
Abstract
Introduction
Generally, a 0.2% CHX solution is used as an irrigant for root canal treatment, but a 2% solution of CHX gluconate can also be used. 5 CHX is a bis-bis-guanide with amphiphatic and antiseptic properties. 6 Bryce et al. 7 found that CHX reduces the number of Enterococcus faecalis cells recovered from biofilm, and that most of the attached E. faecalis cells were nonviable after CHX treatment. However, others have found that the effect of CHX as an antibiofilm is limited. 8,9
For several decades, the most widely used root canal irrigant has been NaOCl. 10,11 Whereas its excellent properties of tissue dissolution and antimicrobial activity make it the irrigant of choice in the treatment of teeth with pulp necrosis, it nonetheless has several undesirable characteristics. Teeth with wide open foramina or with apical structures damaged by resorption or by iatrogenic errors during instrumentation are at elevated risk for extrusion of NaOCl 12 Extrusion of a small quantity of NaOCl through the apical foramen can trigger severe pain, burning sensation, and periapical tissue damage. 13,14 Other risks include tissue toxicity, emphysema overfilling, allergenic potential, and a disagreeable smell and taste. 15 Although effective, NaOCl does not fully clean the surfaces of root canal walls, 16 but is generally found to be more effective than CHX in this regard. 5
Ethylenediaminetetraacetic acid (EDTA) irrigant is generally used after instrumentation because of its chelating action, which removes the smear layer. However, extended use of EDTA or its association with NaOCl at high concentrations might cause excessive dentin erosion 17 and considerable reduction in dentin microhardness. 18,19
Recent advances in dental research have incorporated laser technology as an important modality in endodontic therapy. Development of new laser delivery devices, including thin and flexible fibers as well as new endodontic tips, has made it possible to apply this new technology for cleaning and disinfecting the root canal system. Stabholz et al. 20 reported on the development of a new endodontic tip that can be used with the Er:YAG laser system. The Er:YAG laser beam is delivered through a hollow tube, enabling lateral emission of the irradiation (side-firing), rather than direct emission through a single opening at the far end of the tip. This new endodontic side-firing spiral tip was designed to fit the shape and volume of root canals prepared by Ni-Ti file rotary instrumentation. It emits Er:YAG laser irradiation laterally onto the walls of the root canal through a spiral slit located along the tip. The tip is sealed at its far end, preventing transmission of irradiation to and through the apical foramen of the tooth. 21
Laser-activated irrigation (LAI) has been introduced as a powerful method for root canal irrigation. 22 –24 The effect is based on cavitations: in an aqueous environment, activation of the laser at ablative settings may form large elliptical vapor bubbles that can expand and then implode. These vapor bubbles can cause a volumetric expansion of 1600 times the original volume. 25 which in turn causes high pressure that drives fluid out of the canal. When the bubble implodes after 100–200 ms, under-pressure develops that sucks fluid back into the canal, inducing secondary cavitation effects. LAI can result in smear-layer removal from the root canal wall, but can also cause extrusion of irrigant through the apex. 23,24
The aim of the present study was to evaluate the effectiveness of LAI by using Er:YAG laser irradiation with a side-firing spiral tip combined with different irrigation solutions inside the root canal in order to eradicate E. faecalis biofilm.
Materials and Methods
Distal and palatal roots from 60 freshly extracted human molars were used in this study. Radiographs of each tooth were taken from two different angles prior to the endodontic procedure. The working length of the root canal was determined by an apex locator and radiograph with file no 15, 20. This step was accomplished with intracanal irrigation with 2.5% NaOCl. Endodontic preparation was performed using Protaper™ (Dentsply Maillefer, Baillaigues, Switzerland) F3 Ni-Ti files with irrigation solution 2.5% NaOCl. The coronal of each tooth was removed. Roots were split longitudinally in a meso-distal direction with an ultrathin diamond bur. The roots were imbedded into impression material to obtain their pattern. The two halves of the split root were placed in an ultrasonic bath to remove the smear layer from the root canal walls, thereby creating conditions for the formation of E. faecalis biofilm.
The split teeth were sterilized in an autoclave for 20 min at 121°C. To verify sterilization, they were incubated in brain heart infusion broth (BHIB) for 48 h. After ensuring sterility of the split teeth, the tested teeth were exposed to E. faecalis (from the stocks of the Institute of Dental Sciences, Faculty of Dental Medicine, Hebrew University of Jerusalem) for 3 weeks at 37°C. Every 2 days, two thirds of the broth medium (BHIB) was replaced with fresh BHIB. The BHIB medium was examined periodically for bacterial contamination. At the end of the incubation period, the two halves of each split root were put back together in the dental impression material to recreate the configuration of the original root canal.
The 60 roots were randomly divided into two main groups. The first group contained 30 teeth that were rinsed with three different irrigation solutions: 10 with CHX, 10 with EDTA and 10 with saline. The second group contained teeth undergoing laser irradiation with the same irrigation solutions.
The tested solutions–2% chlorhexidine, 17% EDTA, and saline–were injected with a 27-gauge endodontic needle (Navitip, Ultradent, South Jordan, UT), 10 mL during 60 sec. The needle was inserted 1 mm short of the working length and moved slowly up and down along the root canal.
The second group of irrigation included Er:YAG laser (Opus 20, Lumenis Opus Dent, Yocneam, Israel) with the RCLase™ side-firing spiral tip, flexible, with dimension of 0.4 μm that could be banded according the morphology of the root canal. It is a single use tip that can emit the laser beam onto the lateral root canal wall. The end of the tip is closed, ensuring that all of the energy is directed to the root canal wall. The laser tip was inserted 1 mm short of the root bottom. The laser light was emitted with a pulse energy of 500 mJ at a frequency of 12 Hz for four cycles of 15 sec each, giving a total of 60 sec irradiation with 10 mL of irrigation solutions: CHX (2%), EDTA (17%), or saline.
Scanning electron microscopy
The tested samples were dried and mounted on stubs and then coated with Au/Pd by Polaron SC7640 Sputter Coater (Polaron, Hertfordshire, UK). The effect on elimination of E. feacalis biofilm by the irrigation solutions with or without laser irradiation was examined by scanning electron microscope (SEM) at a high magnification of×10,000 and×50,000. The samples were examined by FEI Sirion High Resolution SEM and FEI Magellan Ultra-High Resolution SEM (FEI, Eindhoven, The Netherlands).
Microanalysis of element distribution by energy dispersive X-ray spectroscopy
The chemical surface content of the root canal following laser irradiation was evaluated. All samples were analyzed by FEI Quanta 200 SEM (FEI, Eindhoven, The Netherlands) equipped with an EDAX (Tilburg, The Netherlands) energy-dispersive X-ray spectroscopy (EDS) system (Sapphire Si[Li] ultrathin window [UTW] detector, 10 mm2, spectral resolution 128 eV) with accelerating voltage of 15.0 kV, spectra acquisition time of 50 sec, and dead time of ∼15%. The EDAX ZAF matrix correction was applied for quantifications. Differences in surface distribution of key elements in dentin, such as Ca, P, and O, were evaluated. Spectra acquisition and quantification were performed using EDAX Genesis software. Element content was determined in wt% and all measured values were compared with controls.
Statistical analysis
The Kruskal–Wallis nonparametric ANOVA was applied to test the statistical significance of the differences between various treatment groups; each subgroup contain 10 specimens, for Ca, P, O, and the Ca/P ratio in dentin. Comparison of two groups, that were laser and non-laser treated, was performed using the Mann–Whitney nonparametric test. A p value≤0.05 was considered statistically significant. Data are presented as mean±SD.
Results
Examination of surface morphology
The dentin surfaces of the root canal wall were observed by SEM. Figure 1 illustrates a heavy layer of E. faecalis biofilm that covered the dentin surface of the canal wall and obliterated tubule orifices in the control group.
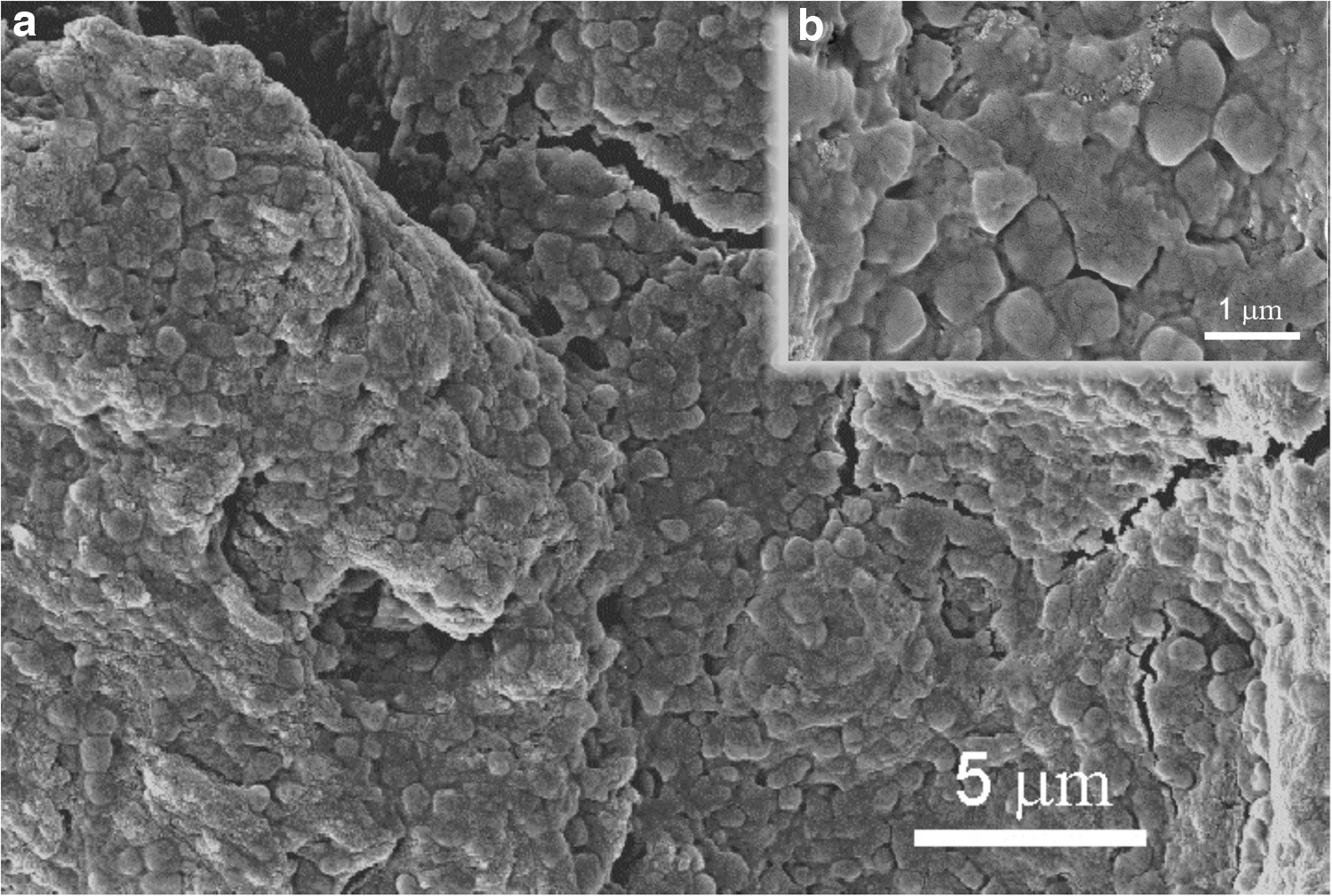
Control Enterococcus faecalis biofilm.
Persistent bacteria were observed on the root canal wall after application of the 2% CHX irrigation solution, which did not eliminate the surface-adhering bacteria from the inner spaces of the dental tubuli (Fig. 2). However, significant reduction in E. faecalis was observed when the canal was treated with the CHX irrigation and laser irradiation combination (Fig. 3). Bacteria were found colonizing only one section of the dental tubules.
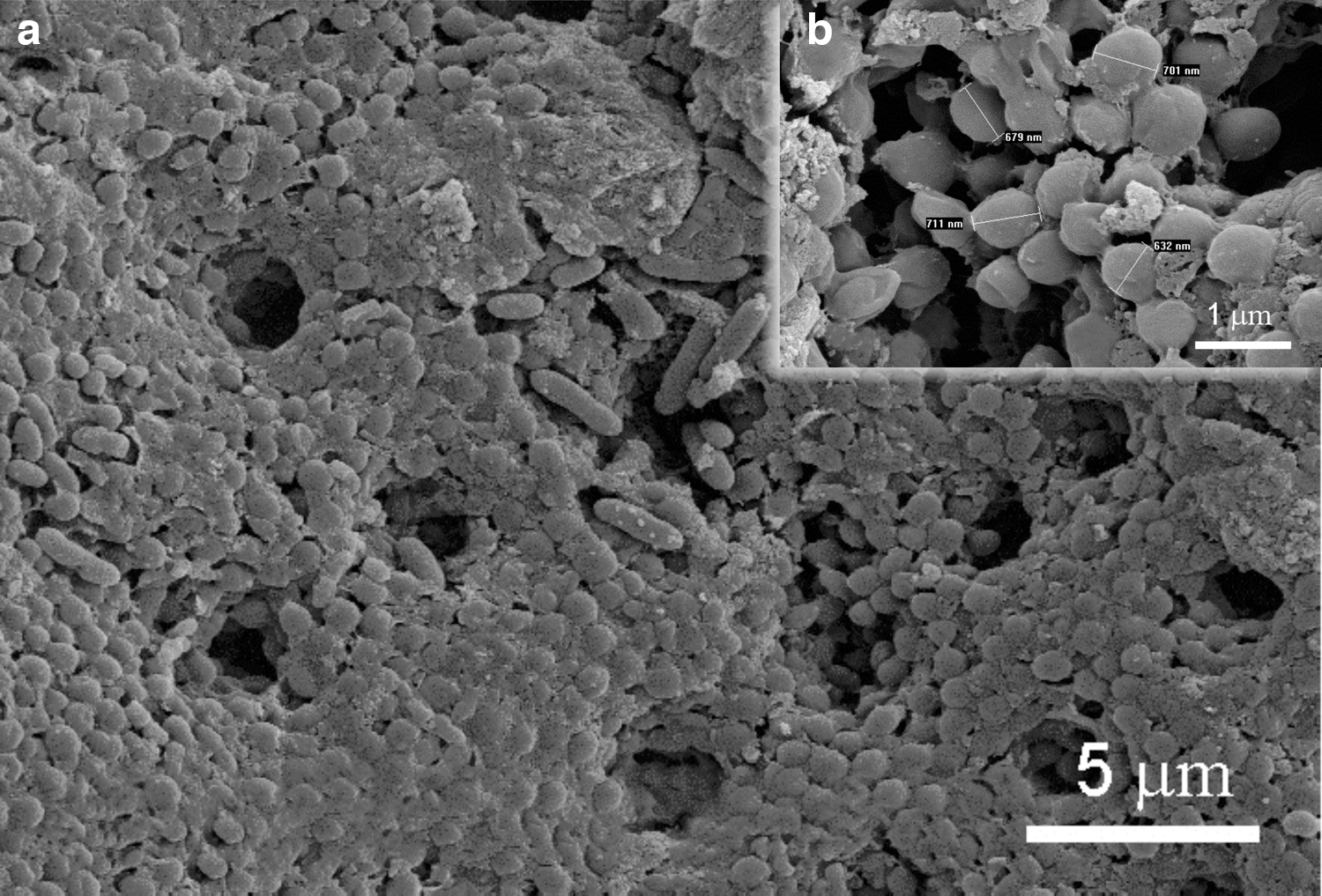
Chlorhexidine (CHX) irrigation of Enterococcus faecalis biofilm.
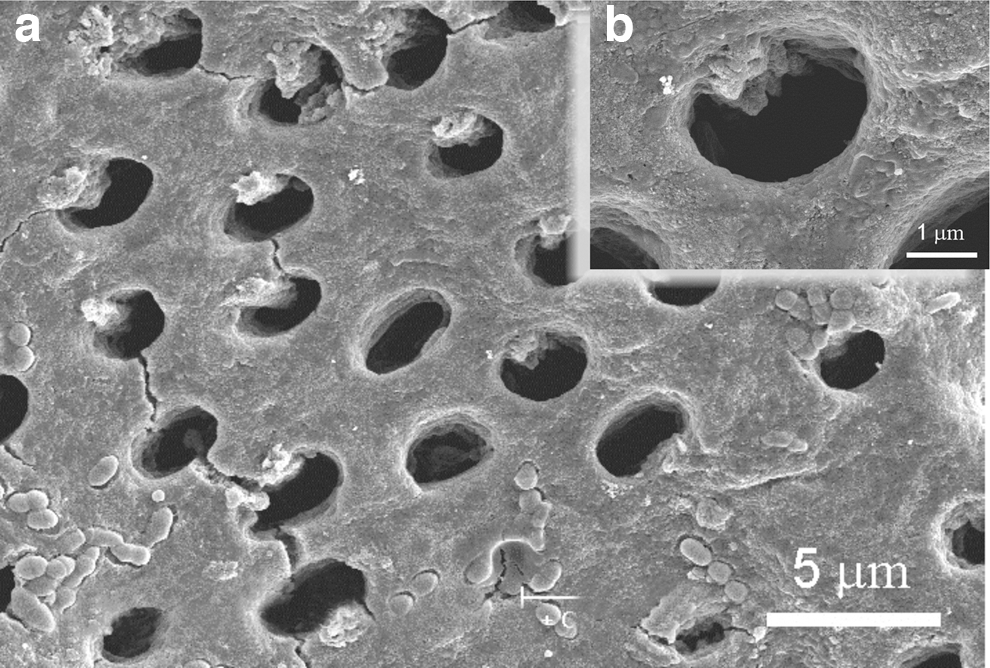
Laser treatment+chlorhexidine (CHX) irrigation of Enterococcus faecalis biofilm.
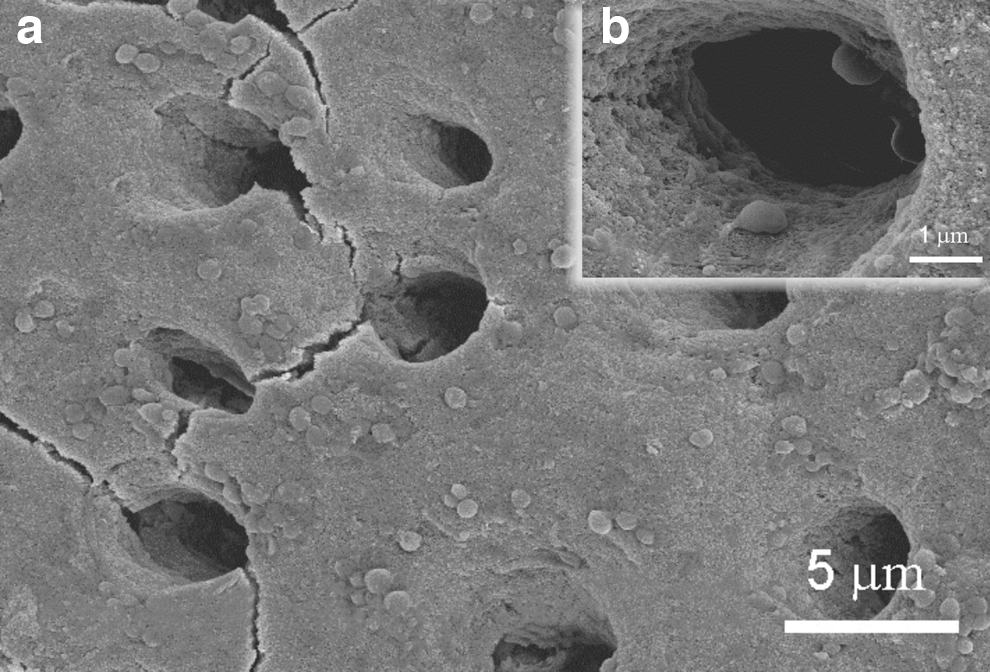
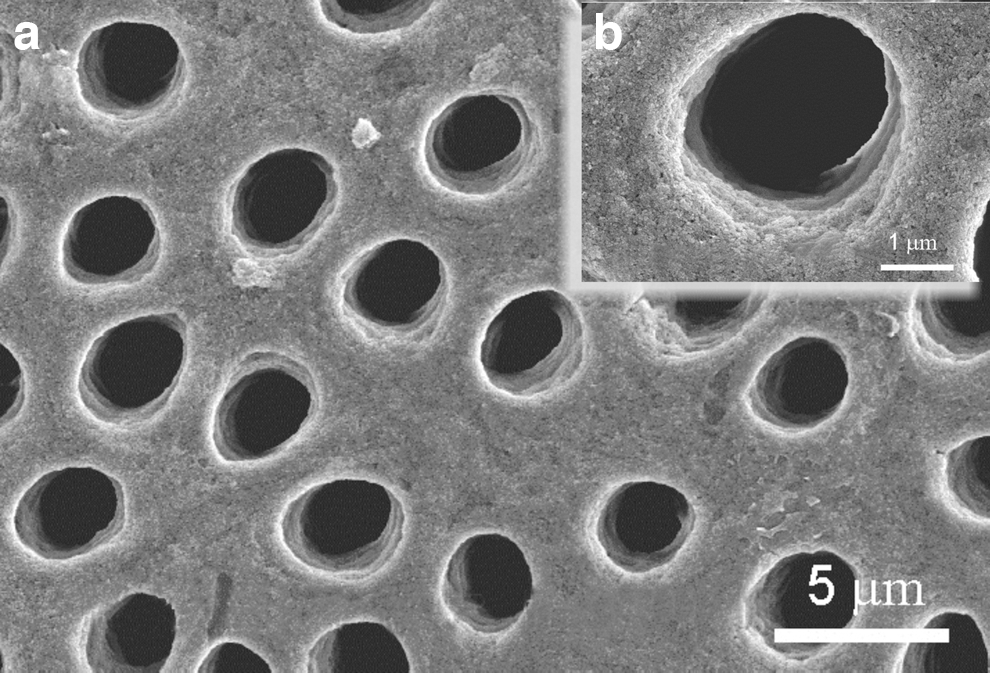
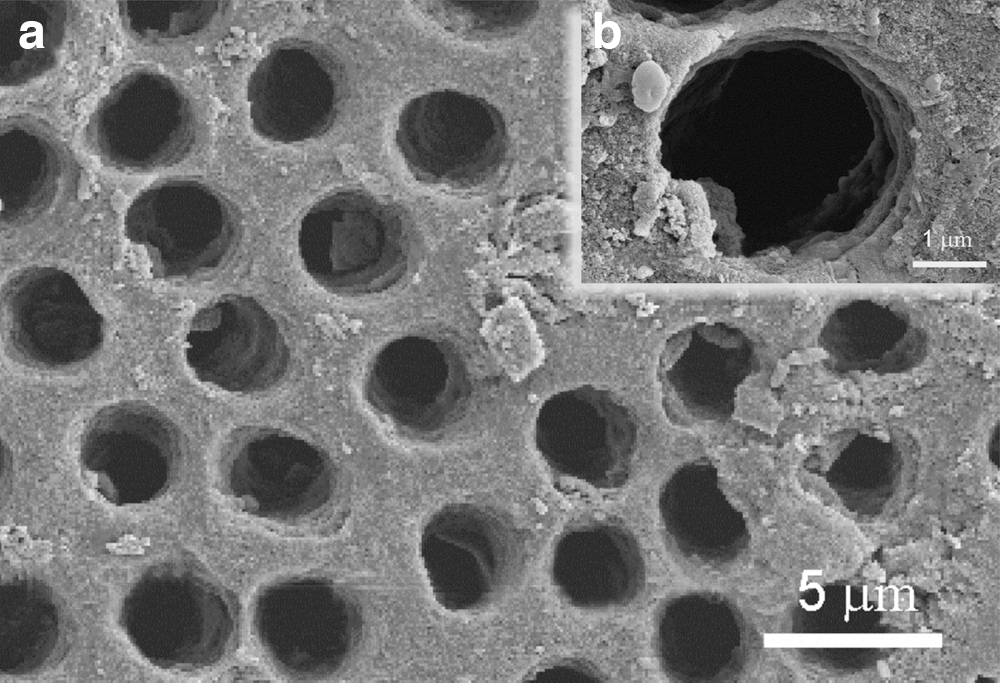
Application of the 17% EDTA solution significantly decreased the quantity of adhered E. faecalis (Fig. 4). Combining this irrigant with laser irradiation maximized the effectiveness of bacterial removal from the root canal walls. The SEM images show that the root canal and tubules surfaces are almost completely devoid of the microorganisms (Fig. 5).
Ethylenediaminetetraacetic acid (EDTA) irrigation of Enterococcus faecalis biofilm.
Laser treatment+ethylenediaminetetraacetic acid (EDTA) irrigation of Enterococcus faecalis biofilm.
Use of saline as the irrigation solution had no effect on bacterial removal, as evidenced by the heavy layer of bacteria covering the surface of the root canal wall (Fig. 6). When this treatment was combined with laser irradiation, some areas remained covered with biofilm, whereas other areas appeared to have open tubules in the canal wall (Fig. 7).

Saline irrigation of Enterococcus faecalis biofilm.
Laser treatment+saline irrigation of Enterococcus faecalis biofilm.
Surface chemical analysis
The mean surface levels of Ca, P, O and the Ca/P ratio in dentin following irrigation alone or the combination of laser irradiation with irrigation solution are illustrated in Figs. 8 and 9.
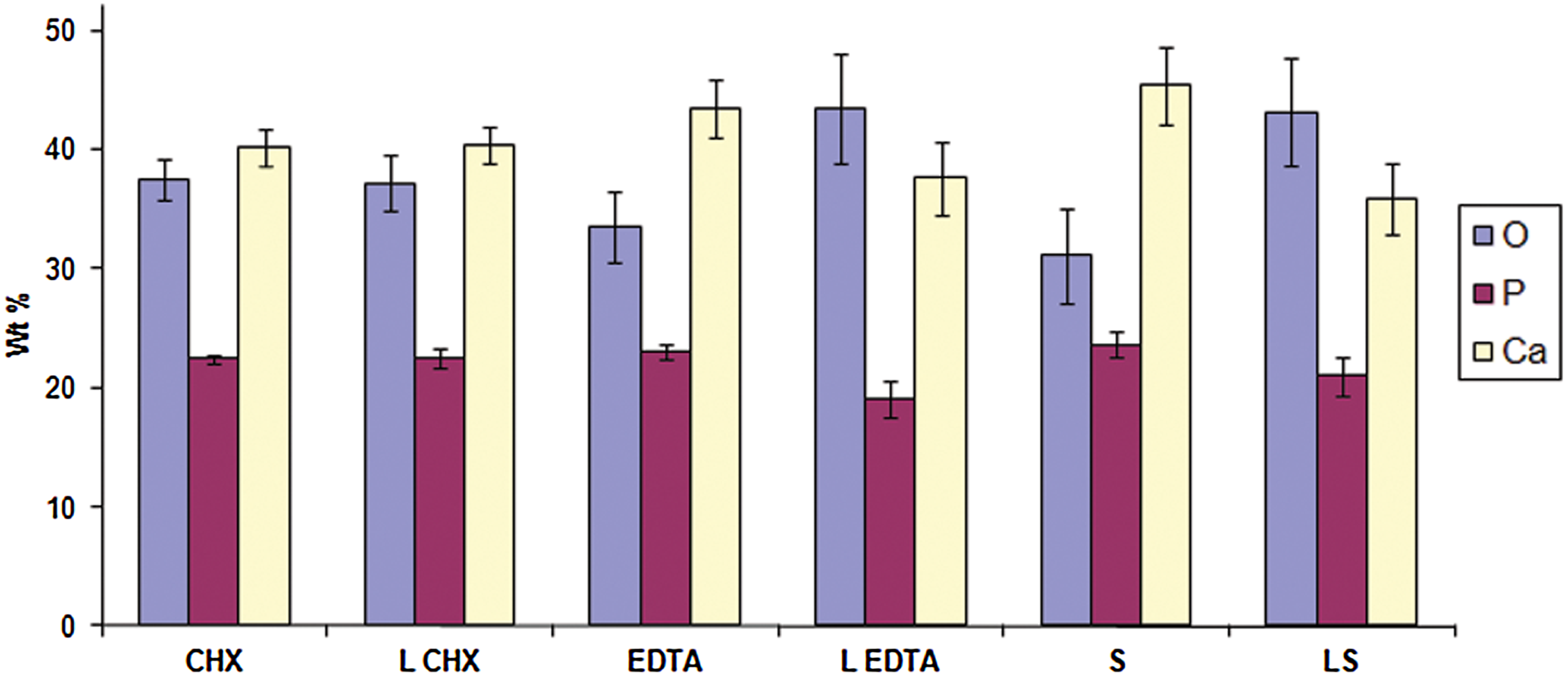
Mineral analysis of the root canal surface after rinsing with irrigation solution alone or in combination with Er:YAG laser treatment.
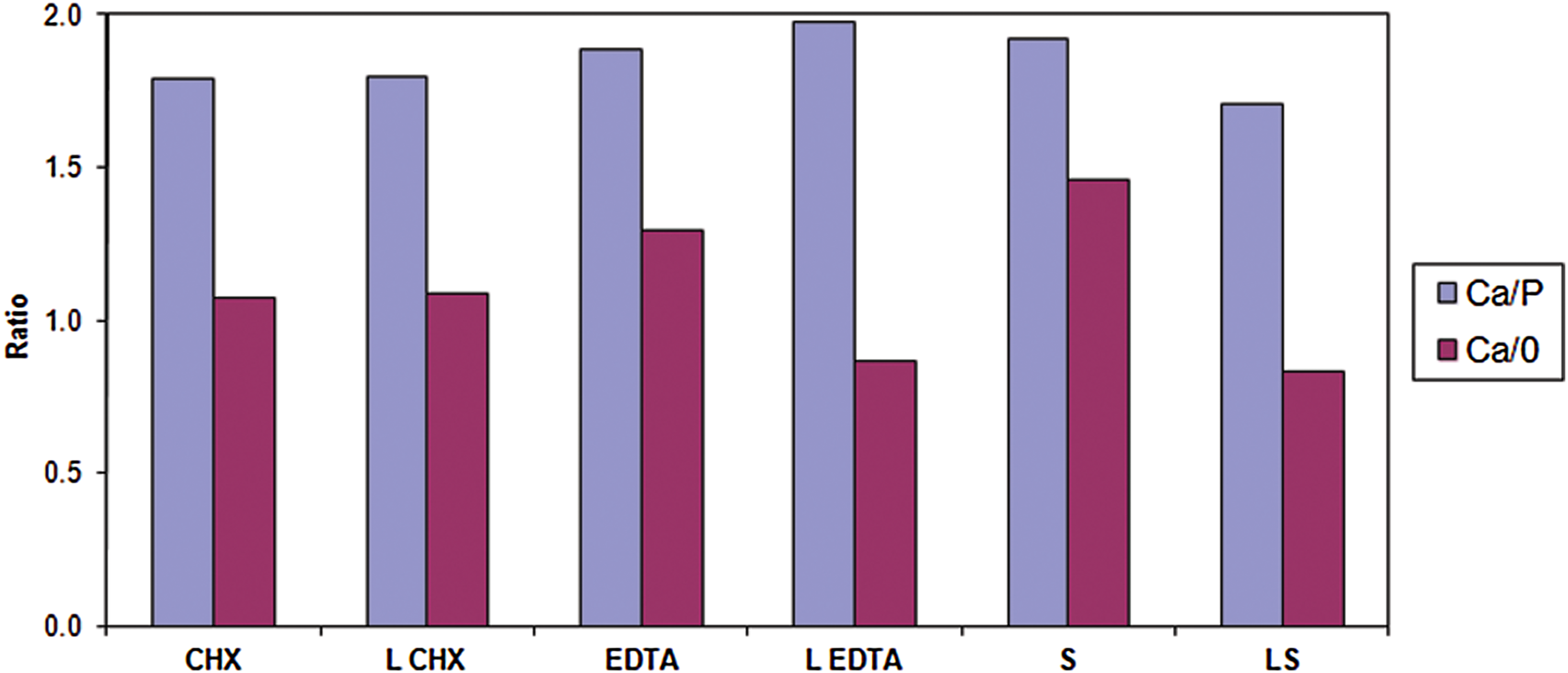
Changes in Ca/P and Ca/O in the dentin root canal walls after rinsing with irrigation solution alone or in combination with Er:YAG laser.
Oxygen content was lowest in the saline with laser group, whereas EDTA showed the highest quantity of surface oxygen compared with the other irrigation solutions (Fig. 8). Changes in P level were minimal in all tested samples.
In general, all samples treated with laser irradiation and irrigation had low concentrations of Ca in all groups compared with samples treated with irrigation alone. The Ca/P ratio was highest in the laser-EDTA group. Relative Ca levels were highest in the EDTA-treated group, whereas the lowest levels were recorded in the saline with laser group. Figure 9 shows that the Ca/P ratio was highest in the laser with EDTA groups, and lowest in laser with saline group. None of the above differences in surface mineral distribution of the root canal dentin were statistically significant when compared among the tested groups.
Discussion
The goal of endodontic therapy is to reduce or eliminate microorganisms and their byproducts from the root canal system. Although there are a number of instrumentation and irrigation techniques for this purpose, complete elimination of bacteria is not always achieved in clinical practice. 26 Therefore, alternative routes to eliminate bacteria from the canal are being explored. Laser may be one of these alternatives that needs to be further explored.
In our study, we used the split root technique, based on prior experience. The split roots are imbedded together in the impression material, which recreates the original root canal configuration. This enables reassembly of the two halves of the tooth back to its original form, with no leakage of fluid from the contact area between the two halves. This method allows us to clean the root canal thoroughly, contaminate the canal with bacteria, and examine the surface of the root canal directly, without any interference on the biofilm or mineral content.
A combination of laser irradiation and irrigation of the root canal can provide effective elimination of the smear layer from the dentin wall. 27 For example, application of Er:YAG laser irradiation combined with CHX to a bacterial suspension was found to have a synergistic inhibitory effect on bacterial growth for 18 h. 28 Er,Cr:YSGG laser irradiation, with or without 5.25% NaOCl, was tested for elimination of Candida albicans. The greatest reduction was achieved when the two treatments were combined. 29
Laser energy emitted from the tip of an optical fiber or laser guide was directed along the root canal, but not necessarily lateral to the root canal walls. 21 This type of emission may result in transmitting irradiation beyond the foramen and can be hazardous in teeth that are in close proximity to the mental foramen or mandibular nerve. 20 In our study, the Er:YAG laser beam was delivered through a hollow tube, with an endodontic tip that allowed lateral emission of the irradiation (side-firing) through a spiral slit located along the tip. The tip was sealed at its far end, preventing irradiation transmission to and through the apical foramen. Because of the configuration of this novel tip, the Er:YAG laser generated rapid agitation of fluid, 30,31 which could improve disinfection against biofilm bacteria. The motion of the novel RCLase side-firing spiral tip facilitated energy beam delivery to all root canal surfaces. In this study, we sought to determine the dose-dependent effects of irradiation on the adhered bacteria and mineral content of the root canal. Consequently, some of the energy dosages we employed were experimental in nature, and apparently not to be used clinically. According to Gabrić Pandurić et al., 32 in experimental study, Er:YAG laser removed significantly more bone tissue when they used pulse energy 1000 mJ; pulse duration, 300 μs; frequency, 20 Hz.
Studies on modes of action and efficiency of various chemical irrigation solutions have shown their direct effect on both organic and inorganic components of the root canal dentin. Given its well-known antimicrobial properties, NaOCl is the most commonly used irrigant, but it can also reduce the modulus of elasticity and flexural strength in the dentin. 33 NaOCl at pH 7.4–11.5 was found to cause 70% protein depletion from a hydroxyapatite surface. 34 Depletion of the organic phase after NaOCl treatment caused mechanical changes. Other studies have also reported that NaOCl decreases dentin microhardness under continuous irrigation with 2.5% or 6% NaOCl for 5, 10, or 20 min. 35
In our study, we limited the use of the irrigation to 1 min in order to eliminate the potential side effects on the dentin surface. The chemical constituents of the dentin wall of the root canal are of the utmost importance in the endodontic treatment's success, as demineralization of the walls may affect the root canal and tooth structure. We monitored the changes in Ca and P in the dentin root canal walls after treatment, and found them to be minimal. All samples treated with laser irradiation and irrigation had slightly lower levels of Ca than samples exposed to irrigation alone. Hossain et al. 36 examined the influence of Er:YAG laser and bur on cavity floor preparation, and no significant differences were found in the Ca/P ratio between the laser group and controls. On the other hand, Ari and Erdemir 37 used various irrigation solutions – 0.2% CHX gluconate, 3% H2O2, 17% EDTA, 5.25% NaOCl, or distilled water – for 15 min, and found decreased levels of Ca and P in the dentin following treatment.
The effectiveness of eradicating bacteria from the biofilm is dependent upon the antibacterial agent chemistry and on contact time with the biofilm. 38 CHX is a positively charged molecule 39 that adheres well to surfaces. Clegg et al. 40 evaluated the ex vivo effectiveness of 2% CHX against apical dentin biofilms. However, they reported that the irrigant was incapable of disrupting the biofilm, although it efficiently inhibited initial adherence, and possibly further accumulation of bacteria on the biofilm. 41 In our study, 2% CHX alone failed to remove the biofilm layer. However, when the CHX irrigant was introduced together with laser irradiation, fewer bacteria were recorded in the SEM images. Following laser-induced agitation of the CHX irrigant, the dentin surface exhibited only small amounts of bacteria, accumulating only inside the dental tubules.
The groups irradiated with EDTA solution demonstrated the lowest scores for bacterial biofilm accumulation. Eliminating bacteria from the root canal surface as well as from the entrance to the tubules resulted in open tubules with minimal change in diameter. In contrast, groups with irrigation but no laser treatment showed biofilm on the root canal surface that obscured the dentinal tubules.
Other studies 42 have shown that Er:YAG laser can effectively ablate tissues containing some water, thereby causing less thermal damage to adjacent tissues. Carbonization, craters, cracks, and fractures were not observed in our study, in accordance with the findings of others. 42 –44
Conclusions
Our observations demonstrate the effectiveness of the Er:YAG laser in the removal of biofilm bacteria. This procedure results in efficient cleaning with a low tendency for mineral loss from the root canal dentin. Further in vivo studies are required to confirm the findings presented here, and to establish clinically safe and effective energy dosages to confirm the ability of the Er:YAG laser to remove mixed biofilm without causing a major change in the mineral content of the irradiated dentin.
Footnotes
Acknowledgments
This study was supported in part by a joint grant from the Hebrew University-Hadassah School of Dental Medicine and the Office of the Chief Scientist in the Ministry of Health, Israel. The authors thank Avshalom Tam for his technical assistance.
Author Disclosure Statement
No competing financial interests exist.