
Abstract
Introduction
There have been various materials used to occlude the dentinal tubules for DH. Hydroxyapatite (HAP) is a good biocompatible material that has been studied as a bone substitute in the field of medical science. 4 Moreover, HAP combined with nanotechnology has new physical properties with decreasing particle size. A previous study showed that the amorphous nano-HAP has a significantly higher solubility than the micro-HAP, and that nano-HAP released only calcium, phosphate, and hydroxide ions, as a resource of tooth ingredient. 5 However, the inorganic component of the natural human enamel and dentin is considered to be a Ca-deficient and carbonate-containing apatite phase. 4,6 Moreover, carbonate apatite (CAP) is more similar to the inorganic component of the teeth/bones, 7 and has excellent biocompatibility, compared with hard tissue. 8 Also, nano-CAP (n-CAP) was able to adsorb on the tooth surface well because it has high surface energy and area. 9 Recently, a study reported that the dentifrice, containing 20% n-CAP, was the most effective in occlusion of the dentinal tubules, compared with other conventional desensitizing dentifrices. 10
However, some studies have shown that dentifrice abrasives have variable affinity for the dentin surface and that the retention of the particles, which are occluding the tubules, can be limited during the washing procedure or affected by drinking acidic beverages. 11 –13 The next approach is a professional treatment by applying varnish, dentin bonding agents, or composite resins. Nevertheless, there have been reports that suggest that even these materials could be washed from the tubules by mechanical and chemical stimulus, or might become acid labile with time. 14,15 Even now, more effective methods and materials to treat DH are still being looked for. 16 In addition to these approaches, a new approach has been reported using a combination of two existing methods in the management of DH. 16 –18
Blocking the entrance of dentinal tubules only by a mechanical combination cannot resist the change in the external environment for a long time, compared with that of the fusing. 13,19 Therefore, it is important that the treatment occludes the tubules effectively, and achieves persistent occlusion by sealing the tubules, because of the dynamic intra-oral environment. 20 Although desensitizing dentifrices can occlude the dentinal tubules, they have some limitations in extending the treatment effect of DH. For these reasons, a combination of the different kind of existing therapies has been tried, to treat DH. 21
Since the ruby laser was introduced to dentistry as a new treatment method in 1965, many studies have been performed using lasers for the treatment of DH. 22 –24 He-Ne, diode, CO2, Nd:YAG, Er,Cr:YSGG, and Er:YAG lasers are used as a potential treatment method of DH. 25 In particular, the Er:YAG laser has as a high absorption on the tooth surface; therefore, it has been used as a treatment method on dental hard tissue, and its effects on DH have already been reported. 22,26,27 The mechanism of the laser irradiation is known to occlude the dentinal tubules by partial melting and re-crystallizing the dentin surface, after which it results in not only reduced acid solubility but also provides long-term desensitizing effects. 28,29
A previous study reported that a 2–3 μm deposition layer forms on the dentin surface after toothbrushing with the n-CAP dentifrice. 10 If this biocompatible layer is used as a source of laser irradiation, the effectiveness of the treatment, with minimized damage to the tooth surface, in addition to reducing the sensitivity, can be robust. Therefore, this study examined the effect of the desensitizing dentifrice containing n-CAP and Er:YAG laser on dentinal tubule occlusion, compared with that of the n-CAP treatment alone.
The null hypothesis of this study was that the combination method would not be effective, compared with the n-CAP dentifrice only, for DH.
Materials and Methods
Specimen preparation
Eight freshly extracted intact third molars were used in this study. The teeth were collected from a dental clinic. After extraction, the teeth were stored in a freezer at −20°C as soon as possible until their use. The teeth were sectioned at the cementoenamel junction with a diamond wheel disc. Each root specimen was embedded with acrylic resin, and ground with silicon carbide papers (P600–1200) to expose the dentin surface. The dentin specimens were sectioned to a size of 2×2 mm. To decrease the variation from each sample, the control and the experimental groups were selected from the same tooth. Thirty-two specimens were embedded into acrylic molds, and etched with 6% citric acid for 90 sec, to open the dentinal tubules.
Experimental groups
The control group had no treatment after etching with 6% citric acid. The experimental group was divided into three groups. The n-CAP group was toothbrushed with n-CAP dentifrice (Dentiguard sensitive, Daewoong pharmaceutical CO. Ltd., Hwasung, Republic of Korea) only. The laser group was irradiated with an Er:YAG laser (LI group). The combined group was irradiated with an Er:YAG laser after tooth-brushing with the n-CAP dentifrice.
Desensitizing dentifrices
The dentifrice, used in this study, contains 20% n-CAP. This concentration was used because of its reported occluding effect on the dentinal tubules by Lee et al., 10 and the dentifrice slurries were mixed in a ratio of one to three. Artificial toothbrushing was performed with back and forth strokes under 150g force, using a V8 Cross Brushing Machine (Sabri Enterprises, Downers Grove, IL, USA). The number of toothbrushing strokes was based on the result of a previous study, 10 which reported 50 strokes to be the most effective toothbrushing number for the dentinal tubule occlusion.
Laser irradiation
The laser equipment was a pulsed Er:YAG laser (wavelength=2940 nm; Key laser 3+®, KaVo, Biberach, Germany) and the irradiation condition was an energy of 40 mJ/pulse and pulse repetition of 2 Hz for 40 sec, using a 2060 handpiece. The laser beam was handled in a de-focused mode without water. The handpiece does not need an applicator; therefore, the free beam from the window (diameter=1.3 mm) can be applied directly to the tooth surface with in the de-focusing mode. This laser is controlled by the autofluorescence signal from the tooth surface induced by red-infrared diagnostic laser, emitting energy at 655 nm. This signal is capable of selecting demineralized tooth surface. 22,30 To keep the same diameter of the laser beam, we fixed the handpiece at a 25 mm distance from the surface. The specimen was moved in a zigzag manner for 40 sec. The power of the laser equipment was checked before the study by manufacturer.
Analysis
All specimens were evaluated by scanning electron microscopy (SEM) (S-800 Hitachi Ltd., Tokyo, Japan). The opened dentinal tubule areas and morphological characteristics of the treated surface were evaluated at 3000×magnification, and the thickness of the deposition layer on the cross-sectioned surface was obtained at 4000×magnification.
The degree of occluded dentinal tubules was quantified, using an image analyzer (Image-Pro PLUS, v 6.0, Media Cybernetics, Silver Spring, MD). It was possible to obtain quantitative data for the exposed dentinal tubular areas (μm2) from a SEM image (JPEG) at a constant magnification of 3000 times with 10 μm scale bar. Three horizontal parts were randomly selected from each specimen, and the average area of the exposed dentinal tubules was calculated using the image analyzer. Then, these specimens were cut longitudinally to obtain the cross- sectioned images (4,000×). From these images, five parts were selected randomly, and then the average thickness of the deposition layer between the groups was estimated.
The means of the dentinal tubular area between the groups were compared using one way ANOVA and a Tukey's post-hoc test (PASW statistics 17.0, SPSS Inc., Chicago, IL, USA). A p value<0.05 was considered significant.
Results
The areas of exposed dentinal tubules of experimental groups were significantly different compared with those of the control group (p<0.001). And the thickness of the deposition layer of the LI and combined group were significantly different compared to that of the n-CAP group (Table 1, p<0.001).
All values denote the mean±standard deviation.
The same letter indicates no significant difference at α=0.05 according to a Tukey's multiple comparison one way ANOVA test.
n-CAP, nano-carbonate apatite; LI, laser irradiation.
The n-CAP group showed 87% effective occlusion in the dentinal tubules, compared with that of the control group (Fig. 1), and the surface was covered with fine particles. On the cross-sectioned surface, the deposition of the n-CAP layer was observed on the dentin surface, and the thickness was ∼0.84 μm (Fig. 2).
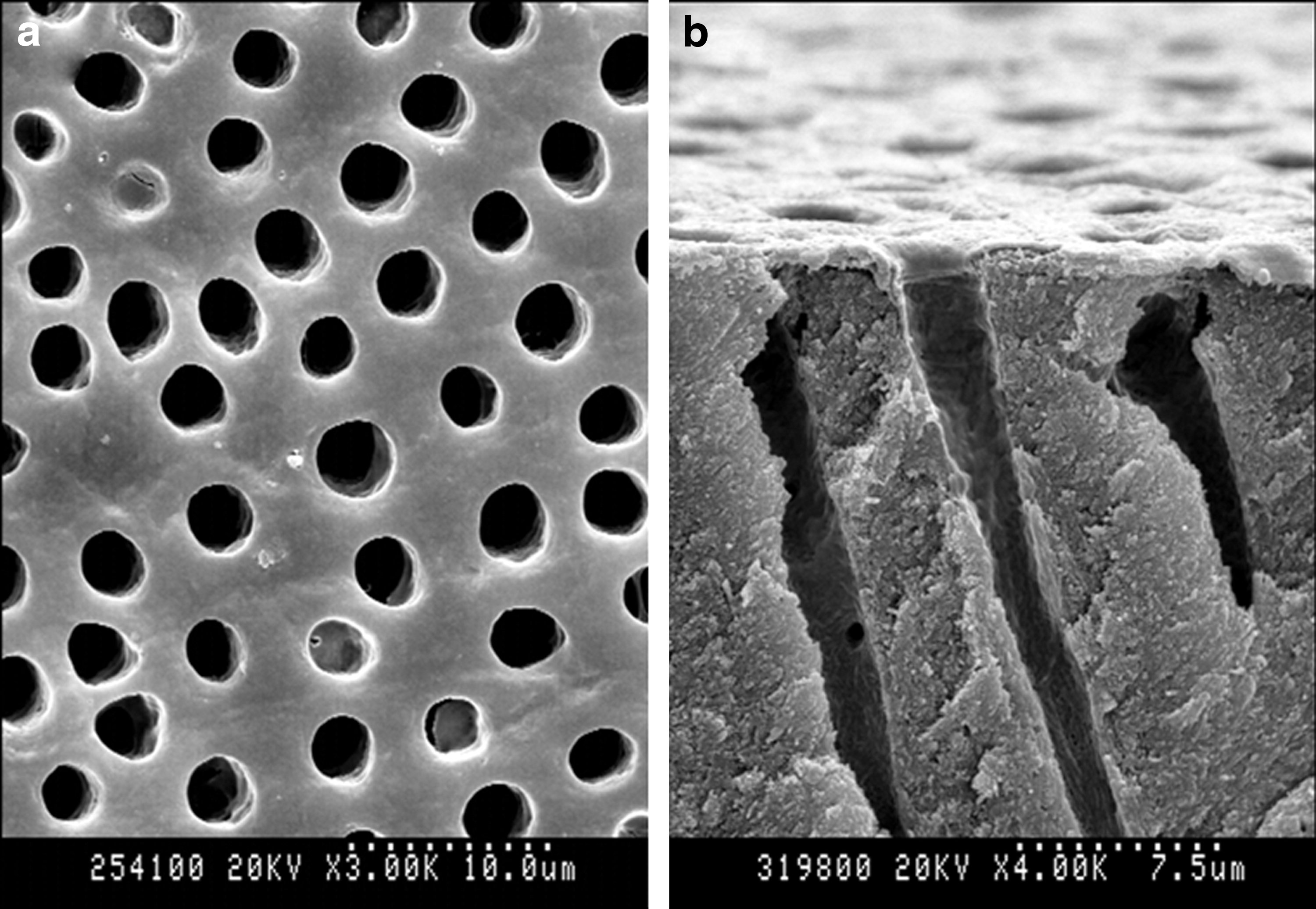
Control group. All the dentinal tubule orifices were opened by 6% citric acid.
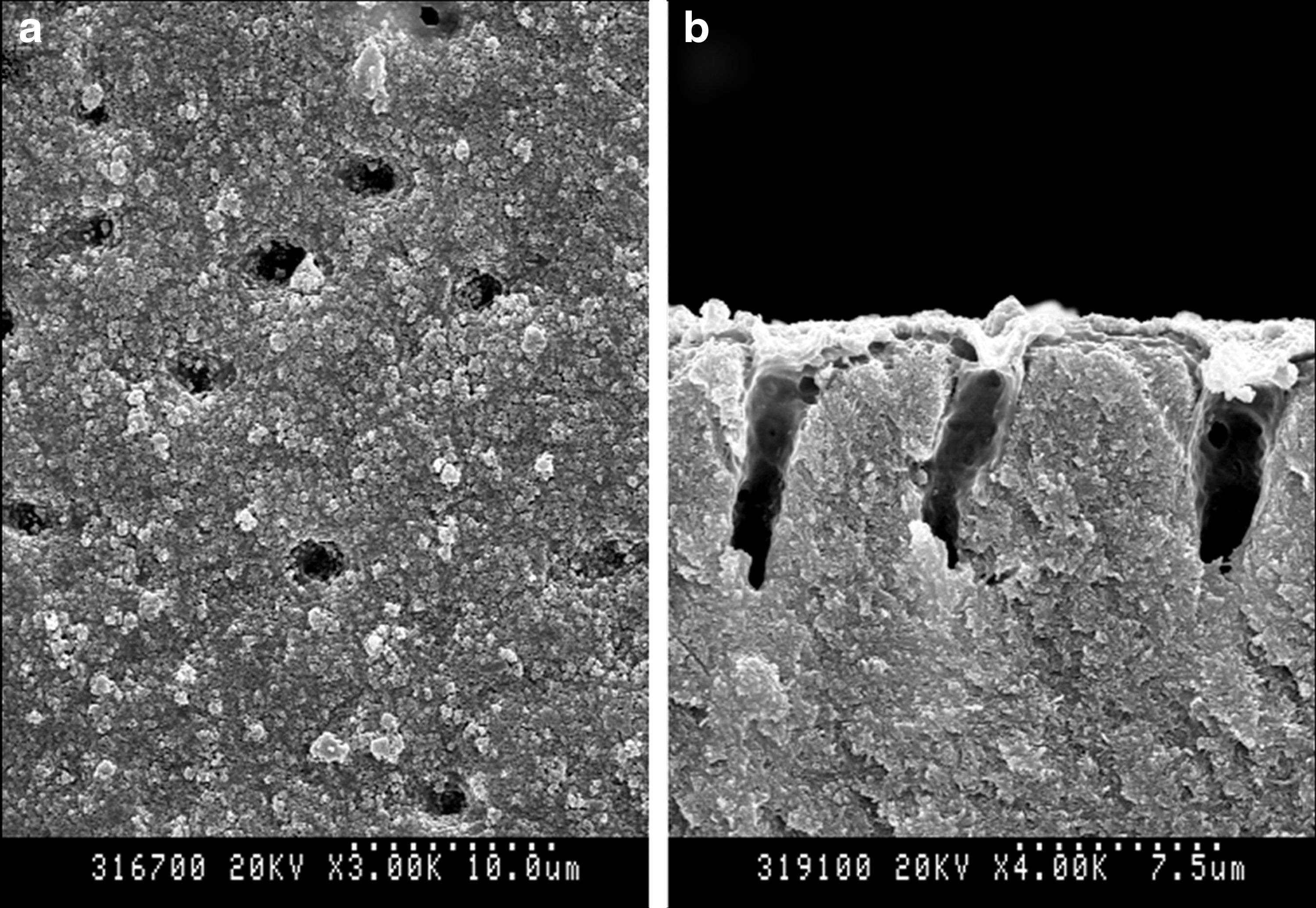
Nano-carbonate apatite (n-CAP) group.
The occlusion effect of the LI and the combined group was 52% and 54%, compared with the control group. The LI group was irradiated with Er:YAG laser, which created a smooth dentin surface with orifices, whereas the combined group was observed to have characteristics of both the n-CAP and LI groups. However, on the cross-sectioned surfaces of both the LI group and the combined group, orifices were observed (Figs. 3 and 4). Also, in the combined group, some of the n-CAP layer on the dentin surface was exposed to laser irradiation, which resulted in n-CAP particles both under and above the irradiated surface (Fig. 4b). In a cross-sectional analysis, the deposition layers of the LI group and the combined group were 2.75 and 2.35 times thicker, compared with that of the n-CAP group (p<0.001).
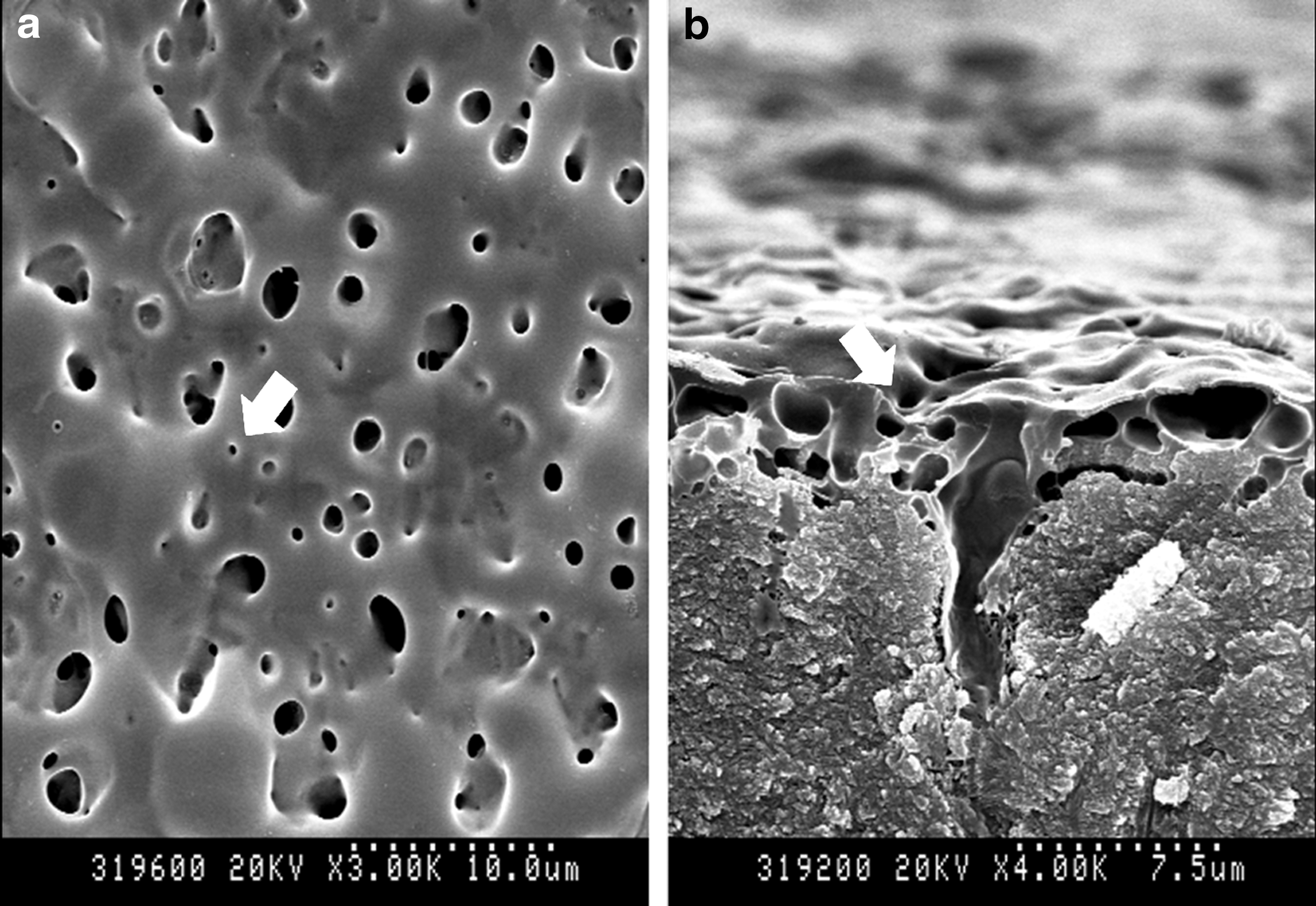
Laser group.
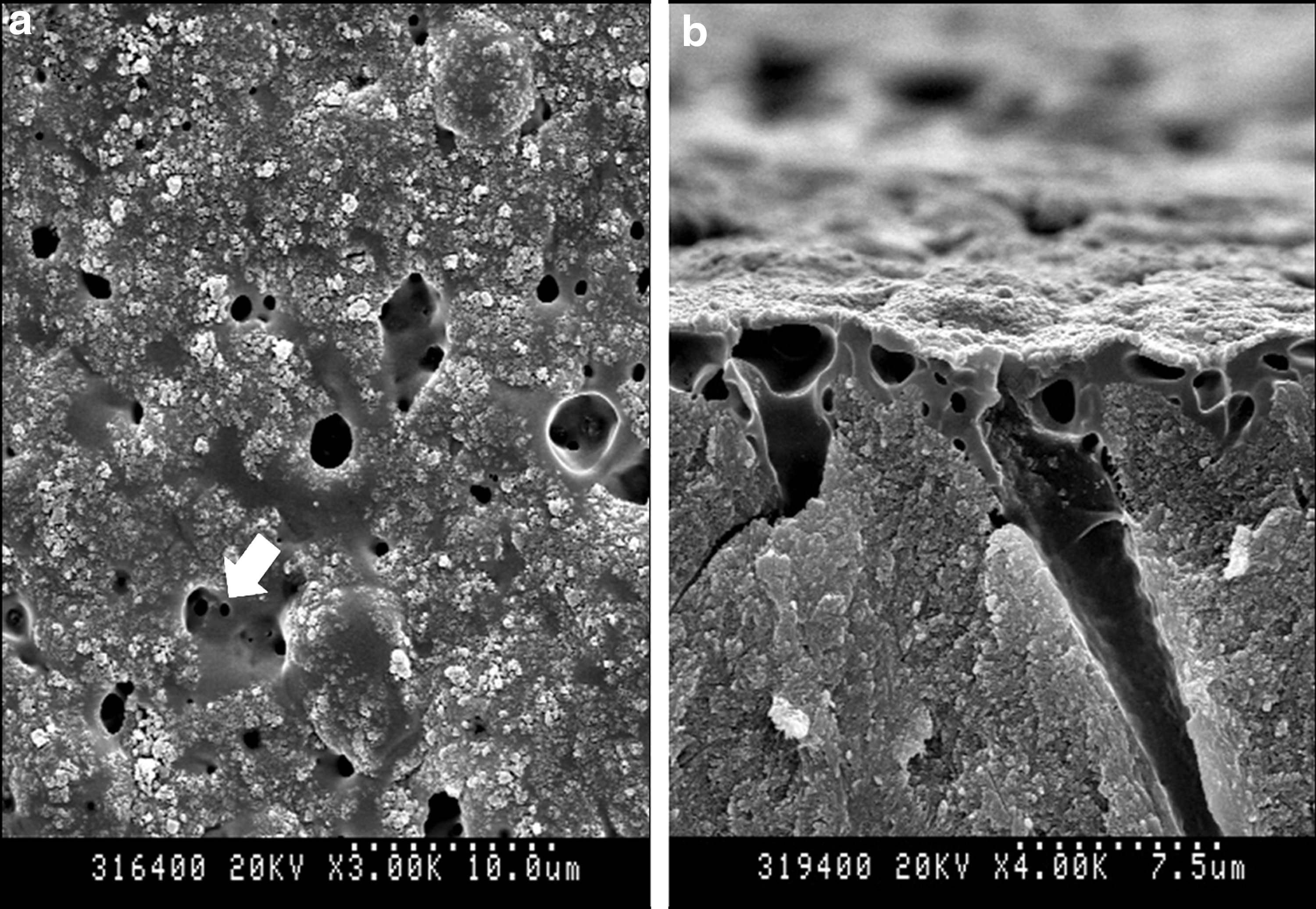
Combined group.
Discussion
The null hypothesis was rejected at the cross-sectioned analysis only. Although the effectiveness of the combined method on the dentinal tubule occlusion was lower than that of the n-CAP group, the thickness of the deposition layer was significantly thicker than that of the n-CAP group.
Occlusion rate of the dentinal tubules of the n-CAP group was 87%, compared with that of the control group, and it was the most effective occlusion rate among the groups (Table 1). These results are in accordance with Lee's study 10 in that 20% of the n-CAP dentifrice group showed an occlusion effect of 80%, compared with the baseline. There was a report that showed that the n-CAP was attached to the enamel surface, so that it significantly prevented re-staining after bleaching. 31 Also, this attaching phenomenon occurred with dentin surface. 10 In this study, a thin layer of 0.84 μm n-CAP was found on the dentin surface. Compared with the n-CAP group, the occlusion effects of the LI and the combined group were lower, 52% and 54%, respectively. In cross-sectional images, however, the thicknesses of the deposition layer of the groups were 2.31 and 1.97 μm, respectively, and they were thicker than that of the n-CAP group.
Low-intensity laser irradiation was capable of occluding exposed dentinal tubules, and the effect was proportional to the duration of irradiation when using the same energy and frequency. 27 In this study, lower energy of 40 mJ/pulse, and pulse repetition of 2 Hz were applied, compared with the manufacturer's recommended settings (energy of 60 mJ/pulse, frequency of 2 Hz), so that minimal invasive effect on dentin surface was expected. The parameter was referred to pilot studies and the distance of 25 mm was set by considering the suitable distance for the 9 molars in the clinic. The LI group was detected as having a thin mineralized layer, and it was the same as the previous studies; 32,33 they reported that a thin mineralized layer was detected in the LI group, and it was found in the previous studies as well because of selective removal of the organic components. On the other hand, the combined group showed that the n-CAP particles penetrated into the dentinal tubules as well as covering the dentin surface (Fig. 4b). This result can be explained by the fact that the n-CAP layer was used as a source to occlude the entrance of the dentinal tubules. Also, the treatment with an Er:YAG laser could be favorable for the attachment of the n-CAP on the dentin surface.
The Er:YAG laser energy is well absorbed into water. Thus, when water remained on the dentin surface after toothbrushing, the laser energy was absorbed to water more than to HAP. 34 As there was no dry process after citric acid treatment or toothbrushing, the specimens could have little water film on the surface. Therefore, it could be assumed that the evaporation of the water molecules occurred before the HAP melted. Sasaki et al. 34 reported porous surface on the dentin after the Er:YAG laser irradiation. This can explain that the n-CAP layer covering the dentin surface in the combined group was removed by water evaporation. Therefore, the occlusion effect was lower than that of the n-CAP group in this study. Moreover, the orifices might have affected the digital analysis because the program detected black orifices on the tooth surface as dentinal tubules. Even if the some of the orifices were not the real dentinal tubules and the result of water evaporation only, the program would calculate the occlusion area with the pore area as well. For improving this inadequacy, we conducted cross-sectional analysis as well, which showed a meaningful different between the groups. Although the water evaporation was affected the analysis, the Er:YAG laser was still effective in decreasing dentinal fluid movement. 18 Also, several studies have shown that laser irradiation caused the decrease in dentin permeability and dentinal pain, 22,35 which could be maintained over time. 24 However, we did not perform the dentinal fluid flow in this study. Therefore further study is needed.
There were hardly any studies that reported combined therapy for DH with Er:YAG laser. However, there have been some studies of Nd:YAG laser. The studies combined 5% sodium fluoride varnish and Nd:YAG laser. 16,17 The deposition layer of the varnish group was reduced by toothbrushing, but in the combined group, because the varnish penetrated the dentinal tubules, >90% of the dentinal tubules were still occluded, even though the external mechanical stimulation was performed. 17 In this study, the image of the cross-sectioned surface of the combined group showed a similar appearance, and the particles of n-CAP penetrated into the dentinal tubules. Another study reported that the treatment effect of the combined group was clinically superior to that of the varnish or the laser group after the stimulation with cold air. In addition, SEM images indicated the superiority of the combined therapy by the reduction of the dentinal tubular areas. 16
In the same context, this study proposed a treatment method, combining at-home and in-office therapies. It was different than the previous studies, which suggested a combination treatment with only the existing professional treatment methods. 16,17 The effect of the dentifrice containing n-CAP was already proven in a previous study, 10 as a biocompatible material, occluding the dentinal tubules well. Although the n-CAP has a higher solubility than that of the microform and can be dissolved in the oral cavity, 5,31 it showed a greater effectiveness for the occlusion of dentinal tubules. 10 Also, other studies reported that it was effective for re-deposition on the damaged region. 31 In this study, although the combined method using the pulsed Er:YAG laser effectively occluded approximately half of the dentinal tubules by the penetration into the tubules, there were some limitations. The instantaneous evaporation of the water by the Er:YAG laser irradiation led to some orifices 29 that blasted away the n-CAP particles from the dentin surface and disturbed tooth surface analysis. However, the meaningful result of this study was that the n-CAP was found under the irradiated surface as well as above the surface in the combined group. The porous surface may help attachment of the n-CAP on the surface, and the irradiated surface can block the way that the n-CAP comes out.
The effectiveness of lasers for treating DH varies from 5 to 100%, depending upon the type of laser and the parameter. 21,36 Also, the irradiated dentin surface is able to increase the resistance to physical and chemical influences. 37,38 This study was the first attempt to evaluate the morphological change by the new treatment method, which is the combination of laser and n-CAP containing dentifrice to enhance the effects of the treatment. In the combined group, despite fewer occluded openings, the layer was thicker than that of the n-CAP group. Thicker layer is expected to produce long-lasting effects of DH treatment, compared with using dentifrice only. Therefore, this combination method seemed that it had the potential for treatment of DH. However, in comparison with the LI group, the difference was not found from the combination method from SEM analysis. Further study is needed to present the combination effects with additional analysis, such as dentinal fluid flow and the long-term effects by acid resistance of this approach.
Conclusions
This study demonstrated the combination therapy of Er:YAG laser and desensitizing dentifrice, containing 20% n-CAP, on DH. The n-CAP dentifrice evenly occluded dentin surface with a thin deposition layer, but the combination with Er:YAG laser showed the possibility for enhancement of the dentinal tubule occlusion. Further studies should be developed with additional analysis, in order to demonstrate the combination effect and the long-term effects of this technique.
Footnotes
Acknowledgments
This research was supported by Basic Science Research Program through the National Research Foundation of Korea (NRF), funded by the Ministry of Education, Science and Technology (R13-2003-013-05002-0).
Author Disclosure Statement
No competing financial interests exist.