
Abstract
Introduction
Minimal surface change involving advanced dentinal caries lesions can be difficult to detect. Early caries diagnosis is important so that appropriate preventive and restorative treatment can be provided promptly. 5 Conventional diagnostic modalities for the diagnosis of caries include visual observation, tactile examination by probing that relies on subjective clinical criteria, and dental radiographs. 6 Traditional visual-tactile and radiographic methods of caries detection can detect only lesions that are more advanced, involving at least 300–500 μm of the enamel. Although conventional diagnostic techniques such as visual-tactile methods and radiographs do not appear to have sufficiently high sensitivity or specificity to efficaciously diagnose non-cavitated caries, 6 the activity of caries lesions may be assessed accurately by using the combined knowledge obtained from visual appearance, location of the lesion, and tactile sensation during probing. 7 –9
Various authors have recommended the combined use of visual inspection (VI) and novel diagnostic systems to detect occlusal caries lesions. 10 –12 Novel diagnostic systems are based on the measurement of a physical signal including radiographs, visible light, laser light, electronic current, and ultrasound. 11,12 Noninvasive novel diagnostic methods of early caries detection include optical coherence tomography, fiberoptic transillumination, light-emitting diodes (LEDs), quantitative light-induced fluorescence, laser fluorescence (LF), infrared fluorescence, terahertz pulse imaging, polarized Raman spectroscopy, ultrasound, and electroconductivity measurements. 6
LF is one of the most useful noninvasive diagnostic methods. A red laser light (wavelength, 665 nm) that is produced by a laser diode and transmitted by an optical fiber is absorbed by inorganic and organic tooth substances and by metabolites from oral bacteria in infected dentine. 15 This device uses a numerical scale of which the digital display (in units related to a calibration standard) correlates quantitatively with the intensity of the fluorescence detected, indicating the extent of caries. 5 Several studies have examined the effectiveness of this method for the detection of occlusal caries lesions in vitro 15 –18 and in vivo. 19 –21
The LED-based device is a new method used for dental caries diagnosis. It is a portable, handheld LED-based device that uses the combination of LED and fiberoptic technology, designed to aid in the detection of caries in occlusal pits and fissures and the interproximal areas of adult posterior teeth. 14
With regard to the performance of new methods to identify carious lesions, it is difficult to generalize findings, especially from in vitro studies, and more clinical studies are needed to inform clinicians about the usefulness of new caries detection devices such as LED-based devices. Although a few in vitro studies 22 –24 related to LED-based devices have been reported in the literature, to our knowledge there is no in vivo study that has been published to date investigating the effectiveness of LED-based devices for occlusal caries detection. Therefore, the aim of this clinical study was to assess the performance of LED-based devices and compare the in vivo validity of VI with that of LF- and LED-based devices in diagnosing occlusal caries in permanent molars.
Materials and Methods
A total of 156 occlusal surfaces were investigated from 37 patients (30 females and 7 males) 20–25 years of age, with a mean age of 20.2±1.51. The aim, procedures, and benefits of this clinical study were explained to the participants, and informed consent was obtained before the study. The volunteer participants were recruited from Department of Restorative Dentistry. Inclusion criteria for the participants were presence of a minimum of one permanent molar with at least one occlusal sound or macroscopically uncavitated caries site. Exclusion criteria included patients who were uncooperative, those with disabilities or severe systemic diseases, and those with language difficulties. The study was approved by the local ethics committee. The teeth were the first and second permanent molars that were macroscopically intact but with inconspicuous caries. The occlusal surfaces were thoroughly cleaned with a rubber cup and non-fluorescent polishing paste. The patients with teeth showing frank cavitation, obvious signs of enamel hypomineralization, or hypoplasia in the occlusal surface and that had fillings, fissure sealant, restorations, or an orthodontic band were excluded from the study.
Examination methods
All the examinations were conducted by two experienced examiners who had been trained in caries assessment in a pilot examination conducted before the study. Teeth were kept humid and were air dried for 3 sec before VI. VI was performed with the aid of a light reflector, air/water spray, and a dental mirror, using the criteria shown in Table 1. Caries lesions on the selected sites of the occlusal surfaces were examined using the LF- (DIAGNOdent devices, Kavo, Dental, Biberachl Riss, Germany) and LED-based (The Midwest Caries I.D. Dentsply Professional Division, York, PA) caries detectors.
Visual examination scores were adopted from Ekstrand's visual scoring system (V1 and V2 were combined), D0-3: LF-based devices readings; C0-3: LED-based devices readings; V0-4: visual inspection readings.
LED, light-emitting diode; LF, laser fluorescence.
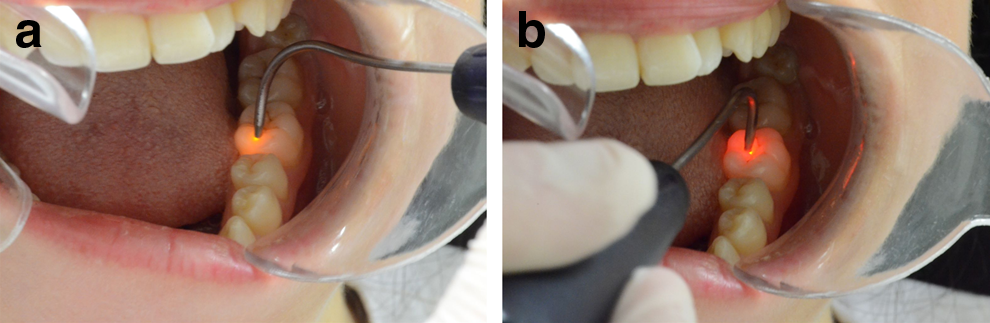
A cone-shaped tip designed for fissure caries was used on the LF-based pen device, and after the VI, the device was calibrated against the ceramic standard according to the manufacturer's instructions. The tip of the LF-based device was placed perpendicular to the long axis of the tooth, and slightly tilted circular movements were performed along the complete occlusal fissure as recommended by the manufacturer. The maximum LF-based device reading (0–99) obtained from the whole fissure pattern was recorded. The presence or absence of occlusal caries was determined using the manufacturer's suggested cutoff points (Table 1). 17 The LED-based device was used to take measurements after calibration with the ceramic standard. For occlusal caries, wet pits and fissures were probed in direct contact parallel to the long axis of the tooth. The presence of demineralization activates a change in the LED-based device from green to red, with a concurrent audible signal confirming the presence of caries (Fig. 1). The performance was assessed according to the cutoff limits suggested by the manufacturer (Table 1).
Participants who had a tooth with any occlusal molar surface yielding a visual score of V1, V2, V3, or V4 or an LF-based device score ≥20 (Table 1) were invited to return within 2 weeks for pit and fissure opening, followed by appropriate preventive or restorative treatment. 5,25 Pits and fissures of the included molars were carefully opened with a diamond fissure bur, and the extent of the lesions was assessed by a specialist in operative dentistry with 5 years of clinical experience, in accordance with the four point scale in Table 1. After all caries were removed using a minimally invasive technique, the cavities were subsequently sealed with an appropriate restorative material. 19 VI after pit and fissure opening with a carbide bur was used as the reference standard in this study.
Statistical analysis
The inter-examiner reliability of the caries detector examinations was assessed using the weighted κ statistics. The sensitivity, specificity, and accuracy in diagnosing occlusal caries using the two devices were calculated according to appropriate cutoff scores. The area under the receiver operating characteristic (ROC) curve was measured for both devices to compare their diagnostic performance for occlusal caries diagnosis at threshold 1 (considering the criterion standard scores 1, 2, 3, and 4 for VI and 1, 2, and 3 for other methods, as evidence of disease) and threshold 2 (considering the criterion standard scores 3, 4 for VI and 2, 3 for other methods, as evidence of disease). In order to determine whether the diagnostic performances of dental caries detection methods were statistically significant from one another, a one way analysis of variance (ANOVA) followed by unequal N honest significant difference (HSD) post-hoc comparisons was performed (Table 2). Analyses were performed using the SPSS version 13 statistics program for Windows.
The mean difference is significant at the 0.05 level.
LED, light-emitting diode; LF, laser fluorescence.
Results
In this study, 56 maxillary molars, 6 maxillary premolars, 86 mandibular molars, and 8 mandibular premolars, totaling 156 teeth, were evaluated and treated. Substantial inter-examiner agreement was found for the LF- and LED-based device readings in the present study (κ=0.76 and κ=0.61, respectively). The κ coefficient of the inter-examiner agreement for the VI was perfect (κ=0.87).
A one-way ANOVA followed by unequal N HSD post-hoc comparisons revealed a better performance of the LF device (p<0.05) compared with visual inspection and the LED- based device (Table 2). Table 3 is a cross-table showing the distribution and number of teeth according to diagnostic methods and fissure opening scores. Upon VI, 30 (19.9%) of the molars were status V0, 43 (26.9%) were V1, 71 (45.5%) were V2, 9 (5.8%) were V3, and 3 (1.9%) were V4. Pit and fissure opening was performed on 126 teeth.
O 1, Observer 1; O 2, Observer 2; D 0-3, LF-based devices readings; C 0-3, LED-based devices readings; V 0-4, visual inspection readings.
LED, light-emitting diode; LF, laser fluorescence.
Higher specificity values were achieved at a T2 threshold using the LF-based device (0.76 and 0.80) and at a T1 threshold for the LED-based readings (0.60 and 0.62) and VI (0.90 and 0.93) for both observers. With regard to VI, higher sensitivity values were found at both thresholds for the two observers when comparing the three caries detection methods (0.98 at T1 and 0.96 at T2). Accuracy values at T1 were higher than those at T2 for all the three caries detection methods (Table 4).
T1, threshold 1; T2, threshold 2.
LED, light-emitting diode; LF, laser fluorescence.
At the T1 diagnostic threshold, the areas under the ROC curve were 0.90–0.91 for the LF-based device, 0.73–0.79 for the LED-based device, and 0.92–0.95 for VI. At the T2 diagnostic threshold, the areas under the ROC curve were 0.82–0.85 for the LF-based device, 0.68–0.70 for the LED-based device, and 0.55–0.56 for VI. The area under the ROC curves showed that VI was better than the LF and LED-based devices at the T1 diagnostic threshold. However, the LF-based device was better than both VI and the LED-based device at the T2 diagnostic threshold. The areas under the ROC curves (u) for all the diagnostic methods used in the study are shown in Table 4.
Discussion
There have been several studies related to the performance of the LF-based device in the literature. 5,12,19,22,23,26,27 Few of them were in vivo. 5,19,26,27 The newly developed LED-based caries detection device was recently introduced to clinicians. However, only a few in vitro studies relating to the detection ability of this device were found in the literature. 22 –24 To our knowledge, there has been no study to date evaluating the in vivo performance of the LED-based device in the detection of occlusal caries. For that reason, the present in vivo investigation aimed to evaluate the validity of the LED-based device for detecting initial occlusal caries lesions by comparing values derived from it with those derived from the LF-based device and VI.
The international trend in caries management is to move away from the invasive toward a preventive approach aiming to control the initiation and progression of the disease process over a person's lifetime. Therefore, a major challenge for the clinician is to detect lesions at an early stage. Occlusal surfaces are known to be the area most susceptible to caries because of the morphological structures of pits and fissures. However, in particular, the early diagnosis of occlusal caries is difficult when using conventional methods to detect such lesions, as there may be dentine caries beneath seemingly intact surfaces. To overcome the difficulty, the use of new instrumentation or noninvasive techniques may improve reliability and aid in the detection of early de-mineralization on or beneath the enamel surface, which may not be apparent clinically. 14
VI was chosen in the present study because it has more validity than tactile examination with regard to caries diagnosis. 28 Furthermore, probing pressure can cause irreversible damage to the demineralized tooth structure and increase the risk of dental caries progression. Moreover, this technique can lead to the spread of caries in the same oral cavity because of the possibility of transferring cariogenic microorganisms from one site to another. 5
In the present study, fissure opening was used as the gold standard to evaluate accuracy of the different diagnostic methods. The criteria used for fissure opening to decide preventive or restorative treatment was varied in the past studies. 5,18,19 Whereas the criteria were determined according to a VI or a radiographic evaluation in conjunction with a DIAGNOdent score (≥20) in one study, 5 VI or radiographic evaluation regardless of DIAGNOdent scores was used as a criterion in other studies. 18,19,21,29 LF-based device performance is dependent upon the cutoff limits applied. Different cutoff limits are used by the manufacturer and by in vitro and in vivo studies, and there is great variation with regard to the cutoff limits adopted. This is confusing for clinicians when deciding restorative treatment in the clinic. Moreover, because it has been reported that the values determined in in vitro investigations were lower in in vivo studies, resulting in an obstacle to obtaining accurate results in the clinic. 18,19,28 Therefore, in this study, it was decided to use fissure opening on the basis of VI or LF device scores.
The κ values calculated for DIAGNOdent in in vivo studies varied from 0.53 to 0.95, and those for VI varied from 0.66 to 0.95. 5,20,21,29 However, VI yielded higher κ values than did the LF-based device in these studies, similar to the present study (κ=0.76 for DIAGNOdent and κ=0.87 for VI). As a new caries detection device, the authors found κ values of the LED-based device to be 0.89 and 0.85. 22,23 In the present in vivo study, the κ value for the LED-based device was found to be 0.61. The differences may result from subjective factors, such as knowledge and clinical experience and in vitro conditions not similar to in vivo conditions. However, the reproducibility of a test may be very good, but it may not always give accurate results for early caries diagnosis.
A good caries diagnostic method should be both highly sensitive and specific; its values should be at least 0.75 for sensitivity and >0.85 for specificity. 30 In previous in vivo studies, the sensitivity of VI ranged from 0.25 to 1.00, and the specificity ranged from 0.75 to 1.00. 5,10,19 –21,29 In the current study, the sensitivity and specificity values were found to be similar to those of previous in vivo studies. 5,10,19 –21,29 VI has been shown to have high specificity but low sensitivity in occlusal caries detection in some studies. 5,10,16,18,20,21 In the present study, the specificity and sensitivity values calculated as 0.90 and 0.98, respectively. However, the specificity value determined according to the threshold used to identify dentine caries was moderate (0.48). The decrease in specificity value may result from differences between cutoff values in thresholds 1 and 2.
The LF-based device for occlusal caries detection has shown moderate to high sensitivity and lower specificity in the present study, similar to those in previous in vivo studies. 5,18,21 However, higher specificity values were reported in some studies 18,19,27 because of different cutoff values used for the LF-based device. Some studies 16,30 have reported that the LF-based device was not reliable for the detection of initial caries lesions, but was more effective in determining caries lesions in dentine. 10,19,21,31 In this study, specificity values at the T2 threshold (0.75–0.80) were higher than those at the T1 threshold (0.60–0.57). These results were in accordance with previous studies. 19,21 Recently, in vivo studies 5,10,18,21 have reported that the LF-based device has greater sensitivity but lower specificity than VI. Contrary to these studies, in the present study, sensitivity and specificity were higher for VI than for the LF-based device, with the exception of the specificity calculated for dentine lesions. The reason for this may be the different cutoff values and thresholds used.
In in vitro studies related to the LED-based device, 22,23 the specificity values of the LED-based device ranged from 0.48 to 0.90 and the sensitivity values ranged from 0.31 to 0.84. In the present in vivo study, the specificity values of the LED-based device ranged from 0.55 to 0.62 and the sensitivity values ranged from 0.80 to 0.88, which were similar to those in in vitro studies. 22,23
The specificity of the LED-based device was lower than that of VI but higher than that of the LF device at threshold 1, and lower than the LF-based device but higher than VI at threshold 2. According to the results of the current study, the LED-based device was more effective at accurately identifying sound surfaces than the LF-based device. The sensitivity of the LED-based device was lower than that of VI and the LF-based device at threshold 1 and lower than that of VI but higher than that of the LF-based device at threshold 2, similar to the results reported by Aktan et al. 22 Therefore, the LED-based device may be more useful to rule out caries at the dentinal level than the LF device.
In this study, accuracy at threshold 1 was the highest for VI (0.96), followed by the LF- (0.85) and LED-based devices (0.83). Therefore, the performance of VI in accurately detecting clinically sound and carious surfaces was better than the performance of the other methods. However, because accuracy at threshold 2 was the lowest for VI (0.51), followed by the LED- (0.62) and LF-based devices (0.75), VI has a lower ability to detect caries on dentine than the other methods.
Conclusions
VI yielded more accurate results than the LF- and LED-based devices, when teeth were free of occlusal caries. The LED-based device was able to detect dentine caries more accurately than the LF-based device. The ability of the LF-based device to accurately identify sound surfaces was better than that of the LED-based device. The proportion of correct responses of the LF-based device according to the fissure opening scores was greater than for the other methods. Therefore, both the LF- and LED-based devices may be used as a valuable adjunct to VI.
Footnotes
Author Disclosure Statement
No competing financial interests exist.