts occur as a result of the release of oxygen free radicals in combination with the generation of nucleotides that preferentially interrupt the RNA or DNA of pathogens. Development of resistance is unlikely, given the mechanism of action of these compounds. Such a strategy could potentially be effective against a broad spectrum of pathogens including bacteria and viruses.
Both ultraviolet and blue light wavelengths have been demonstrated to have antimicrobial activity, 11 –13, 15 –18 However, the applicability of these wavelengths to clinical use is limited in effectiveness because of lack of penetration and a distance dependency from the light source result in nonhomogeneous microbial inactivation. The PCF strategy increases the concentrations of reactive oxygen species (ROS) at or near the target tissue, which are available for diffusion to deeper layers adjacent to the primary area to which they have been applied. Preliminary in vitro studies conducted in our laboratory using conventional and biofilm bacterial culture techniques 24 suggest that the ROS produced after light exposure are stable for a sufficient period of time, such that PCF films which were photoirradiated prior to placement are capable of inhibiting bacterial growth. This may make it possible to treat wounds with these materials without the need to photoradiate the wound itself. However, we did not investigate this alternative in the present studies. Future experiments will explore this strategy.
Collagen is a good source for a drug carrier because it is known to be biocompatible and bioabsorbable. Riboflavin and its light-activated decomposition products are essential nutrients and as such are exploited as a source of ROS, which provide an effective substrate with low toxicity. The chemically modified collagen materials used in these studies have several attributes that are desirable for future clinical use. The material is biocompatible and is pliable. 21 The material conforms to any surface to which it is applied. It is hydrophilic and behaves as a postoperative adhesion preventative when placed intraabdominally. 20,22,23 The material can be used as a carrier for biologically relevant molecules and chromophores, and can be designed to dissolve and be reabsorbed over a specific period of time by adjusting collagen photophysical properties. These attributes facilitate the application of a precise dose and controlled release of an optimized flavin mixture as an antimicrobial agent with accurate placement to effectively manage wound bioburden.
There is a need for the development of novel strategies to reduce levels of contamination in acute and chronic wounds. The use of flavins as a photosensitizer that produces ROS after photoactivation with blue light represents an opportunity to achieve antibacterial effects with low toxicity in contradistinction to antibiotics and typical agents utilized for classic photodynamic therapy applications. Future studies are necessary to determine and optimize the frequency of dressing changes and parameters and frequency of light exposure necessary to achieve maximal antimicrobial activity. These studies should also investigate and contrast pretreatment of the collagen-flavin composites with in situ activation, as is reported in this series of experiments. Other work should explore the use of this modality as an adjunct to traditional wound care and antibiotic therapy.
The present studies utilized prototype laser sources with blue light emissions spectra within the optimum range for riboflavin photoactivation as documented in our in vitro studies 24 and the absorption peaks for riboflavin and lumiflavin. 14 Daily photoradiation alone (R) and PCF alone groups were not evaluated in the multiple treatment study (experiment 2) based on the results obtained in our prior pilot studies 24,25 as well as the fact that there was no difference observed between C and R groups in the single treatment experiment (experiment 1). The results of the multiple treatment study should be confirmed with larger numbers, and with a daily photoradiation group, in light of the work of others demonstrating the antimicrobial effects of blue light alone in some scenarios. 14 –17
Wound infection and related complications increase the cost of care and prolong hospital stays. There is increasing pressure to reduce wound infection rates with various strategies, including the Centers for Medicare and Medicaid Services (CMS) “no-pay” initiative for certain hospital acquired infections. 34,35 Wound care strategies that are easily applied and that could reduce primary or secondary wound contamination would improve wound care and patient outcomes. Further development of photoactivated collagen technology is warranted.
Footnotes
Acknowledgment
This work was supported by National Institutes of Health (NIH) National Institute of General Medical Sciences (NIGMS) Grant # 1R43GM087753-01.
Author Disclosure Statement
Drs. Lanzafame and Stadler have intellectual property rights with Conversion Energy Enterprises. Drs. R. Stoltz and B. Stoltz are owners and have an equity position with Conversion Energy Enterprises. Drs. Cunningham, Muhlbauer, and Griggs have no disclosures or conflict of interest with this content.