
Abstract
Introduction
Pharmacological agents are not the only avenue available to produce a bactericidal outcome. Examples of nonpharmacological agents used to inhibit growth of organisms are ultraviolet light and electrical current. The use of ultraviolet light has long been demonstrated effective in terms of its antibacterial properties. 5,6 Its use in actual patient care, however, has been limited by its potential detrimental effect on human tissue. Kincaid and Lavioe 7 found high voltage pulsed electrical stimulation to inhibit the growth of Staphylococcus aureus, Escherichia coli, and Pseudomonas aeruginosa, but the required treatment times were quite long.
Visible light, as an antimicrobial agent, has been demonstrated to have potential in the treatment of infection. 8 –11 Suggested amendable conditions include the treatment of acne vulgaris 12 and oral bacteria, 10 and the inactivation of Mycobacterium terrae. 13 Results appear to be dependent upon specific wavelengths used and type of bacterial organism. 11 Light has also been shown to facilitate bacterial growth when wavelength and dose are not appropriate. 11
Visible blue light (405 nm) has been shown to be much less potentially harmful to mammalian tissue when compared with ultraviolet irradiation. 14 Guffey and Wilborn 15 demonstrated S. aureus to be susceptible to blue light in vitro at relatively low doses, requiring short exposure times. Another positive aspect of light-based therapies is equal killing effectiveness regardless of resistance to antibiotics. 16 Infected and poorly healing wounds are a major concern in terms of mortality and morbidity, not to mention cost. 17 Many of the common organisms isolated in human wounds are inhibited by blue light. 18 The most current hypothesis suggests that blue light excites endogenous intracellular porphyrins, and that this photon absorption then leads to energy transfer and the production of highly cytotoxic reactive oxygen species, more specifically singlet oxygen. 19 –21
A slightly different form of light therapy for bactericidal action is known as photodynamic therapy (PDT). In this application, red light is employed. PDT, however, requires the addition of a dye that must be absorbed by the target cells. The administered red light interacts with the dye to produce the bactericidal outcome. As Barros et al. 22 have pointed out, there is currently no evidence of microbial resistance to PDT.
The bactericidal potential of visible light is established. What has not been fully investigated is whether organisms susceptible to light irradiation are capable of developing a resistance to certain wavelengths, as they have been able to do for many pharmaceutical agents. The purpose of our study is to determine whether S. aureus has the ability to develop a resistance to the application of blue light.
Methods
S. aureus (ATCC 25923), an organism that grows well in ambient air, was used in this study. The organism was harvested from a 20-h-old culture and added to sterile deionized water to form a suspension equivalent to a 0.5 McFarland standard. Use of a 20-h-old culture is standard microbiological practice and serves to minimize the lag time for new growth. The suspension was further diluted 1/1000 using 100 μL automatic pipettes for purposes of accuracy and reproducibility. All dilutions were made immediately before the treatment with blue light (wavelength of 405 nm).
Using a 10 μL automatic pipette, an aliquot of the 1/1000 dilution of S. aureus was inoculated onto Mannitol Salt Agar (MSA) in 60×15 mm sterile, polystyrene petri dishes. MSA was chosen as a growth medium because it is a selective and differential medium. MSA is selective for organisms able to grow in 7.5% (w/v) NaCl (primarily Staphylococcus species). The medium is also used to differentiate mannitol fermenters (primarily S. aureus) from non-mannitol fermenters (coagulase negative staphylococci). The microorganism was applied to the surface of the plates in a star-streak pattern to enable colony counts to be performed. Therefore, colonies of S. aureus, which were the product of replication by organisms able to survive treatment with light at a wavelength of 405 nm, were subcultured to blood agar plates so they could be subjected to a subsequent exposure at 9 J/cm2. Organisms were removed from the blood agar plate and a suspension equivalent to a 4.5 MacFarland standard was prepared. The bacterial suspension was further diluted 1/1000 using 100 μL automatic pipettes to maintain accuracy and reproducibility. A 10 μL aliquot was then plated on mannitol salt agar and subjected to blue light treatment.
Organisms were treated with 405 nm light at 9 J/cm2. The organisms surviving the initial exposure were designated as stage 1. Stage 1 microbes were subcultured to a fresh growth medium and subjected to a second exposure and then designated as stage 2. This series of exposure-subculture-exposure cycles was repeated until stage 7 was reached. After each exposure and incubation at 37°C in ambient air, a colony count was performed to determine the kill rate. A sharp decrease in the kill rate could be an indication that the test organism was able to develop resistance to the bactericidal effect of blue light. If the kill rate remained relatively unchanged after a series of exposures, this could be interpreted as a failure on the part of the microorganism to develop a mechanism of resistance.
Light exposures were achieved using The Dynatron® 701 Solaris™ manufactured by Dynatronics Corp. (Salt Lake City, UT). This device is designed to accommodate a variety of light probes. For this experiment, we chose to illuminate the cultures using a wavelength produced by an SLD light probe that emitted a band of light focused around the primary wavelength of 405 nm. The probe consisted of a 5 cm2 illuminating surface area comprised of 32–405-nm SLDs with an average power output of 160 mW. Dose was calculated in J/cm2. As output for the probe was held constant, adjustment in time of irradiation provided the dose (9 J/cm2). The Dynatron 701 Solaris automatically calculates time of irradiation when desired dosage is selected.
Data were analyzed using Statistical Package for the Social Sciences Version 20. A one-way ANOVA was employed to compare means. Tukey honestly significant difference (HSD) was used for post-hoc analysis.
Results
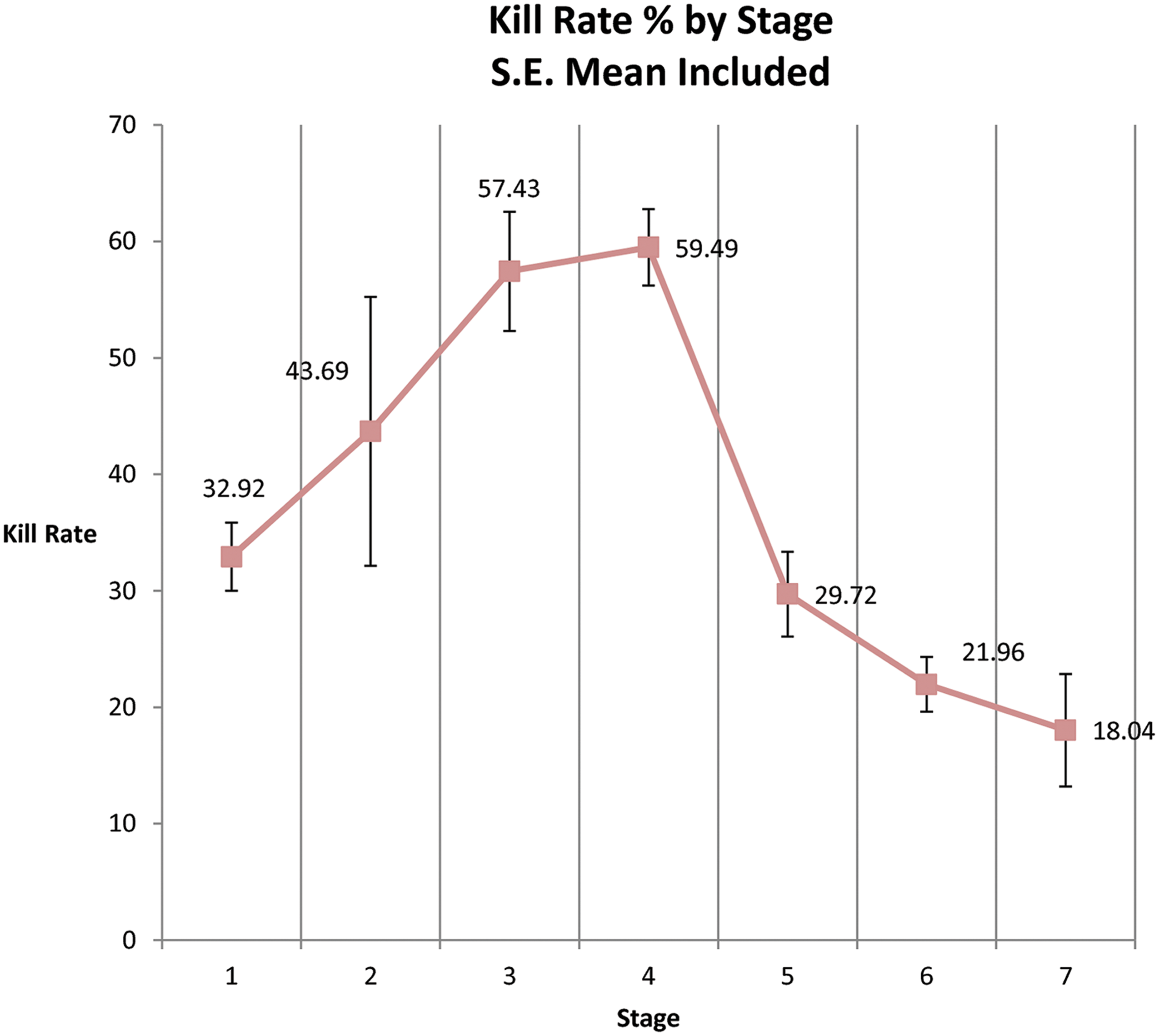
The 405 nm light produced a statistically significant (p≤0.05) bactericidal effect at every stage. Seven total stages were employed to examine the long-term response to the light energy. The observed changes in S. aureus growth at each subsequent stage are reflected in Table 1. These changes were all significant (p<0.05), and 405-nm light was increasingly effective as a bactericidal agent through stage 4 of the experiment demonstrating a 59.49% kill rate. After stage 4 (stages 5–7), the impact of the light energy decayed to a kill rate of only 18.04%, suggesting the formation of a resistance achieved by the organism. Figure 1 graphically displays the observed loss of kill rate. This point is further supported by the ANOVA (F6, 28=8.535, p=0.000). Post-hoc analysis (Tukey) identified stages 2, 3, and 4 as being statistically different from the later stages.
Kill rate of Staphylococcus aureus at subsequent stage of growth after 405 nm light treatment.
Discussion
The ability of bacteria to develop resistance to antimicrobial agents is a well-documented phenomenon, and one that has plagued clinicians since the emergence of penicillin-resistant strains of S. aureus shortly after its introduction in 1946 as the drug of choice to treat staphylococcal infections. 23,24 To further complicate matters, it is an accepted fact that antibiotic resistance can be transferred between different species of bacteria. 25 There has even been speculation that the end of the “era of antibiotics” is approaching, because of the emergence of multi-drug resistant strains of bacteria. 11 It is not surprising, then, that other bactericidal methods are currently under investigation.
Having demonstrated that electromagnetic radiation with a wavelength of 405 nm retards growth of S. aureus, 9,10 it seemed prudent to investigate the possibility that bacteria could develop resistance to this photo energy. Treatment at 9 J/cm2 had historically 9,10 and presently produced a profound negative effect on growth of the organism.
The results of this research continue to support the earlier 15,18 understanding that blue light is an effective agent in terms of inhibiting the growth of S. aureus in vitro. We also observed in this set of experiments that a relatively lose dose (9 J/cm2) of blue light can effectively inhibit the growth of this organism. What we believe to be the most interesting finding associated with this work is the observation that S. aureus has what appears to be an ability to develop a resistance to the application of blue light.
As can be seen in Fig. 1, the effectiveness of the light irradiation improved through four stages of treatment. It was only at the fifth stage of the experiment that we observed diminishing kill rates. This observation continued through the seventh stage. If these results can inform clinical practice, the implication would be that after the fifth administration of an effective light dose, best clinical practice would include the consideration of some alteration in the application of the agent.
Because our intention is to support the understanding related to the clinical use of visible light, we believe that this observation of the potential for resistance development is important. Our review of the related literature yielded no evidence that this phenomenon has been observed to date. Barros 22 has noted that organisms treated with PDT have not been observed to develop any potential for resistance. PDT differs from our experiment in that it usually implies the use of red (∼660 nm) light and incorporates a photosensitizing dye. Accepting the assertion that organisms cannot develop resistance to PDT, it seems likely that some alteration in the application of blue light needs to be developed if the treatment is to be performed in more than four to five stages.
We have considered various strategies for investigating ways to improve the effective kill rate for blue light in the later stages of treatment. One possible strategy would include the incorporation of one or more additional wavelengths. One of our earlier works 18 included light at 880 nm combined with blue light. We are already collecting data to evaluate any impact this wavelength and 660 nm might have on the observed resistance development. Another strategy would be to consider some sliding scale of dose. We have observed multiple doses to effectively inhibit the growth of S. aureus. We now plan to evaluate the impact a changing dose regimen might have on resistance development.
Blue light effectively inhibits the growth of S. aureus in vitro. There is unquestionably a potential clinical application to this finding. We have, however, uncovered evidence that this organism may be able to, over time, develop a resistance to blue light irradiation. Work now needs to be done to determine whether this potential for resistance can be overcome with techniques that would be easily replicated in a clinical environment.
Conclusions
These data lead us to the following conclusions. 1. Blue light at 405 nm has a bactericidal effect on S. aureus in vitro. 2. The effectiveness of blue light irradiation improved through four stages of the treatment protocol. 3. After the fourth stage of the experiment, a declining effectiveness was observed, suggesting the development of a resistance to the treatment. 4. Even though the bactericidal effectiveness of blue light declined in the later stages of the experiment, the kill rates observed were still statistically significant.
Future research should focus on techniques to circumvent this organism's ability to develop resistance to irradiation with blue light.
Footnotes
Author Disclosure Statement
No competing financial interests exist