
Abstract
Introduction
The relationship between PPP and psoriasis, however, is controversial. Up to 24% of PPP patients have psoriasis, 3 which is much higher than the normal population prevalence of psoriasis. Therefore, it may be associated with other forms of psoriasis, although it appears to be a distinct entity in terms of epidemiology, pathophysiology, and genetics. The age of onset is usually between 30 and 50 years. 3,5 PPP is more common in females, with a sex ratio of 4.6 to 11.5, 3,5 and is strongly associated with tobacco smoking 6,7 and thyroid dysfunction. 6 In a small proportion of patients, it is associated with an arthritis of the sternocostoclavicular joint 8,9 and streptococcal tonsillitis. It has been reported that psoriasis susceptibility gene 1 (PSORS1) locus in the major histocompatibility complex region (the major genetic determinant for psoriasis vulgaris) is not associated with PPP. In this study, PPP appears to be a distinct disorder. 10
PPP is a debilitating illness that interferes with work and with everyday activities involving the hands, mobility, and daily activities. Patients with PPP show an increased negative social and psychosocial impact with decrements in quality of life (QOL). 11
PPP is characterized by sterile pustules localized in the lowest part of stratum corneum and erythematous, scaly skin confined to the palms and soles. PPP has some common features with other pustular forms of psoriasis and is often classified as a localized form of pustular psoriasis. The histology of the skin lesion of PPP and other pustular forms of psoriasis share many common features, such as spongiform pustules and a mononuclear inflammatory infiltrate. 12
Treatment is difficult, requiring systemic therapies in some patients. The choice of treatments is heavily influenced by their side effect profiles. Treatments are often disappointing and may cause side effects. Topical treatments consist of emollient creams, corticosteroid preparations, tar and anthralins, or topical retinoids. They tend to be ineffective for PPP and only suitable for a short period of therapy. Systemic treatments include retinoids, photochemotherapy (PUVA), retinoid PUVA (re-PUVA), tetracycline, other antibiotics, cyclosporine, and methotrexate.
PPP is often recalcitrant to therapy, and acitretin, although an effective systemic treatment, is associated with mucocutaneous side effects, lipid and hepatic abnormalities, and risk of teratogenicity. 13,14 None of the aforementioned treatments can reliably induce remission, or maintain it once it is achieved. 1
PPP has some common features with psoriasis and recently, for treatment of localized psoriasis and palmoplantar psoriasis, a series of devices emitting focal UVB light have been introduced such as the monochromatic excimer light (M.E.L.) or the excimer laser. Both have a wavelenghth of 308 nm and have been reported to be effective and safe and to offer long-term remission. 15
A very recent technology, Alba 355 nm, which administers energy in the UVA-1 spectrum, has been used in the treatment of psoriasis. 16 This instrument is based on a 1064 wavelength neodymium-doped yttrium orthovanadate (Nd:YVO4) laser, optically pumped using a 808 nm infrared beam able to achieve a third harmonic 355 nm wave delivery. Possibly, the repeated treatments may achieve a prolonged and stable relapse-free state, through a modulation of the local immune response, T cell depletion, and alterations in apoptosis-related molecules.
Because no previous studies were performed to evaluate the efficacy and safety of Alba 355 nm in the treatment of PPP, we conducted an open trial in order to confirm the same observations and find an alternative therapeutic approach in the management of PPP.
UVA-1 has a deeper penetration in the skin than does UVB, and its biological effect can be produced selectively at the level of the inflammatory cell infiltrate of the disease, inducing cell death via apoptosis.
The aim of the present study was to investigate for the first time the efficacy, side effect profile, and patient tolerability of of a monochromatic light in the UVA-1 range, in the treatment of this recalcitrant disease.
Patients and Methods
This was a pilot perspective study performed on patients affected with PPP. We treated 33 patients affected with PPP on the palm, sole, or both with Alba 355 nm. Participants included 21 men and 12 women (Fitzpatrick skin types II–IV), mean age of 42.6 (range, 23–67)±13.67 years, affected with PPP for an average of 12 years and with a Palmoplantar Pustular Psoriasis Area and Severity Index (PPPASI) 17 ranging from 2.4 to 11 (Table 1).
Number of cigarette/day>15 and years smoking>5.
Alterations T3, T4, thyroid stimulating hormone (TSH), thyroperoxidase (TPO).
PPPASI, Palmoplantar Pustular Psoriasis Area and Severity Index.
The local ethical committee gave its approval to this study (Tor Vergata Ethical Committee Protocol PSOPPL 11–2012).
All patients gave informed consent, and were instructed to avoid use of any topical medication during treatment. Patients with a history of skin cancers or photosensitivity-related disorders were excluded. Patients who had been on systemic medication for < 8 weeks or phototherapy for 4 weeks, or had used treatments within the past 2 weeks, were also excluded.
Patients were instructed to wear protective glasses while palmar and plantar areas were selectively treated. At every session, new morphological and photographic evaluations were performed.
Subjects were classed as “complete responders” if they had a decrease in PPPASI and in the number of new and total pustules of > 75% as compared with baseline, “good responders” if they had a decrease between 50 and 75%, “poor responders” if they had a decrease between 25 and 50%, and “nonresponders” if they had a decrease between 0 and 25%.
All patients completed the treatment with 16 sessions and had a 3 month observation.
Laser source and therapeutic protocol
The energy administered in the UVA-1 spectrum was produced using a new laser technology, that is, laser Alba 355 (Elettronica Val Seriana, Casnigo, Italy).
The solid-state laser uses an active media and an Nd:YVO4 crystal that is “energetically pumped” by another laser with 808 nm wavelength. The light emitted by the Nd:YVO4, at a wavelength equal to 1064 nm, is impulsed through an acoustic optic crystal called “Q switched,” which produces a frequency of 20–50 kHz and transforms the laser light in an ultra-short pulsed light (25 nsec). This pulse rate is > 20 kW and it is sent to crystals in order to duplicate and triplicate the 1064 nm light frequency, producing second (532 nm) and third (355 nm) harmonic light frequency delivery. The laser beam is then filtered by a harmonic separating crystal in order to select from its galvanometric head a 355 nm wavelength specific beam that is amplified and homogenate, just before galvanometric head output, with a 2.5 mm spot and a pulse repeating potential up to 50,000 spots/sec and designing variously shaped bidimensional figures.
The dose was calculated according to patient skin type, erythema, pustules, and desquamation component of the lesions.
The therapeutic protocol consisted of the administration of moderate to high fluences (80–140 J/cm2), according to the skin type and morphology. Treatment was administered two to three times every 7 days without an increase of the previous dose. In patients who evidenced a complete remission, we administered a maintenance application of 80 J/cm2 every other week until we reached a 90 day follow-up visit. At each visit, reduction in size and flattening of lesions; reduction of erythema, pustules, and scaling; or the appearance of side effects were reported. Clinical evaluation was performed before every session and PPPASI was calculated every 2 weeks.
Results
After a mean of five sessions of UVA-1 laser treatment, all patients evidenced an improvement of the PPPASI. Changes in PPPASI were significant after 8 weeks of treatment (p<0.05). This significance was maintained at week 16 and at the follow-up visit (Figs. 1 and 2).

Palmar pustular psoriasis at baseline.
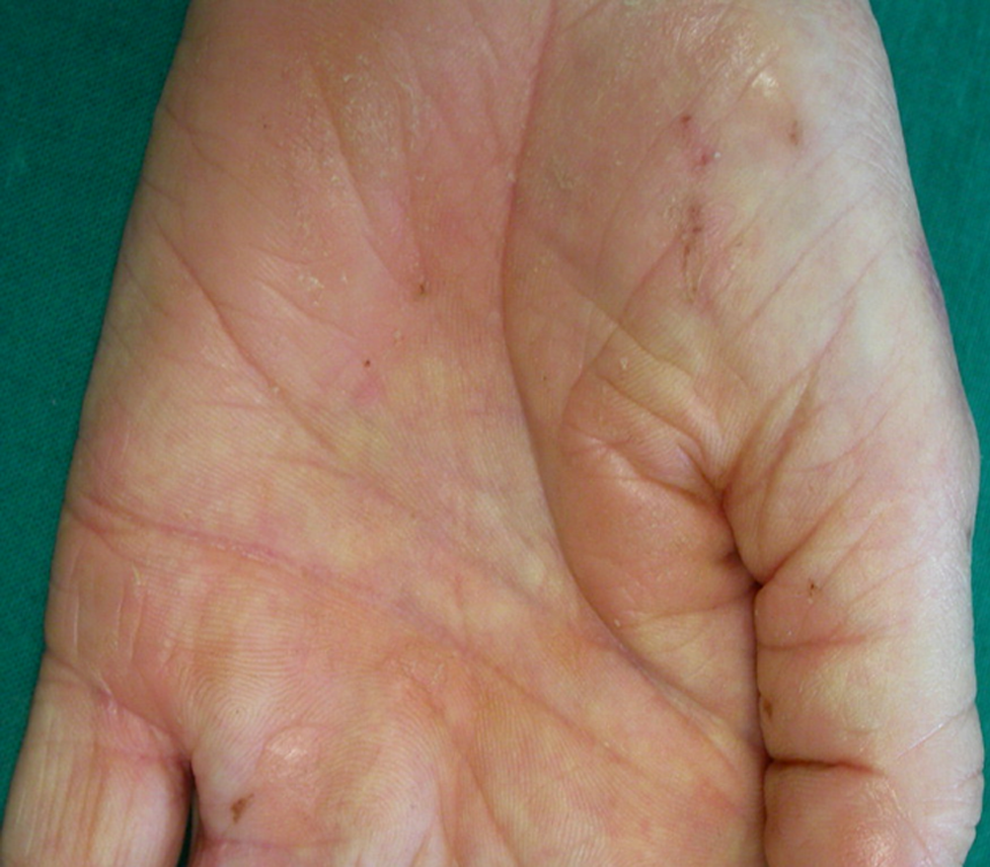
Complete remission.
After 3 months, a complete remission was evident in 22/33 patients (>75%), a good remission was evident in 5/33 patients (25%), and a moderate improvement was evident in 5/33 patients (17%) (Table 2). This benefit was maintained at 3 month follow-up in 27/33 patients. Notably, 12/33 patients achieved a total remission of the lesions.
Response Rate, reduction of Palmoplantar Pustular Psoriasis Area and Severity Index (PPPASI) score at 3 month follow-up: 0–25% poor; 25–50% moderate; 50–75% good; 75–100% complete.
Side effects: mild erythema, oedema.
A prolonged erythema (24–48 h) with a mild pruritic sensation was evidenced in 8/33 patients after the first and second application.

Plantar Pustular Psoriasis at baseline.
Formation of vesicles and edema were observed after three sessions in 2/33 patients. These resolved after a local treatment with hydrocortisone 1% ointment for 3 days.
However, the patients responded to the following sessions and completed the treatment successfully.
Discussion
The efficacy of UVA-1 for treatment of psoriasis is controversial. According to the literature, good results have been reported; 18 however, these findings do not support the results reported by Krutmann suggesting that UVA-1-based phototherapy should not be used for inflammatory skin disorders. 19
The present study showed for the first time the clinical efficacy of the application of a monochromatic UVA-1 laser therapy for the treatment of PPP, a condition that has been reported to be responsive to monochromatic UV light at different wavelengths. 15
The monochromatic coherent and coordinate UVA-1 light (laser therapy) used in the present study (wavelength of 355 nm) has shown a high success rate in the treatment of mild to severe psoriasis, 16 reaching both the epidermis and the dermis, indicating the need of further laboratory studies to assess every aspect of its biological effects.
The present study, conducted on 33 patients, affected by moderate to severe PPP (PPPASI between 2, 4, and 11) showed a significant improvement in the PPPASI score after only 2 weeks (four to six sessions) in patients treated with 80–140 J steady doses, suggesting a possible use for treatment of other chronic dermatological diseases that share the same immune-inflammatory background. The safety profile of UVA-1 is high, as only mild side effects have been reported, and those occasionally, similarly to those in the study conducted by Zerbinati et al. 16 on plaque type psoriasis. These included mainly erythema and, only in few patients, formation of vesciculation and edema.

Remission after treatment.
From a therapeutic perspective, exposure to UVA-1 radiation therapy can be divided into low (10–30 J/cm2), medium (40–80 J/cm2), and high (80–120 J/cm2) doses. Low doses are administered with fluorescent lamps with low-cost instrumentation and maintenance costs. High energy fluences (>100 J/cm2) can be delivered only with metal-halide lamps that have high costs and time-limited fluorescence. The use of a monochromatic laser source emitting in the UVA-1 range (355 nm) would make it possible to achieve high brightness compared with the traditional gas-discharged tubes, lowering the exposition time while administering always the same dose. The qualitative and quantitative brightness of a monochromatic laser source would be superior to all the devices used so far in this field.
Another interesting point observed is that UVA-1 radiation does not require a progressive increase to achieve therapeutic efficacy in comparison with 308 or 311 nm UVB therapy. Furthermore, the advantage given by the monochromatic radiation is to selectively deliver high energy quantities on the lesions in considerably less time than traditional lamps. Five cm2 areas can be irradiated with a time of application 10 times less than that for metal halide. Moreover, the proposed instrument is considerably less expensive than metal-halide lamps, which also require constant maintenance to maintain high tube brightness. The proposed UVA-1 is able to maintain a stable brightness for a number of hours, consisting in 20,000 deliveries, and with the possibility of delivering up to 100 J/cm2 in 12 sec. This leads to a possible selective treatment of 5 cm2 psoriatic plaques in 1 min if compared with UVA-1 instruments that deliver a total body of nearly 100 J in 45 min. Moreover, it is evident in the difference in the therapeutic outcome, and in the patient's satisfaction, as focusing attention on the body's lesions can affect the person's psychosocial balance.
The present study shows how UVA-1 radiation makes it possible to achieve a higher dermis penetration accompanied by a greater biological and immunological response 20 –22 on both the dermis and epidermis than with UVB radiations. Cell damage of inflammatory cells is effected mainly via apoptosis.
In our opinion, further data are needed to determine how the UVA-1 remission rate may be maximized in order to provide patients good long-term control of their disease. A study to prove longer term results is in progress.
Conclusions
In this study, we evidenced the benefits of UVA-1 laser such as a selective use of high doses with a partial or total remission in >75% of the patients.
This novel UVA-1 laser is, therefore, to be considered as a valid option in the treatment of PPP with an overall efficacy even in absence of topical/systemic drugs, although we suggest the chance for combined therapies. Furthermore, it represents a novel and useful alternative to existing therapy (e.g., psoralen plus UVA treatment or cyclosporine), and these results suggest that it is an effective and well-tolerated treatment for PPP.
Footnotes
Author Disclosure Statement
Dr. Zerbinati has received speaker fees from EV Lasers. The other authors have no competing financial interests.