
Abstract
Introduction
A
Cardiovascular surgery has evolved in the last three decades, particularly regarding the treatment of coronary heart disease, and especially in the surgical treatment of myocardial ischemia caused by coronary artery obstruction. 3 In Brazil, the first studies on myocardial revascularization (MR) were pioneered by Zerbini et al. 4 During the first half of 2011, an average of 208 monthly cardiac procedures were performed at The Heart Institute, The General Hospital at Medical School of University of São Paulo (InCor/HC-FMUSP).
Jatene et al. 5 were the first to perform MR using internal saphenous vein bypass. Nonetheless, saphenectomy site complications can lead to postoperative morbidity, as a result of coronary artery bypass grafting. Moreover, significant incisional complications occur following lower extremity bypass procedures. 6 Saphenectomy dehiscence after MR causes 10% of patients' health debilitation, and increases length and cost of hospital stays. 7
Studies performed in patients undergoing MR showed that several factors are associated with morbidity, changing the normal healing process. Among them are diabetes mellitus (DM), hypertension (HBP), dyslipidemia (DLP), older age, and cardiopulmonary bypass. 7 –9
Low-level laser therapy (LLLT) is one of advanced healing tools, accelerating and optimizing the tissue repair process. 10 –12 There is evidence that LLLT advances tissue repair by enhancing RNA, DNA, 13 and adenosine triphosphate (ATP) synthesis, 14 facilitating angiogenesis, 15 fibroblast proliferation, 16 collagen, and other tissue component synthesis, 17 –19 as well as promoting immunologic action. 20 Although there are few studies detailing LLLT in surgical prevention, 21 Chavantes 22 has shown positive results, avoiding dehiscence in sternotomy as well as in saphenectomy, 7 which presented a significant reduction in morbidity rates. By preventively applying LLLT, Pinto et al. 23 found a decline in the incidence of surgical wound dehiscence in neonates who underwent surgical repair of congenital myelomeningocele.
The purpose of the study was to evaluate tissue repair in prodromal saphenectomy incisions applying LLLT in patients undergoing MR.
Materials and Methods
Patients
This work was a pilot study with 14 patients (5 women and 9 men), who presented prodromal signals on the saphenous incision post MR were selected. Patients were divided equally into two groups: The Laser Group (G1) – conventional therapy plus laser irradiation on surgical incision (n=7) The Control Group (G2) – conventional therapy only (n=7)
All patients were evaluated within the first 12 h (immediate postoperative [IPO]), 48 and 72 h post-surgery, subsequently on the 7th day (prior to hospital discharge), and subsequently on the 15th, 30th, 60th, and 180th days following the surgery.
The present study was conducted at The Laser Medical Center, The Nursing Department and The Cardiovascular and Thoracic Surgery Department of The Heart Institute, General Hospital, Medical School, University of São Paulo (InCor-HC/FMUSP). Data were collected after the approval of the Ethics Research Committee of The Heart Institute (InCor-HC/FMUSP). Patients read and signed the written informed consent. All groups were randomly sorted.
Exclusion criteria
Criteria for excluding potential research subjects included: (1) immunosuppression; (2) infection; (3) respiratory, kidney, or liver failure; or (4) class III or IV obesity.
Treatment
A continuous wave (CW) diode laser (GaAlAs–780 nm) with beam area=0.04 cm2 (Twin Laser from MM Optics, São Carlos-SP, Brazil) was used under the following specifications: fluence=19 J/cm2, output power=25 mW, exposure time=30 sec, spot size=0.04 cm2, irradiance=625 mW/cm2, energy=0.75 J, were applied surrounding the entire surgical perimeter wound edge (each 2 cm). Dosimetry was kept even with the incision reduction. The points' numbers were changed for each patient, according to wound's size. Laser irradiation applied at the following intervals: 2nd PO and 4th PO day in the intensive care unit (ICU). All patients received conventional treatment in the ICU, where cleaning was performed using saline solution (SS) at 0.9% and gauze occlusive dressing every 24 h.
Surgical incision
The suture closed material used was synthetic absorbable poly (glycolide E-caprolactone) monofilament, 4350-40XF (4-0, MONOFYL®).
A single, independent, experienced investigator documented and compared the surgical incisions. Regardless of the absence or presence of any alterations, all patients were examined, with the investigator taking particular care to report on the progression of inflammatory processes. The data were evaluated and categorized into the following: erythema, edema, blister, hematoma, transudation, and dehiscence on saphenectomy. A A visual analogue scale (VAS) was used to evaluate incision pain, and it was classified from zero (no pain) to 10 (maximum pain).
Statistical analysis
A nonparametric test to compare and to evaluate proportions was performed, to verify qualitative variables A χ2 test was performed, and significant statistical variables up to 5% (p value<0.05) were used.
Results
Patients were homogenous and similar. Regarding gender, 71.4% were male in G1, and 100% were male in G2. The same percentage in both groups (71.4%) had dislipidemy. In G1, 100% had hypertension compared with 71.4% in G2. Approximately 71.4% of the patients in G1 had diabetes compared with 57.4% in G2. Around 71.4% of the patients in G1 developed wounds on the left leg compared with 85.6% in G2 (Fig. 1).
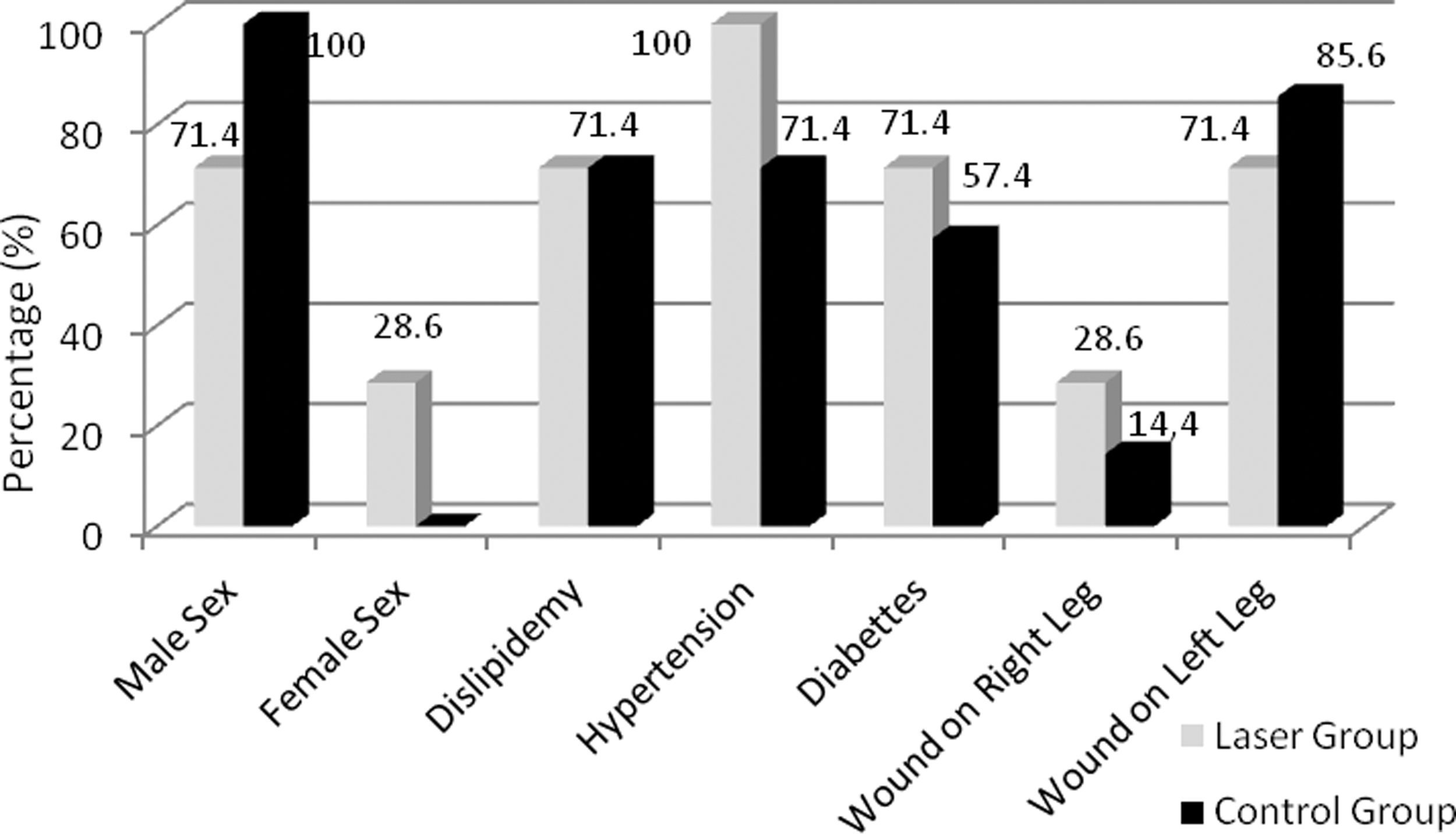
Population characteristics in both groups.
Mean age was 63 years (range 39–84). Upon examination, the following assessment was made regarding the presence of inflammatory signs: in G1, seven patients had erythema, four had edema and hematoma, six had blisters, and two indicated pain; in G2, six patients had erythema and blisters, three had edema, one had hematomas, and none indicated pain (Fig. 2).
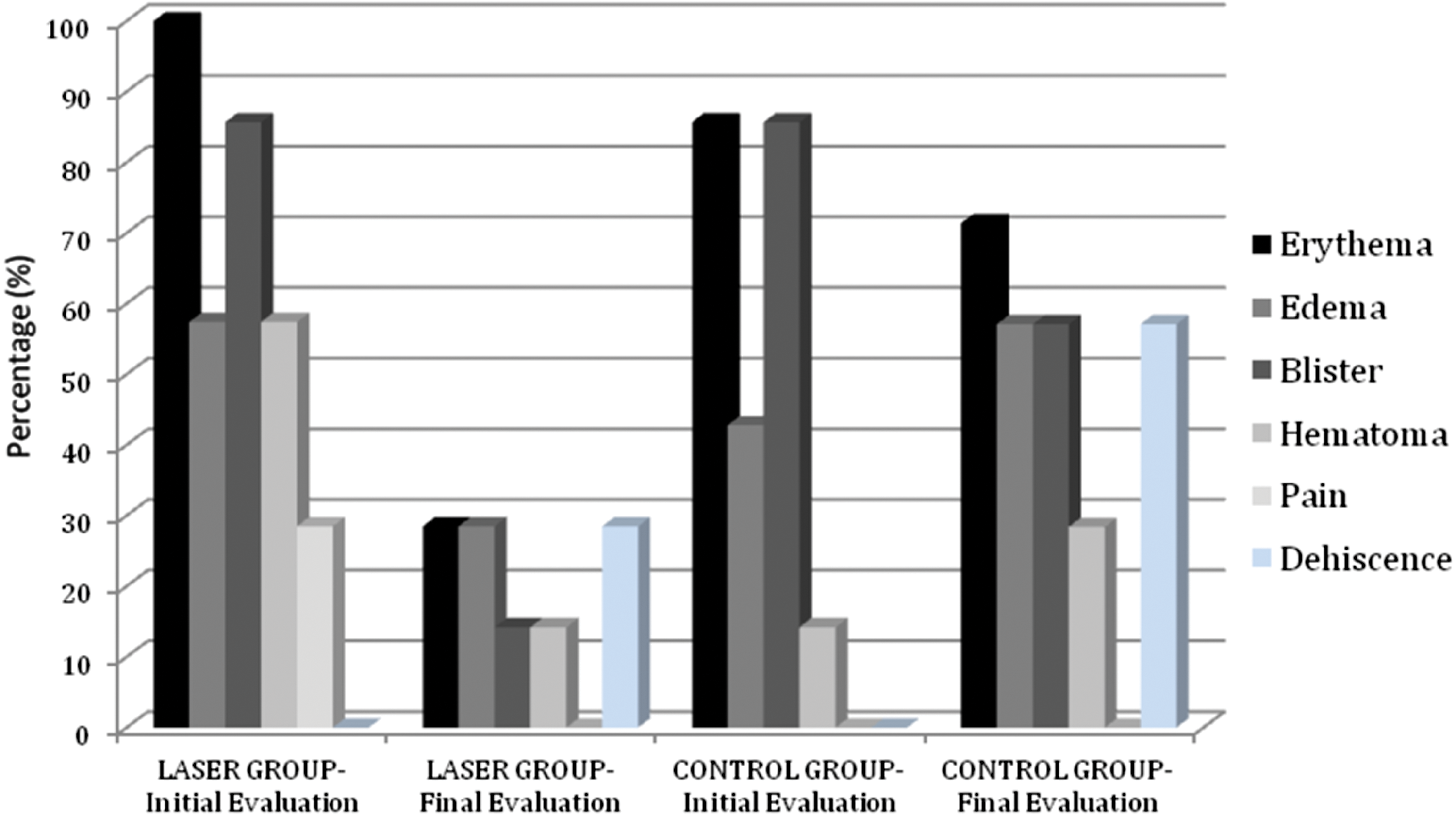
Prodromal signs in saphenectomy incision, initial (immediate postoperative <12 h) and final assessment (7th postoperative day).
It is noteworthy that, before treatment, G1 patients exhibited conditions that were more acute than those experienced by patients in G2.
All patients were assessed prior to discharge. The patients' distribution according to inflammatory signs was as follows: in G1, only two patients had erythema and edema, one had decreased blisters and hematomas, and none reported pain. In G2, five had erythema, four had edema and blisters, and two had hematomas (Fig. 2), all without pain. Altogether, G1 showed significant improvement of the prodromal signs, whereas G2 exhibited a worsening in the inflammatory process. It is noteworthy that, before treatment, G1 patients exhibited worse conditions than those experienced by patients in G2.
Five patients (71.4%) from G1 had saphenectomy repair following hospital discharge. From this group, only two cases (28.5%) presented a small dehiscence (length=1 cm). On the other side, four patients (57.1%) from G2 developed saphenectomy dehiscence. Two patients (28.5%) experienced uniform and continuous healing. We were unable to contact one of the patients after discharge.
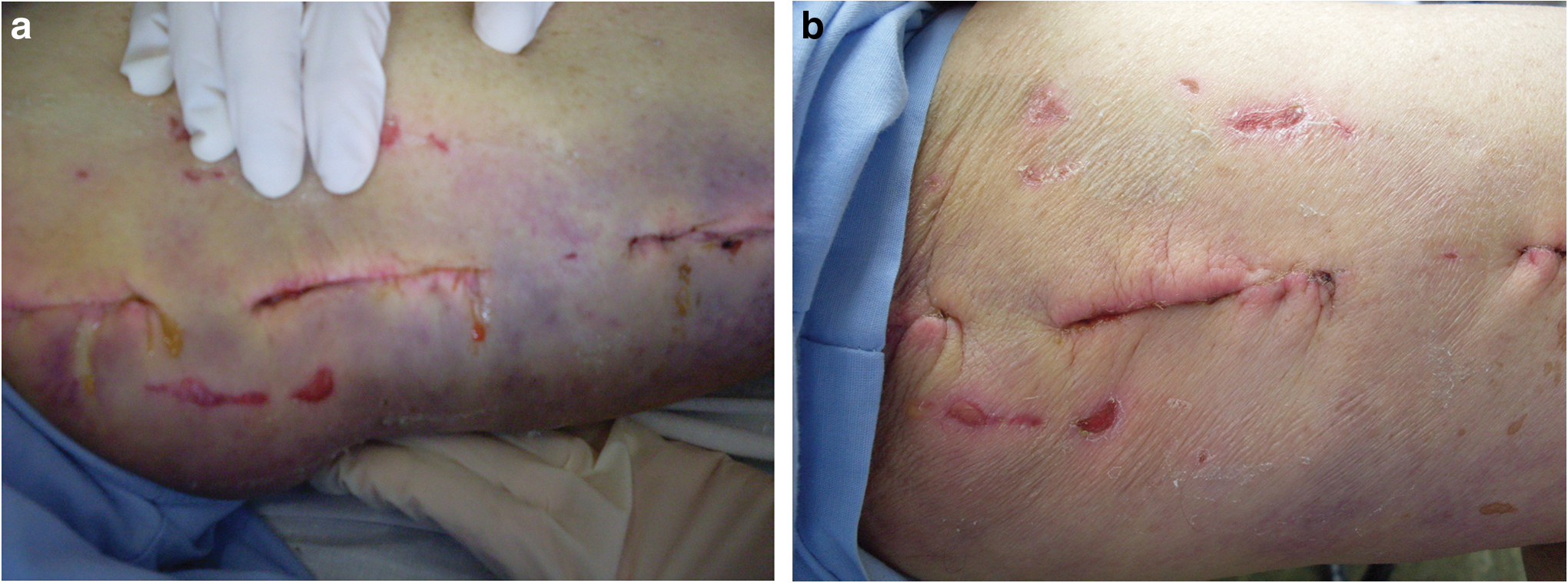
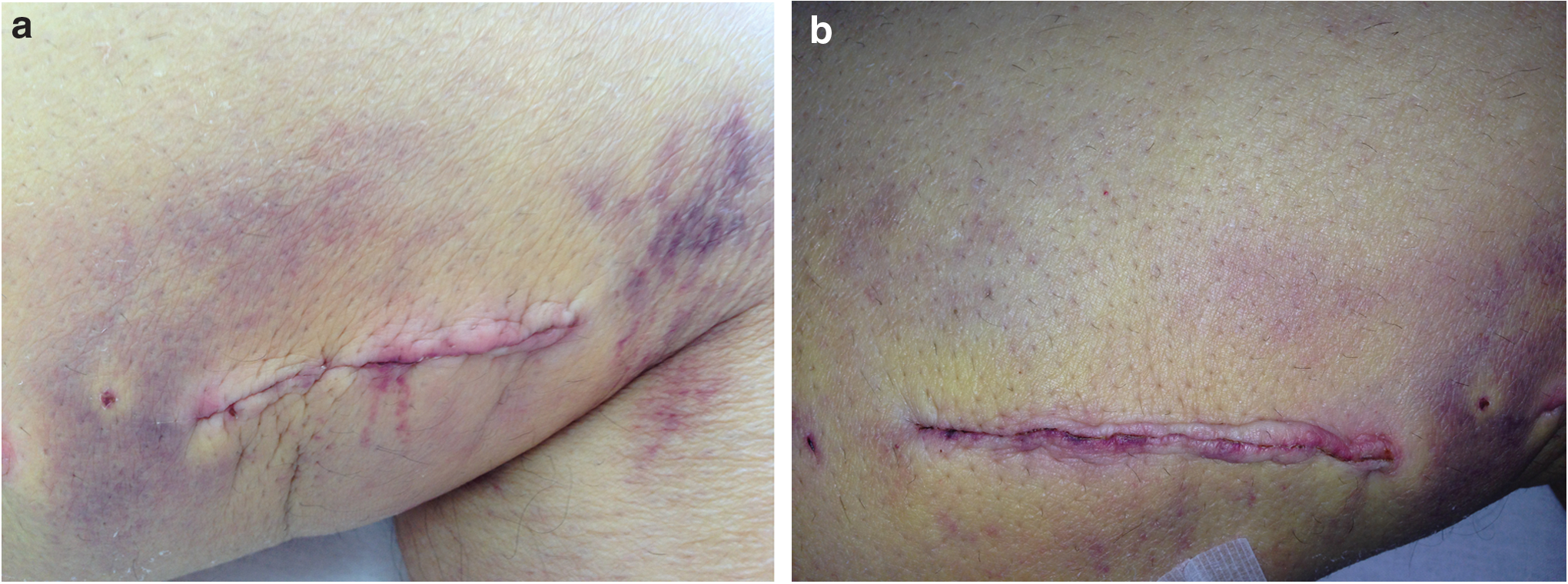
The presence of erythema, edema, hematomas, and transudate in the surgical incision can be noted in Fig. 3a. Figure 4a shows an incision with signs of edema and erythema. In G1, post laser therapy treatment, it was possible to observe hematoma reabsorption (Fig. 3b), without secretion. In the Control Group, prodromal signs worsened over time (Fig. 4b). All patients were discharged 7 days after the surgery.
No statically significant signs of inflammation were observed between the Laser and the Control Groups (p=0.10), with the exception of erythema (p=0.05).
Discussion
Cardiovascular surgeries are complex procedures. Therefore, postoperative morbidities—frequently experienced by patients undergoing saphenectomy—are not only dreaded because of possible complications, but they can also manifest in increased hospital stay and cost both for patients and institutions. The Heart Institute InCor- Medicine Faculty of University Hospital performs almost 3000 cardiovascular procedures/year. It is important to note that this number has been increasing at staggering rates. MR accounted for 856 cardiovascular operations/year in the 1980s. Nowadays this figure has increased to 1106 operations/year. 24
As we face a considerable number of MRs performed at InCor and the risk of saphenectomy dehiscence occurs, the fundamental importance of this study—preventing such morbidity—becomes clear. Complications in surgical incisions are common when wound dehiscence occurs. Any complications incurred by saphenectomy are predicated on the surgical techniques employed in the procedure, as well as on the patients' overall health.
Dalman et al. observed in their study that metabolic conditions are a significant predictor of wound complications. 6 We observed in this pilot study that most patients who developed dehiscence had hypertension and diabetes, although this were not statistically significant. Cardiovascular literature reports that metabolic disorders increase risks of postoperative complications, and this was encountered in our work as a key factor. 25 Factors such as diabetes, dyslipidemia, being elderly and female, and vascular disease may contribute to wound infection and delayed wound healing, 26,27 as we observed in our groups.
Most researchers report that LLLT is an effective tool to accelerate the tissue repair process, as well as to treat pain that does not respond to conventional medical treatments. 28 –30
In our study, only erythema was found to present a statically significant difference (p=0.05) when comparing G1 and G2. Laser therapy has proven to be beneficial in the management of saphenectomy incisions. The present data and findings indicated that there was no statistically significant divergence (p=0.10) between the Laser and the Control Groups for prodromal signs—most likely because of the small size of sample groups in this pilot study.
Minatel et al. showed that the combination of 660 and 890 nm lights promoted tissue granulation and rapid healing of diabetic ulcers, particularly when these failed to respond to other forms of treatment. 28 According to Mester et al. and Medrado et al., groups receiving fluence=4 J/cm2 always presented better cicatrization. They concluded that LLLT reduced the inflammatory process, increased collagen deposition, and induced greater proliferation of myofibroblasts in cutaneous wounds. 30,31
Regarding the parameters of our study in the Laser Group (G1), the infrared laser was applied only twice, and it is possible that the low energy administered to patients was insufficient to completely heal all patients' wounds effectively, as later on in G1, one patient progressed to a small dehiscence. Nonetheless, all patients in the Control Group developed significant dehiscences, as well as twice as many complications as those in the Laser Group.
Campana et al. suggests that the laser action on the tissue is related to the possibility of inhibiting the occurrence of chemotactic factors during the initial stages of inflammation. 32,33 It is believed that applying LLLT in the early inflammatory phase is essential to obtaining good results, 15 as we found. In the Control Group (G2), all patients developed a posteriori saphenectomy dehiscence.
As observed during follow-up examinations, >50% of patients with total wound healing, following only two LLLT applications, belonged to the Laser Group. Only one patient in Laser Group presented a small dehiscence. It is possible that patients in the Control Group experienced a greater number of complications because of risk factors and, possibly, the absence of LLLT's adjuvant therapy.
In consonance with the results established by this study, it can be asserted that patients treated with LLLT, including those with diabetes and other metabolic disorders, undergo an effective healing process, especially in the prevention of post-saphenectomy dehiscence, although the study does not evince a significant statistical response. Another factor to be credited is the patients' financial burden; those patients who develop dehiscence had higher costs because of prescribed medicines.
Further study is required to determine the actual efficacy of LLLT, and its potential and value in the management of saphenectomy incisions.
Conclusions
This pilot study reports an effective response applying laser therapy in the early stage dehiscence (prodromal signals) immediately after surgery, which then avoids several complications. Our work indicates that it is possible to prevent morbidity in patients undergoing saphenectomy post MR, with cost effectiveness, by using LLLT.
Footnotes
Author Disclosure Statement
No competing financial interests exist.