
Abstract
Introduction
The study and application in clinical practice of low-level laser irradiation (LLLI) has been occurring for two decades. It has been demonstrated that LLLI is not only safe, but also can modulate various biological processes. LLLI, for example, has the potential to accelerate collateral circulation; improve microcirculation; 7 facilitate wound healing; attenuate the inflammation reaction; and promote the proliferation of osteoblasts, lymphocytes, articular cartilage cells, and fibroblast cells. 8 –10 Over the years, Oron et al. found that LLLI could reduce formation of scar tissue and infarct size after MI in rats and dogs. 8,9 They also demonstrated that LLLL could remarkably upregulate vascular endothelial growth factor (VEGF) and inducible nitric oxide synthase (iNOS) expression in the infarcted rat heart, and enhance angiogenesis and cardioprotection. 11,12 Moreover, LLLI could stimulate proliferation, growth factors secretion, and myogenic differentiation of bone marrow-derived mesenchymal stem cells (BMSCs). 13 It is well known that oxygen free radicals (OFR) play a large role in myocardial injury, especially in myocardial hypoxia and ischemia-reperfusion injury. Unfortunately, to our knowledge, there are few studies so far on the effects of LLLI on the OFR in the infarcted rat myocardial tissues. Therefore, the purpose of this study was designed to assess the effects of LLLI on the OFR in the infarcted rat myocardial tissues and the VR following MI in the rat by low level 635 nm diode laser irradiation.
Materials and Methods
Animals
A total of 120 female Sprague–Dawley rats (Laboratory Animal Center of Henan Province, Henan, China), weighing 250–350 g, were divided into sham group (30 rats), control group (45 rats), and LLLI group (45 rats) at random. The study was performed in accordance with guidelines of the Measures for the Administration of Experimental Animals in Henan province, and the experiment protocol was approved by the local Ethics Committee for Animal Study in the Second Affiliated Hospital of Zhengzhou University.
Establishment of RMMI
RMMI was induced by ligation of the left anterior descending coronary artery (LAD). 14 Briefly, the rats were anesthetized with 10% chloral hydrate solution (0.3 mL/100 g body weight). After the tracheotomy, the tracheal incubation was performed with an 18 gauge vein tube and mechanical ventilation was used at 75 breaths/min, with a tidal volume of 3 mL/100 g (HX-100E type of MS4000 ventilator for small animals, Chengdu Taimeng technology Ltd). The thoractomy was performed by invasion parallel to the ribs of the intercostal muscles between the fourth and fifth ribs. The ribs were spread by two retractors to expose the heart. The pericardium around the heart apex was opened slightly and limitedly with two sharp forceps. The heart was then exteriorized by exerting some pressure on the two sides of the chest. The ligation of the LAD was performed at a site 2.0–3.0 mm below the anterior- inferior edge of the left atrium with 6-0 polypropylene thread, along a line connecting the middle of the left auricular appendage and the pulmonary trunk with the apex of the heart. Before the LAD occluded, 0.05 mL 20% lidocaine carbonate injection was dropped in the surface of the heart to avoid arrhythmia. The chest was closed when the infarct heart beat regularly. The rat was subjected to extubation after spontaneous respiration, and allowed to recover in a special warm chamber at 30°C until fully awake. Benzylpenicillin with 10×1 03 U was injected into the thigh muscles at 1 day before the operation and for 3 days postoperation continuously. Food and water were supplied ad libitum. The rats in the sham group underwent the same procedure described without ligation of the suture.
Laser irradiation
Three weeks after establishment of RMMI, the thoracotomy was performed again to expose the heart by invasion of the intercostal muscles between the fifth and sixth ribs. A diode (GaAs) laser, with 600 quartz optical fiber, continuous wavelength of 635 nm, and an adjustable power output from 0 to 20 mW, was used in this study (Model KDL-300, Beijing KeDian Microwave Electronics Co. Beijing, China). The output power was set at 6 mW continuously with uninterrupted wave mode. The optical fiber tip, in all experiments, was placed 15 mm above the surface of heart to allow a laser beam diameter of 10 mm. The power density on the myocardium was 7.64 mW/cm2. Thus, the laser beam could spread over most of lateral wall of the left ventricle including the infarct myocardial area. The irradiation lasted for 125 sec constantly. The energy density to the myocardium appeared to be 0.96 J/cm2. The rats in the sham and control groups underwent the same process as that described for the laser irradiated rats, but the laser power was not switched on. The rats with MI were chosen at random for the laser irradiation and no irradiation groups. After laser irradiation, the chest was closed, and the rats were taken through the same procedure as after the RMMI establishment.
Measurement of the superoxide dismutase (SOD) activity and malondialdehyde (MDA) content
At 1, 24, 48, and 72 h and 1 week after laser irradiation, the hearts of the four to six rats in each group were harvested. The hearts were excised and immediately rinsed and cleaned with 4°C saline solution. The condition of the MI was checked in the control and LLLI rats. Rats without MI were omitted from the study. The free wall of the left ventricle, especially part of the myocardial necrosis, was excised and deposited in −80°C deep freeze laboratory refrigerator. Then, in the infarcted myocardial tissue homogenate, the activity of SOD was detected with the xanthine oxidase method, and the content of MDA was detected with the thiobarbituric acid (TBA) method following the instruction of SOD and MDA kits.
Histological analysis and Masson's staining
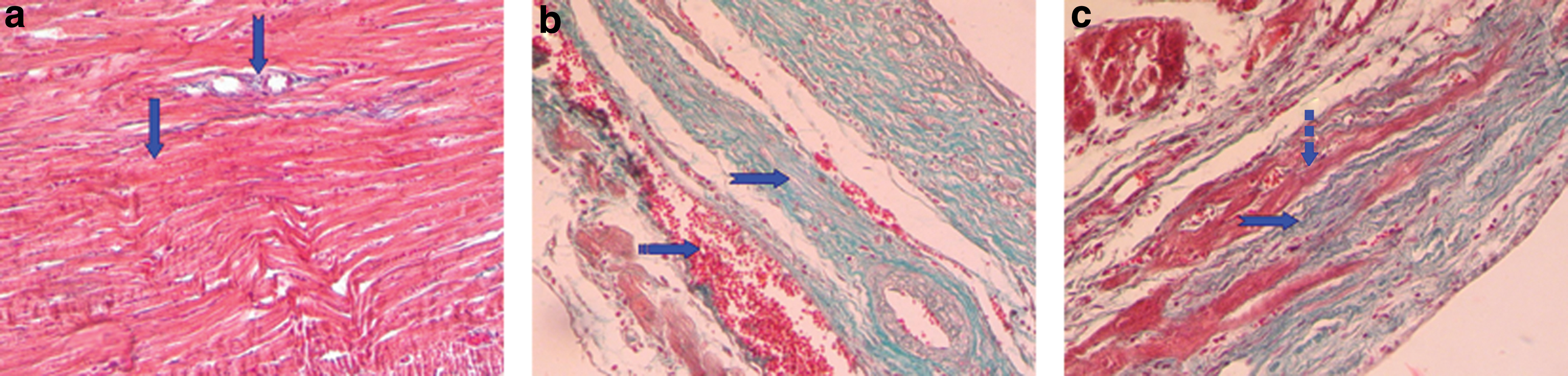
The hearts were excised at 1 week after the second operation, immediately soaked in the cold saline to remove blood caused by the heart beating, and rinsed clean of the residual blood in the chamber. Then, the hearts were fixed in 10% neutral buffered formalin for at least 48 h, dehydrated in different concentrations of alcohol, and embedded in paraffin. Sections 8 μm thick were prepared in a plane parallel to the atrioventricular groove and in the middle of the infarcted area. The serial sections were stained with hematoxylin and eosin (H&E) to observe the morphological changes and determine the infarct size and the left ventricular anterior wall thickness (Fig, 1) and with Masson's trichrome to delineate fibrous tissue from viable myocardial tissue and determine the percentage of fibrous tissue in the left ventricular anterior wall (Fig. 2). The infarct size was described as the percentage of infarct wall length from the circumferential length of the left ventricular wall. The left ventricular wall thickness was calculated by measuring the endocardial and epicardial length of the infarcted area. The percentage of fibrous tissue in the left ventricular anterior wall was determined in a different visual field of each histological section. Two observers who were blind to the experiment analyzed the histological slices.
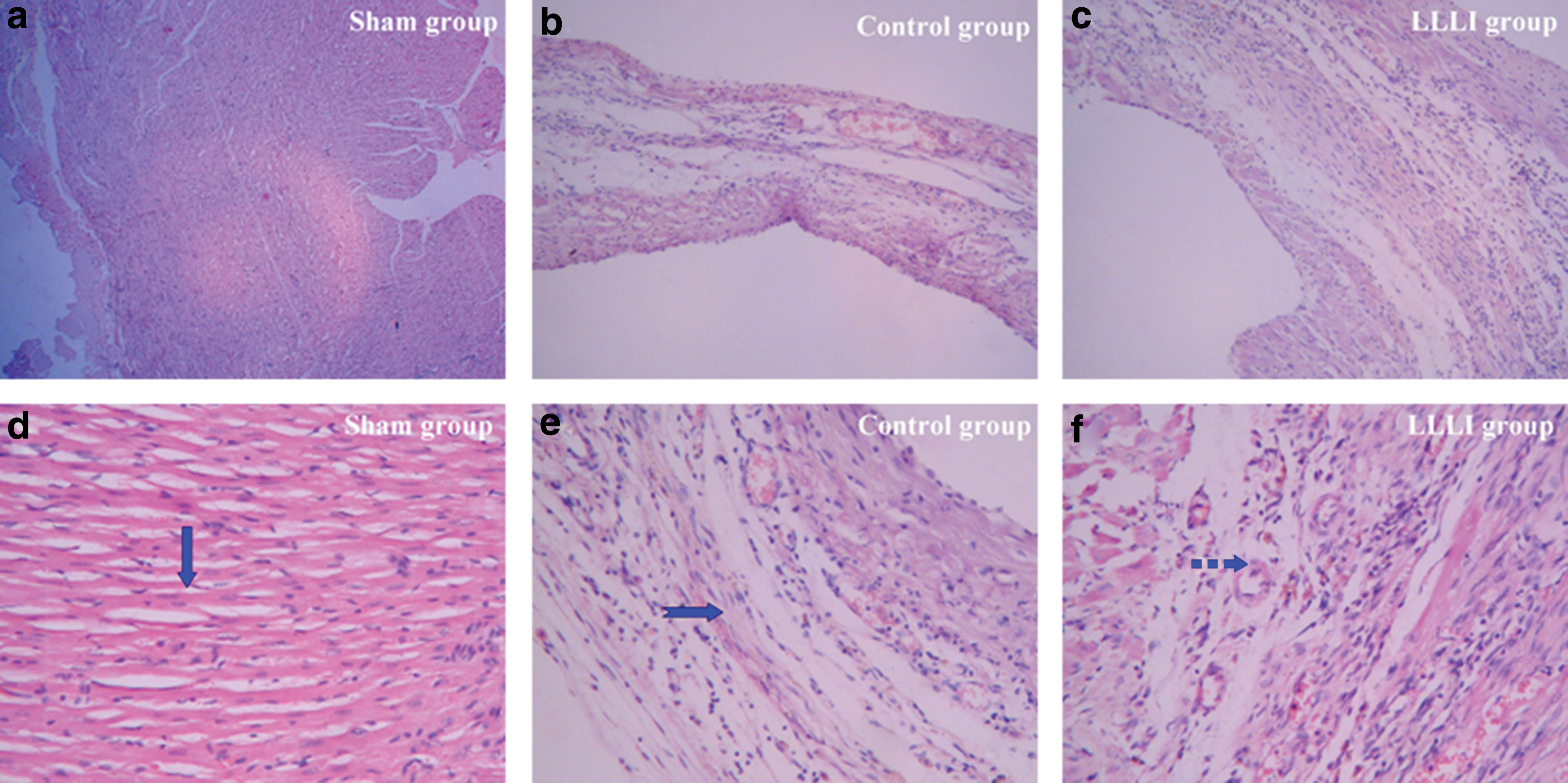
Representative light micrographs of hematoxylin and eosin (H&E)-stained cross-section of intact heart (
Typical light micro-photographs of intact normal rat heart
Statistical analysis
The data were collected and reported as means±SE. SPSS 17.0 software was used for statistical analysis. The group data comparison was made by one-way analysis of variances (ANOVA) and multiple comparisons with the least significant difference (LSD) test. A value of p<0.05 was considered statistically significant.
Results
Status of establishing MI model
The survival rate of RMMI was 77.8%. Unrecovered breathing, acute left ventricular failure, and fatal ventricular arrhythmia were the main causes of death. Three days after LAD ligation was the high-risk period. Ten rats could not breathe spontaneously, eight rats had acute left ventricular failure, and two rats died of fatal ventricular arrhythmia. As shown in Figs. 1 and 2, the normal cardiac cell disappeared and a large mass of collagen fibers formed in the infarcted myocardium. One third of the RMMI suffered left ventricular aneurysm (Fig 3). There was no significant difference in mortality between control and LLLI rats after laser irradiation.
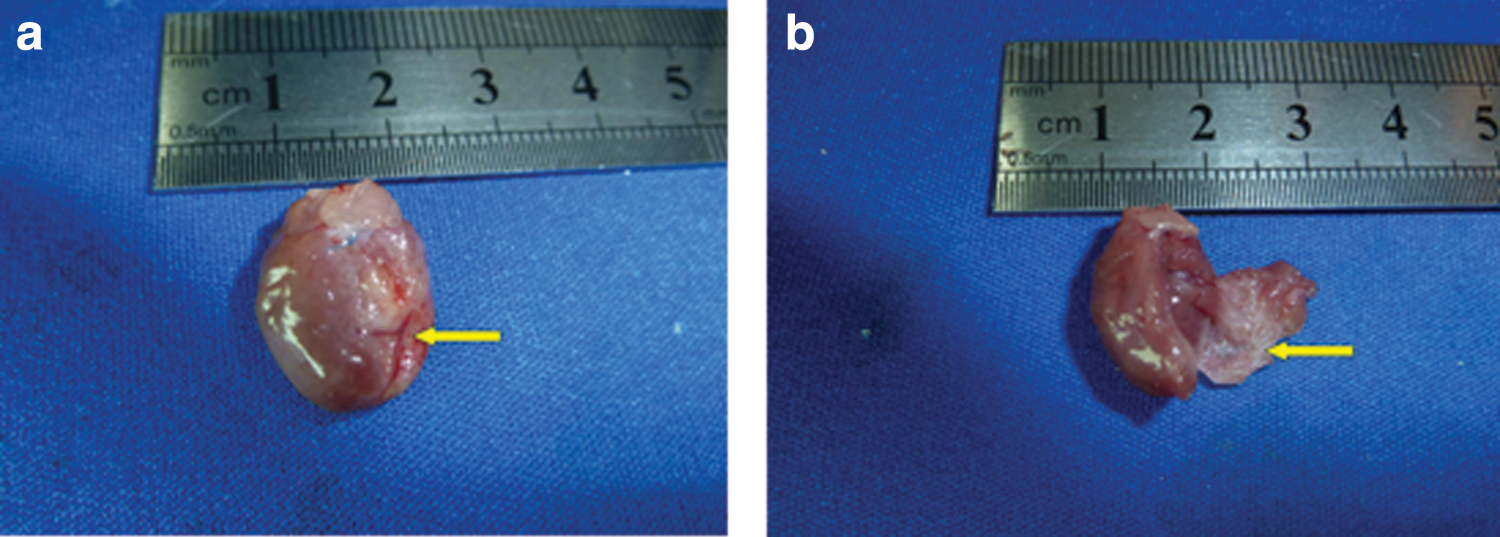
Gross appearance of the infarcted heart with left ventricular aneurysm marked with arrow in
Effects of LLLI on the SOD activity
As shown in Table 1, the activity of SOD in the infarct myocardium (control and LLLI group) decreased significantly at each time point compared with sham. SOD activity in the LLLI rats was lower than that in the controls until 1 week. It gradually increased from 1 to 48 h, peaked at 48 h after operation, and then decreased in all rats.
U/mgprot, n=4–6
p<0.05 vs. sham group; † p<0.05 vs. control group.
LLLI, low-level laser irradiation.
Effects of LLLI on the content of MDA
As shown in Table 2, the content of MDA in the sham rats was lower statistically than that in the rats with MI at different time points after the second operation. After laser irradiation, the MDA content increased significantly compared with in control rats. In contrast to the trend of SOD activity, MDA content decreased gradually from 1 to 48 h, bottomed out at 48 h, and then began to rise again in all rats.
nmol/mgprot, n=4–6.
p<0.05 vs. sham group; † p<0.05 vs. control group.
MDA, malondialdehyde; TBA, thiobarbituric acid; LLLI, low-level laser irradiation.
Assessment of the infarct size and left ventricular wall thickness
As shown in Fig. 1, infarct size decreased significantly in the LLLI group compared with the control group (18±9% vs. 35±10%, p<0.05). The left ventricular wall thickness in LLLI rats was 0.84±0.02 mm whereas in the control rats it was 0.31±0.03 mm (p<0.05), and the left ventricular wall thickness of the sham rats was 1.32±0.04 mm. The differences were all significant (p<0.05).
Evaluation of collagen fibers in the left ventricular wall
As shown in Fig. 4, the percentage of collagen fibers in the left ventricular wall in the sham rats was 4.81±0.40%. The percentage of the collagen fibers in the control (64.34±2.20%) and LLLI (30.97±2.60%) groups increased as compared with sham.
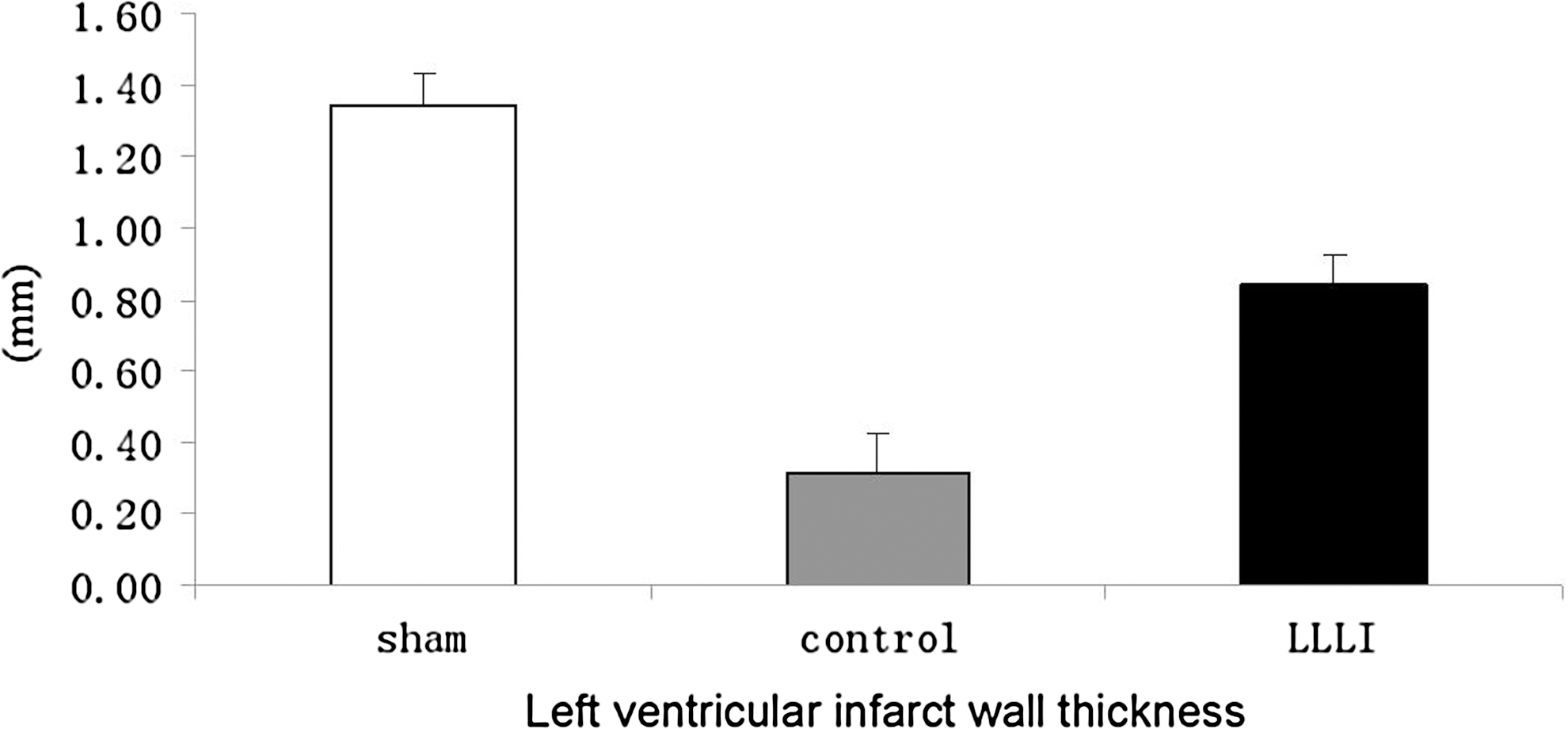
The assessment of left ventricular infarcted wall thickness.
Discussion
MI, hypoxia, and myocardial ischemia reperfusion injury behind MI can break the balance between production and elimination of OFR in the myocardium, and cause the excess accumulation of OFR that induce lipid peroxidation of unsaturated fatty acid in cell membrane to increase the content of MDA. Therefore, MDA content can directly reflect the degree of the lipid peroxidation. SOD, which plays large role in scavenging OFR, can protect the myocardium from cell injury induced by MDA. 3 The higher the activity of SOD, the greater the power of eliminating OFR. Therefore, the activity of SOD and MDA content can evaluate the level of the OFR.
The main findings of the present study are that LLLI can regulate the accumulation of OFR. Laser irradiation can decrease the activity of SOD and increased MDA content in the infarcted myocardium at the late stage of MI, and then reduce the infarct size and the left ventricular wall thickness and attenuate the formation of collagen fibers.
LLLI, which is a noninvasive physical treatment technique causing no significant harm, has a photochemical effect sometimes referred to as “photobiomodulation.” Unfortunately, the exact mechanism of the biological effects has not been fully understood. Karu et al. previously thought that cytochrome c oxidase (or cyt a/a3) and nicotinamide adenine dinucleotide (NADH)-dehydrogenases of the respiratory chain in eukaryotic cells, which mediate the transfer of electrons, were the photoacceptors. 15 The electron transport could lead to changes of the redox properties of the respiratory chain. In the process of mitochondrial electron transport, the superoxide radicals, such as O2 ·- and H2O2, are produced. Even a small increase in the concentration of O2 ·-and H2O2 can result in series of secondary responses, such as an increase in Ca2+, initiating lipid peroxidation in cellular membranes. The accumulation of lipid peroxidation products (such as MDA) facilitates the increase in the permeability of Ca2+ irons. The production of superoxide radicals and the increase of the Ca2+ iron content activate various signals and modulate numerous biological processes, such as improving blood circulation, facilitating wound healing, and promoting the process of angiogenesis. This is the so-called “free-radical mechanism of stimulating effect of LLLI.” 15 –18 Our findings support this point. Laser irradiation reduced the activity of SOD and increased the MDA content significantly. It has been found that laser irradiation could cause an elevation of hydrogen peroxidate and even a little increase in the ROS in cells could activate signal transduction. We postulate that an increase in OFR plays a large role in activating signal transduction to modulate various biological processes. Tuby et al. found that LLLI upregulated the VEGF and iNOS expression in the infarcted heart and had a cardioprotective effect. 11 Yang et al. also demonstrated that LLLI could alter cardiac cytokines, such as granulocyte macrophage colony-stimulating factor (GM-CSF), interleukin-4 (IL-4), cytokine-induced neutrophil chemoattractant-3 (CINC3), and fractalkine. 19 Therefore, we cannot ignore the link between OFR elevation and the biological effects of LLLI. Additionally, Lubart reviewed the evidence supporting that low-level energy light (LLEL) could induce the formation of the reactive oxygen species (ROS) and that the light-induced ROS could stimulate the synthesis and activity of some antioxidants such as SOD in the cell. 20 However, we did not find that the activity of SOD increased following LLLI. Adversely, it was decreased. This might be related to the replacement of the normal myocardium by collagen fibers.
Although Fujimaki et al. found that LLLI could attenuate the production of ROS by human neutrophils in the inflammatory tissues to improve wound healing in smokers, 21 Fishbein et al. 2 did a histological study in rats with MI and found that there was a mild and brief acute inflammation response with neutrophilic polymorphonuclear leukocytes (PMN) at the margins of the necrotic myocardium from day 1 to day 6 post-MI. After 48 h, chronic inflammation was present until the formation of a scar, usually by 21 days. Chronic inflammation cells, such as lymphocytes, infiltrated the periphery of the infarct from 48 h until day 21. 2 This might explain the reasons that LLLI had no effect in reducing the production of OFR, but could not explain the effects of reducing infarct size, left ventricular wall thickness, and collagen fibers. Additionally, the energy density of laser irradiation, 0.96J/cm2, was used in this study to gain maximum benefit and avoid heating injury. Yaakobi et al. in their previous studies demonstrated that the energy density of ∼1 J/cm2 was the “optimal” dose to obtain beneficial effects for the ischemic heart diseases. 22
The pathological process of VR following MI includes necrosis of myocardial cells, hypertrophy of non-necrotic myocardial cells, infiltration of inflammatory cells, development of granulation tissue, and scar formation. 23 The sections of myocardial tissues in this study displayed some of the abovemnetioned pathological changes. The present study further demonstrated that LLLI could reduce the infarct size and attenuate the formation of collagen fibers. Therefore, we think that LLLI could improve VR following MI. The results are in accordance with previous findings. Oron et al. found that LLLI with proper energy density could reduce infarct size by 65% and attenuate formation of scar tissue in rats and dogs with myocardial infarction. 8,9 In addition, LLLI could stimulate proliferation, increase growth factor secretion, and facilitate myogenic differentiation of BMSCs. 13
Conclusions
The present study demonstrates the LLLI has benefits in improving VR following MI, which is possibly mediated by the upregulation of OFR. Future works need to investigate the application of LLLI in MI.
Footnotes
Acknowledgments
This study was supported by the scientific and technological innovation talent foundation of Henan province, China (104200510007). We thank Xiuhua Ren for assistance in histological preparation and morphometric analysis, and Shanfeng Zhang for assistance for technical assistance. We also thank Drs. Di Zhao and Huaijie Zhu for their considerable language editing.
Author Disclosure Statement
No competing financial interests exist.