
Abstract
Introduction
Interest in the treatment of DH has increased because of increasing numbers of hypersensitivity patients. Two treatment principles are used to address DH. First, open dentinal tubules should be occluded mechanically so as to decrease tubular fluid flow in dentin, and second, the pain should be controlled chemically by desensitizing sensory nerves in the pulp. 3 Based on these principles, desensitizing dentifrices are most commonly used. In a previous study, 8 dentifrice containing 20% nano-carbonate apatite (n-CAP) was found to be most effective at occluding dentinal tubules. Carbonate apatite is chemically similar to the mineral compositions of teeth and bones, 8,9 and n-CAP has an extremely small particle size, which increases its surface area and promotes its absorption onto tooth surfaces.
However, to treat DH successfully, a long-lasting occluding effect is required, in addition to blocking exposed dentinal tubules, and, therefore, treatment ingredients must be resistant to the acid and mechanical challenges presented by the oral environment. 10 Furthermore, the primary mechanism of desensitizing dentifrices, various fluoride products, and of resins applied to dentin is one of mechanical occlusion rather than fusion with dentinal tubules, 3,11,12 and, therefore, treatments must be applied repeatedly. 10,13
Recently, various types of laser therapy have been used to treat DH. 3 The lasers used for the treatment of DH are divided into two groups: low output power (low level) lasers (i.e., diode lasers or He-Ne lasers) and middle output power lasers (Nd:YAG, CO2, and Er:YAG). Although the mechanism of low level laser has been mostly unknown, it is postulated that this type of laser mediates an analgesic effect related to depressed nerve transmission. The mechanism of middle output power lasers has been known; the beam melts and re-crystallizes the dentinal tubules, which leads to occlusion or narrowing of dentinal tubules. CO2 laser is a middle output power laser. 14,15 Also, in previous studies, 13,16,17 irradiation from CO2 laser was found to increase resistance to physical and chemical challenges by changing the structure of dentin. Furthermore, a number of experiments have been conducted with the aim of relieving the symptoms of DH using a various lasers, including CO2, Nd:YAG, and Er:YAG, in combination with desensitizing products, 11 –13, 18 –22 and these experiments showed that this type of combination treatment can reduce pain symptoms more so than either treatment used alone. According to Ipci et al., 11 CO2 laser or Er:YAG laser combined with NaF gel provide better results than NaF gel alone. Furthermore, the use of a CO2 laser and chemical inhibitors has been reported to act synergistically to provide almost complete acid resistance. 23
For desensitization purposes, it is important to choose a laser that will melt n-CAP. Recently, Nd:YAG, Er:YAG, and CO2 lasers have been widely used to treat DH. 3,24 However, Nd:YAG lasers have thermal side effects, because they penetrate deep through dentin, 3,20 and Er:YAG lasers remove dentin and cementum mechanically, which increases surface porosity. 25 Furthermore, the results of one study suggested that Er:YAG laser irradiation removes the n-CAP layer on the dentin surface because of microexplosions involving OH- in hydroxyapatite. 26 On the other hand, CO2 lasers do not thermally damage the tooth surface or pulp, and because the emitted radiation is absorbed efficiently by water and hydroxyapatite, it does not penetrate pulp. 17,24,27 For the reasons mentioned, we decided to use the n-CAP plus CO2 laser combination in the present study. The aim of this in vitro study was to evaluate the tubule occluding effects of dentifrice containing 20% n-CAP plus CO2 laser treatment, and to assess the acid resistance of occluded tubules.
Materials and Methods
Sample preparation
For this study, 120 specimens of extracted human molars (free of lesions) were used. Crowns were removed up to the cemento–enamel junction using a diamond wheel disc (NTI-Kahla, Kahla, Germany) and a low speed handpiece (Lasungmedice, Incheon, Korea). Root samples were first embedded in a Teflon mold using an acrylic resin (Ortho-jet, Lang Dental Mfg. Co., Inc., USA). The root surface was then ground with silicon carbide paper (Allied High Tech Products, Rancho Dominguez, USA) using a polishing machine (RB 209 Minipol, R&B Inc, Korea) to expose the dentin surface. Four specimens (2×2 mm2) were obtained from each embedded root dentin sample. These specimens were then embedded in an acrylic mold with putty (Examfine Putty type, GC Dental Products Corp., Japan), etched with 6% citric acid for 90 sec to completely open dentinal tubules, and rinsed. 8,28
Classification and treatment of control and experimental groups
One hundred and twenty specimens with exposed dentinal tubules were divided into four groups (the control, n-CAP, laser, and combined groups). Thirty specimens in each group were reassigned to three different conditions: baseline, treatment for occluding dentinal tubules, and acid challenge (Table 1). The treatments were: the application of n-CAP, CO2 laser irradiation, and n-CAP, followed by CO2 laser irradiation. Control group specimens were not treated after opening dentinal tubules with citric acid. Specimens in the n-CAP group were treated with 20% n-CAP dentifrice (Dentiguard sensitive®, Daewoong, Korea) slurry using 50 linear strokes at a force of 150g using a V-8 Cross Brushing Machine (Sabri Enterprises, Downers Grove, IL, USA) and then rinsed with distilled water. Specimens in the laser group were irradiated with a CO2 laser (Panalas CO5∑, Panasonic, Japan) with a 1A tip for 1 min. The laser beam was swept in a zigzag manner with the beam directed vertically to the dentin surface. The irradiation conditions used were: a wavelength of 10.6 μm at a power output of 3 W with a low air cooling setting. Energy density was 0.96 J/cm2 with ∑mode. The combined group was first treated with 20% n-CAP and then irradiated.
Thirty specimens in each group. Ten specimens from each group were reassigned to the baseline, treatments, and the acid challenge.
After treatments, 10 specimens from the four groups were subjected to an acid challenge by immersion in pH 4.0 acetate buffer solution (0.1 M sodium acetate+0.1 M acetic acid) for 3 min without agitation, and then rinsed.
Scanning electron microscopy (SEM) examination and image analysis
All specimen surfaces were evaluated after opening dentinal tubules, treatments, and acid challenge using an SEM (S-4700 Hitachi Ltd., Tokyo, Japan) to identify morphological changes (×3000). Three micrographs were randomly taken of each specimen. Degrees of dentinal tubule occlusion were quantified using an image analyzer (Image-Pro PLUS 6.0, Media Cybernetics, USA). Image analysis was used to measure numbers of open dentinal tubules on SEM micrographs of specimen surfaces. The software polygon tool was used to draw the outline of dentinal tubules based on gray pixel intensity differences between dentinal tubules and the outer area, and then total mean open areas were calculated. 8 Specimens were placed on their longitudinally sectioned surfaces to obtain the thicknesses of deposition layers (×5000).
Statistical analysis
One-way ANOVA and Tukey's post-hoc test (PASW statistics ver. 18.0, SPSS, Chicago, IL, USA) were used to evaluate intergroup differences, and the paired t test was used to determine the effects of treatment on tubule occlusion and of the acid challenge. p Values of<0.05 were deemed statistically significant.
Results
Effects of treatments on dentinal tubule occlusion
According to before and after treatment results, the area of open dentinal tubules decreased significantly after treatment in all three experimental groups (p<0.0001, Fig. 1). After treatment, all experimental groups exhibited a significant decrease in tubule area as compared with the control group (p<0.0001, Table 2). However, the occluding effects of different treatments were not significantly different. n-CAP group specimens had partially or completely plugged tubules and an n-CAP layer covering surfaces on cross-sectional micrographs (Fig. 2b). The laser group had occluded dentinal tubules because of the melting of dentin, and a thin dentin layer was observed on dentin surfaces to cover the tubules (Fig. 2c). Most tubules were occluded in the combined group and the n-CAP layer was observed to have partially melted (Fig. 2D). According to cross-sectional micrographs, the combined group had a thicker n-CAP layer than the n-CAP group, and re-crystallized particles were found to have penetrated into tubules (Fig. 2d).

Comparisons of dentinal tubule area at baseline, after treatment, and after acid challenge. Statistically significant differences between groups are indicated with asterisks (*p<0.05; paired t test).
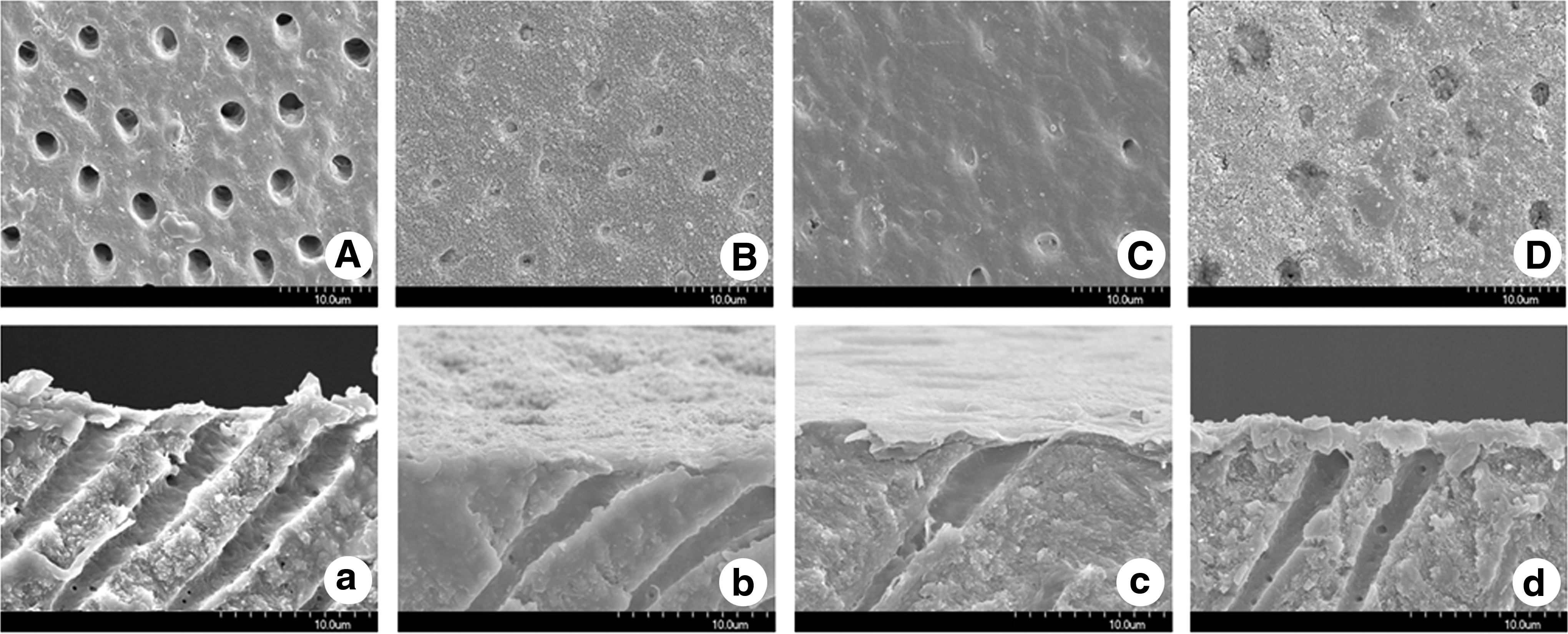
Scanning electron microscopic (SEM) micrographs of specimen surfaces (
All values denote the mean (standard deviation).
Unit: μm2
p-values were determined by one-way ANOVA (α=0.05).
In the same column, different superscript letters denote significant differences between groups by Tukey post-hoc (α=0.05).
Assessment of acid challenge
After specimens had been immersed in acetate buffer solution, significant increases in open tubule areas were observed in the three experimental groups (p<0.0001, the n-CAP and the laser group; p=0.003, the combined group, Fig. 1). However, the combined group had the fewest reopened dentinal tubules, and the laser group had the most (Table 2). In the n-CAP group, n-CAP particles were observed on dentin surfaces, but dentinal tubules were open (Fig. 3B). In the laser group, the melted dentin layer covering dentinal tubules was absent (Fig. 3C). However, in the combined group, in addition to fewer open tubules, tubules were narrower because of remaining n-CAP on inner tubule walls (Fig. 3D). Furthermore, the n-CAP layer formed during the combined treatment remained after acid challenge.
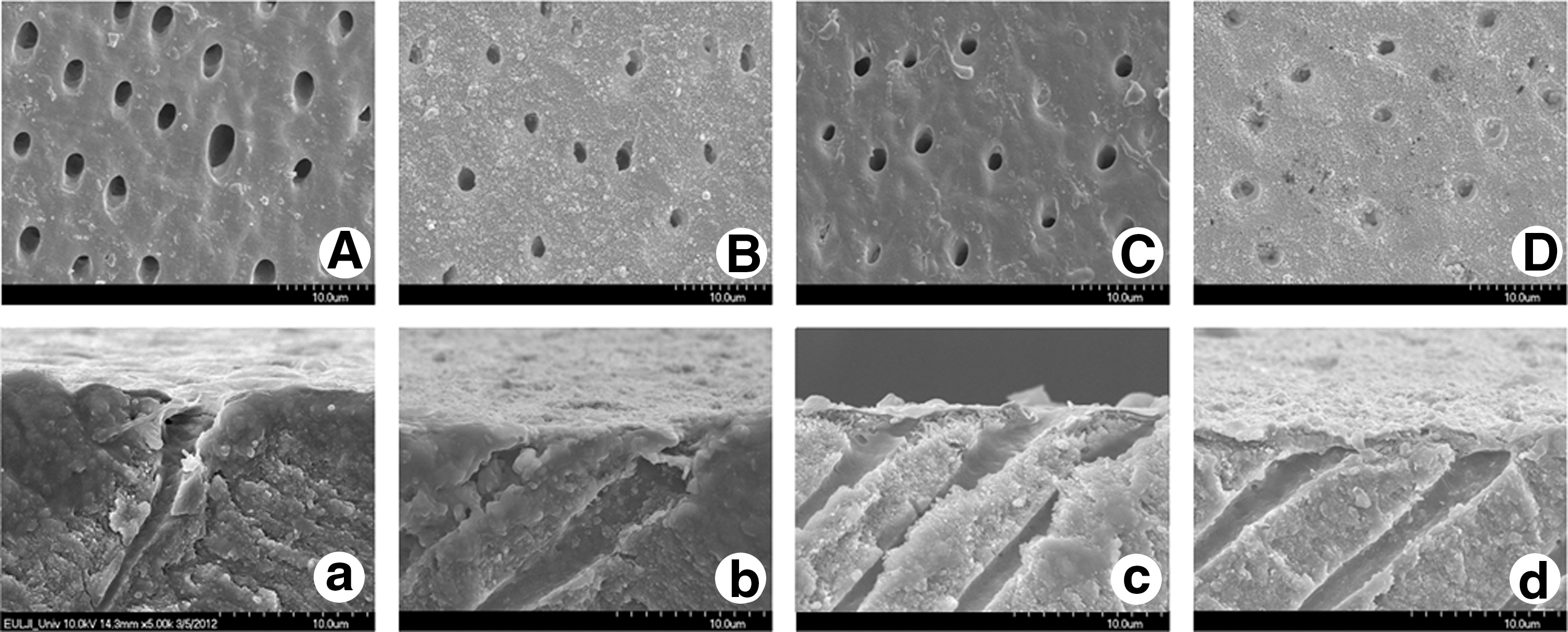
Scanning electron microscopic (SEM) micrographs of specimen surfaces (
Discussion
Various desensitizing products have been developed for the treatment of DH, and much research is being conducted on their effectiveness. Currently, a dentifrice is widely used to treat DH at home. Lee et al. 8 evaluated the tubule occluding effects of dentifrices containing various concentrations of n-CAP, and found that a dentifrice containing 20% n-CAP produced the highest occlusion rate and was more effective at tubule occlusion than one containing SrCl2. Hence, a dentifrice containing 20% n-CAP was used in the present study, and the tubule occlusion rate achieved was 89% (p<0.0001), which is similar to the result previously obtained. 8
The acid used in this study is pH 4.0 acetic buffer solution and it was used for 3min. Kameyama et al. 29 reports having used pH 4.0–4.5 of lactic or acetic buffer solution to investigate the acid resistance of a tooth, and reported it to be useful. One previous study used acid for acid challenge limited to 3 min without agitation. The acid challenge was chosen to be at the severe end of the spectrum, so that it could be determined whether occlusion was maintained in a severe erosive regime. 30
On SEM micrographs, the n-CAP group had occluded dentinal tubules with n-CAP particles (Fig. 2B). However, the n-CAP layer was easily removed by the acetate buffer solution used in the acid challenge. According to a previous study that evaluated the effects of various dentifrices in terms of their abrasion and antierosion characteristics, a dentifrice containing zinc-carbonate-hydroxyapatite exhibited the greatest enamel loss when specimens were immersed in acidic solution or were immersed with additional brushing, presumably because zinc-carbonate-hydroxyapatite is easily dissolved by acid. 31 The acid-labile nature of the occlusion precipitations formed by an arginine-containing dentifrice (a currently marketed dentinal tubule occlusion dentifrice) has been supported by a number of recent publications. 32 –34 In another study, Wang et al. 35 found that dentin permeability was significantly reduced to <40% when two desensitizing dentifrices were used. And attentuated total reflectance Fourier transform infrared spectroscopy (ATR-FTIR) analysis showed an increase in the intensity of the phosphate peak after treatment, and SEM images showed partially occluded dentinal tubules. However, dentin permeability significantly increased and the intensity of the phosphate peak decreased after acid challenge for the two dentifrices groups, and SEM showed that tubules had reopened after acid exposure.
The primary mechanism of these dentifrices depends upon mechanical occlusion (without adhesion) by the precipitation of insoluble calcium fluoride crystals within tubules. Thus, precipitates cannot resist the challenges posed by the oral environment. 11,12,36 Therefore, dentifrices that rely on mechanical occlusion must be applied repeatedly. The application of various lasers is emerging as a new means of sealing dentinal tubules to achieve a long-term effect. Lasers exert their desensitization effects by occluding dentinal tubules and/or reducing dentinal nerve function via ion interactions. 3,14 Because it has a lower penetrating depth than the Nd:YAG laser, the CO2 laser reduced the risk of pulp damage. 3,20 Also, the CO2 laser can melt and cause dentin re-crystallization because of absorption by hydroxyapatite. 3 According to the results of the present study, the CO2 laser had an occlusion effect of 77% as compared with baseline (p<0.0001). Tubular occlusion achieved using the CO2 laser was the result of shiny, smooth, melted peritubular dentin (Fig. 2C). Nevertheless, the open tubule area was significantly increased by acid exposure (p<0.0001), presumably because the protective layer formed by melting dentin was thin and did not penetrate tubules. Loss of calcium and phosphate ions from enamel was observed in almost all test groups that were exposed in hydrochloric acid after being irradiated by different CO2 laser parameters with varying fluences from 0.1 to 0.9 J/cm2, pulse durations from 80 to 400 μs, and repetition rates from 180 to 700 Hz. 37
One of the side effects of lasers is that they can damage pulp and hard tissue because of the accumulation of heat. Therefore, many studies have been performed to optimize laser irradiation parameters for the treatment of DH. In most studies, a continuous wave mode that operates at constant energy and a pulsed mode that releases high power pulses at regular intervals are used. The pulsed mode has been used in many previous studies, 3,17,27,38 because it tends to cause less thermal damage. The manufacturer recommends using ∑ mode to treat DH. The ∑ mode of this laser is the same as the power of pulsed mode of CO2 laser, except that its total thermal energy is 25% of the pulsed mode. In the present study, tubule occlusion was greatest in the combined group (p<0.0001, Fig. 1). SEM micrographs showed that the n-CAP layer had been fused (Fig. 2D), and some re-crystallized particles were observed in tubules. n-CAP can bond chemically to the surface of enamel because of its similar composition, but because it is amorphous, it dissolves in the oral cavity. 39 Therefore, the laser irradiation of the n-CAP layer results in a more resistant protective layer by promoting the re-crystallization of n-CAP particles, and, in particular, significantly increases acid resistance by eliminating carbonate. 19 Recently, several studies have reported a new therapy that combines calcium compounds or fluoride and laser treatment. Romano et al. 18 reported that calcium hydroxide paste achieved significantly higher tubule occlusion scores than CO2 laser irradiation only. Furthermore, in vivo, CO2 laser plus stannous fluoride gel after 3 months showed that 94.5% of patients were free from sensitivity 13 and in the same cohort after 18 months, the success rate was 96.5%. 21 In the present study, after acid challenge, fewer tubules reopened in the combined group than in the CO2 laser or n-CAP group. We surmise that the n-CAP was melted by the laser and then combined with the dentin. Esteves-Oliveira et al. 19 concluded that the irradiation of enamel with a CO2 laser in combination with amine fluoride gel significantly decreased the abrasion of softened enamel by tooth brushing. In another study, 20 combined therapy (CO2 laser+fluoride) could effectively reduce enamel surface loss during citric acid exposure. Fluoride in sites irradiated by a CO2 laser could transmute hydroxyapatite into fluorapatite by enhancing fluoride uptake by teeth.
Conclusions
To summarize, all experimental groups (the n-CAP, the CO2 laser, and the combined group) showed higher dentinal tubule occlusion rates than that of the control group. Excellent occlusion was achieved in combined group, and this effect was maintained after the acid challenge. The combined therapy using a dentifrice containing n-CAP and a CO2 laser was found to provide greater relief for DH than either treatment method alone. Our findings indicate that CO2 laser treatment to the n-CAP layer should reduce patient discomfort and result in less dentin damage. However, this study is limited by its in vitro nature, and, therefore, further study is needed using an in situ model to assess the clinical situation.
The application of both 20% n-CAP and CO2 laser irradiation was found to have a beneficial desensitizing effect on exposed dentin. However, these treatment methods had no benefit on acid resistance. On the other hand, combined n-CAP and CO2 laser treatment achieved better dentinal tubule occlusion and acid resistance. The present study shows that combined therapy (CO2 laser+20% n-CAP dentifrice) offers a promising means of treating DH in a clinic setting.
Footnotes
Acknowledgments
This research was supported by Basic Science Research Program through the National Research Foundation of Korea (NRF) funded by the Ministry of Education, Science and Technology (R13-2003-013-05002-0).
Author Disclosure Statement
No competing financial interests exist.