
Abstract
Introduction
The recommended procedure for achieving the goal of being minimally invasive is to begin any restorative dental processes by only removing infected tissue, retaining any affected tissue that may be capable of remineralization. Therefore, when a glass ionomer cement (GIC) provisional restoration is inserted in the cavity, the final restoration will be performed after waiting for an adequate pulp response and, consequently, dentine hardening. This aims to decrease bacterial colonization and increase the pH.
The Er,Cr:YSGG laser has a wavelength of 2.78 μm, which coincides with the peak absorption of water and hydroxyapatite. This laser is capable of removing hard dental tissue and is, therefore, suitable not only for cavity preparation but also for the removal of caries-infected dentine, conditioning of dental tissues, and reduction of microbial counts inside the prepared cavity. 2,3
Irradiation with an Er,Cr:YSGG laser causes an irregular dentine pattern without smear layer, with open dentinal tubules, protruded peritubular dentine, 4 and a microretentive morphological pattern that is allegedly favorable for adhesive procedures. However, the laser parameters for both dentine conditioning and cavity preparation have not been yet standardized, leading to conflicting results. Certain authors 4 –9 have observed a reduction in bond strength (BS) in irradiated dentine, whereas others 10 have demonstrated that for cavity preparation, the BS was greater for irradiated dentine than for drilled dentine.
It is important to emphasize that, depending upon the energy density that is used, laser's thermomechanical effects may cause a superficial denaturation of collagen fibrils on subsurface dentine. 9 This collagen denaturation results in the formation of an acid-resistant surface with granular structures that is either carbonized or covered by dentine melting products. 9 Thus, this denaturation hinders the infiltration of the adhesive system into the dentine, thereby adversely affecting hybrid layer formation and resulting in compromised adhesive resistance. 11,12
The majority of articles have evaluated the BS over sound dentine, although the clinically relevant substrates are sclerotic and caries-affected dentine. As caries-affected dentine is a soft tissue, with characteristics distinct from those of sound dentine, an adjunct procedure to obtain a hard tissue before the insertion of the final restoration should be performed. In this context, GIC are highly indicated, as they release fluoride 13 and chemically adhere to the dental substrate by ionic diffusion. 14 The increase in dentine surface mineral content and the alterations in collagen protein conformation caused by Er,Cr:YSGG laser irradiation are likely to impair the BS of materials such as GIC. 15 However, few studies have evaluated the effects of the Er,Cr:YSGG laser on the BS of conventional GICs, 8,10 and the results of previous investigations are contradictory.
Because of the laser's ability to condition dentine, it is believed that the association of laser and GIC is highly indicated for conservative procedures and preparing a cavity for a final restoration. The establishment of adequate irradiation parameters for these applications is, therefore, critical.
Therefore, the objective of this study was to identify the optimal parameter for dentine surface conditioning with an Er,Cr:YSGG laser that will be restored with a conventional GIC.
Materials and Methods
Sampling
Eighty-five extracted human third molars (n=17) were used in this study, which was approved by Research Ethics Committee of the University of São Paulo (USP) under the protocol of 120/11.
Sample preparation
Enamel and superficial dentine of the crown were grounded perpendicularly to the tooth long axis to expose a flat surface. This was obtained with silicone carbide paper under running water with the aid of a polishing machine under water cooling (Ecomet 6/Automet, Buehler Ltd., Lake Bluff, IL). The exposed flat surfaces were then polished with wet 600 grit silicon carbide paper. 16
Experimental groups
Teeth were randomly divided into four groups (n=17), according to the conditioning protocol, as follows: G1: No conditioning G2: Conditioning with Er,Cr:YSGG laser (power of 0.5 W, 25 mJ per pulse, and an energy density of 9 J/cm2) G3: Conditioning with Er,Cr:YSGG laser (power of 1.0 W, 50 mJ per pulse, and an energy density of 18 J/cm2) G4: Conditioning with Er,Cr:YSGG laser (power of 1.5 W, 75 mJ per pulse, and an energy density of 27 J/cm2) G5: Conditioning with GIC liquid, which contains polyacrylic acid, for 10 sec, as recommended by manufacturer.
Samples had their surfaces analyzed by SEM (n=2) and the remaining teeth were subjected to the micro-shear test (n=15).
For tooth irradiation, an Er,Cr:YSGG laser (Waterlase, Biolase Technology, San Clemente, CA), from the Biophotonics Laboratory of the Nuclear and Energy Research Institute (São Paulo, Brazil) was used. This laser has a 2.78 μm wavelength with a pulse duration of 140–200 μs, a fixed 20 Hz repetition rate, and an average output power that could be adjusted from 0 to 6W. The equipment was cooled with an air/water spray that was used at 65% air pressure and 55% water pressure. 5,8 A model “G” sapphire fiber tip was attached to a #2415 hand piece (Millennium, Biolase, San Clemente, CA). The specimens were mechanically irradiated for 50 sec with an XYZ micropositioner (Model ESP 300, Newport Corporation, CA) with automatic pitch shifting, at standardized speed (6.0 mm/sec) and distance (200 μm) of specimen displacement between laser pulses, thereby avoiding the creation of any gaps between the laser pulses.
Sample restoration
Tygon tubing molds (R-3603, Norton Performance Plastic; Cleveland, OH) were mounted on the dentin surface, delimited by an adhesive tape. 17 GIC (Ketac™ Molar Easymix- 3M- ESPE, SP, Brazil) was manipulated in accordance with the manufacturer's instructions. Two to four cylinders of GIC, ∼0.8 mm in diameter and 0.5 mm in height, were bonded to each dentinal surface. After the material had lost its glossy aspect, a layer of acid-resistant varnish was applied to the top of each test specimen. 18 Specimens were stored at 370C for 24 h, prior to removing molds with a scalpel blade. The specimens were then stored in water at 370C for 24 h.
Micro-shear bond strength test (μBS)
Before the micro-shear test was conducted, all samples were checked under an optical microscope (40×magnification) for defects (Olympus SZ-PT; Tokyo, Japan). Samples that showed interfacial gap formation or bubble inclusion were excluded from the study and replaced by another sample. Specimens were mounted in a jig to place the GIC/tooth interface parallel and as close as possible to a wire (diameter 0.20 mm) that was looped around the GIC cylinder, in contact with half of the cylinder base. The micro-shear test was performed at a crosshead speed of 1 mm/min using a universal testing machine (Mini Instron 4442, Instron; Norwood, MA).
The micro-shear bond strength was calculated by dividing the maximum load at failure by the cross-sectional surface area of the bonded surface. If a spontaneous interfacial debonding occurred while the specimens were being mounted or sectioned, the bond strength was recorded as 0 MPa.
Fracture pattern analysis
All tested samples were first stained by immersion in 2% Ponceau S solution for 5 min and washed for 10 min, and were examined under optical microscope at 40×magnification to identify failure mode. The fractures were categorized as follows: Type I – adhesive failure between GIC and dentine; Type II – cohesive failure in dentine; Type III – cohesive failure in GIC; or Type IV – mixed failure (when cohesive failure of GIC and adhesive failure occurred in the same specimen). Two specimens that experienced each fracture type were then randomly selected, dehydrated in sequential baths of alcohol, and gold-sputtered for SEM evaluation (MEV, JEOL JSM 6460LV, Jeol Ltd., Tokyo, Japan).
Analysis of the dentine surface with SEM
Two specimens from each group were observed under SEM (JEOL JSM 6460LV, Ltd., Tokyo, Japan) at standard magnifications of 30×, 500×, and 2000×. After applying the irradiation protocol according to experimental groups, samples were fixed in 2.5% glutaraldehyde solution for 24 h at 4°C, dehydrated in sequentially ethanol baths for 10 min each (30%, 50%, 70%, 90%, 96%, and 100%, for 20 min) and then transferred to a critical-point dryer (HMDS) for 30 min. The specimens were mounted, gold-sputtered at 10 mA for 1 min, and analyzed.
Statistical analysis
Data were analyzed using one-way analysis of variance (ANOVA) and Bonferroni's post-hoc test (Minitab 14 Software Minitab; State College, PA) to perform group comparisons (p<0.001).
Results
Morphological evaluation of dentine surface
At the lowest magnification (30×) (Fig. 1 G1A), G1 samples, with no conditioning, showed regular dentine surfaces covered by smear layer that obliterated the entrance of the dentinal tubules. At a higher magnification (500×) (Fig. 1 G1B), it was possible to observe pathways left on the surface by the sandpaper, whereas at the 2000×magnification (Fig. 1 G1C), the marks of the openings of a number of dentinal tubules could be detected, indicating that the smear layer over the sample was rather thin.
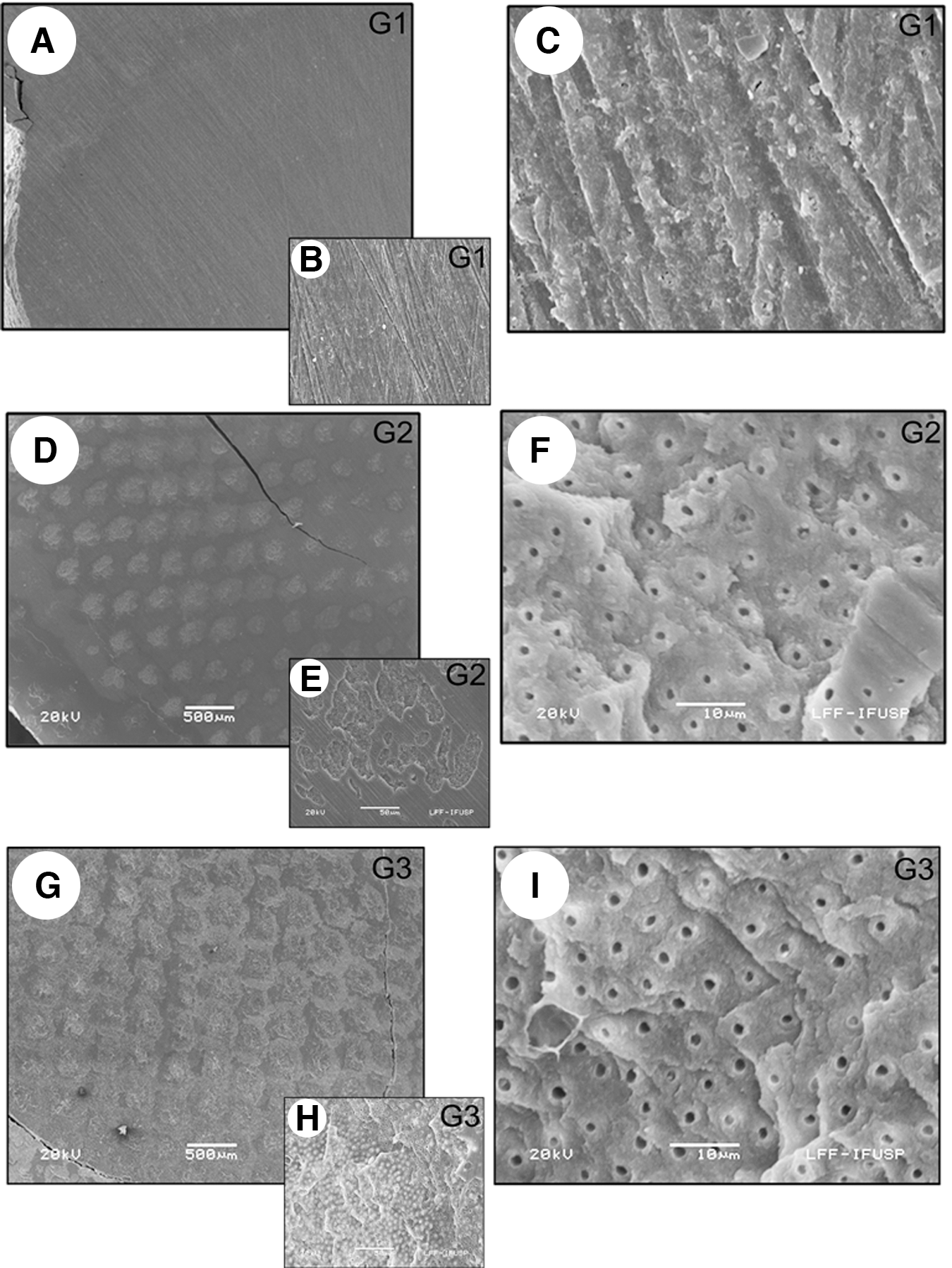
Scanning electron microscopic (SEM) micrographs of dentine surface with no pretreatment (G1A–C) conditioned with Er,Cr:YSGG laser with energy density of 9 J/cm2, 0.5 W average power, 25 mJ/pulse (G2D–F) and with energy density of 18 J/cm2, 1.0 W average power, 50 mJ/pulse (G3G–I). In G1A (30×) the smear layer covers the entire dentine surface; in G1B (500×) there are marks left by abrasion with sandpaper; in G1C (2000×) the location of the opening of some dentinal tubules can be identified, indicating a thin layer; in G2D (30×) the laser pulses can be easily distinguished, and there is smear layer between them; in G2E and G3H (500×) the irradiated dentine is irregular, with opened dentinal tubules and smear layer remains covering some of the surface; in G2F and G3I (2000×) peritubular dentine can be easily detectable; and in G3G (30×) the laser pulses can be easily identified. There is a small amount of smear layer between pulses, but it is hard to delimit its boundaries.
For samples that were irradiated with an energy density of 9 J/cm2 (G2), at 30×magnification, the dentine surface displayed obvious marks from the laser pulses, and the smear layer remained present between the laser pulses (Fig. 1 G2D). At higher magnifications (Fig 1 G2E and G2F) samples had a scaly appearance, with open dentinal tubules with clearly identifiable peritubular dentine.
For G3, the energy density of 18 J/cm2 was used for conditioning, and the laser pulse markings were still clearly visible, but the distance between them was smaller and the remnants of smear layer between the pulses could no longer be easily observed (Fig. 1 G3G). Rough irradiated surfaces were observed with open dentinal tubules, with clear peritubular dentine presence (Fig 1 G3H and G3I).
In the group irradiated with an energy density of 27 J/cm2 (G4), it was not possible to discern individual laser pulse marks (Fig. 2 G4J), indicating that the increase in energy produced a broader irradiated area; therefore, in this case, the broader pulse effects were in sufficient proximity to prevent the detection of an individual pulse. At higher magnifications (Fig. 2 G4K and G4L), the same irregular pattern of irradiated dentine, with open dentinal tubules, was observed.
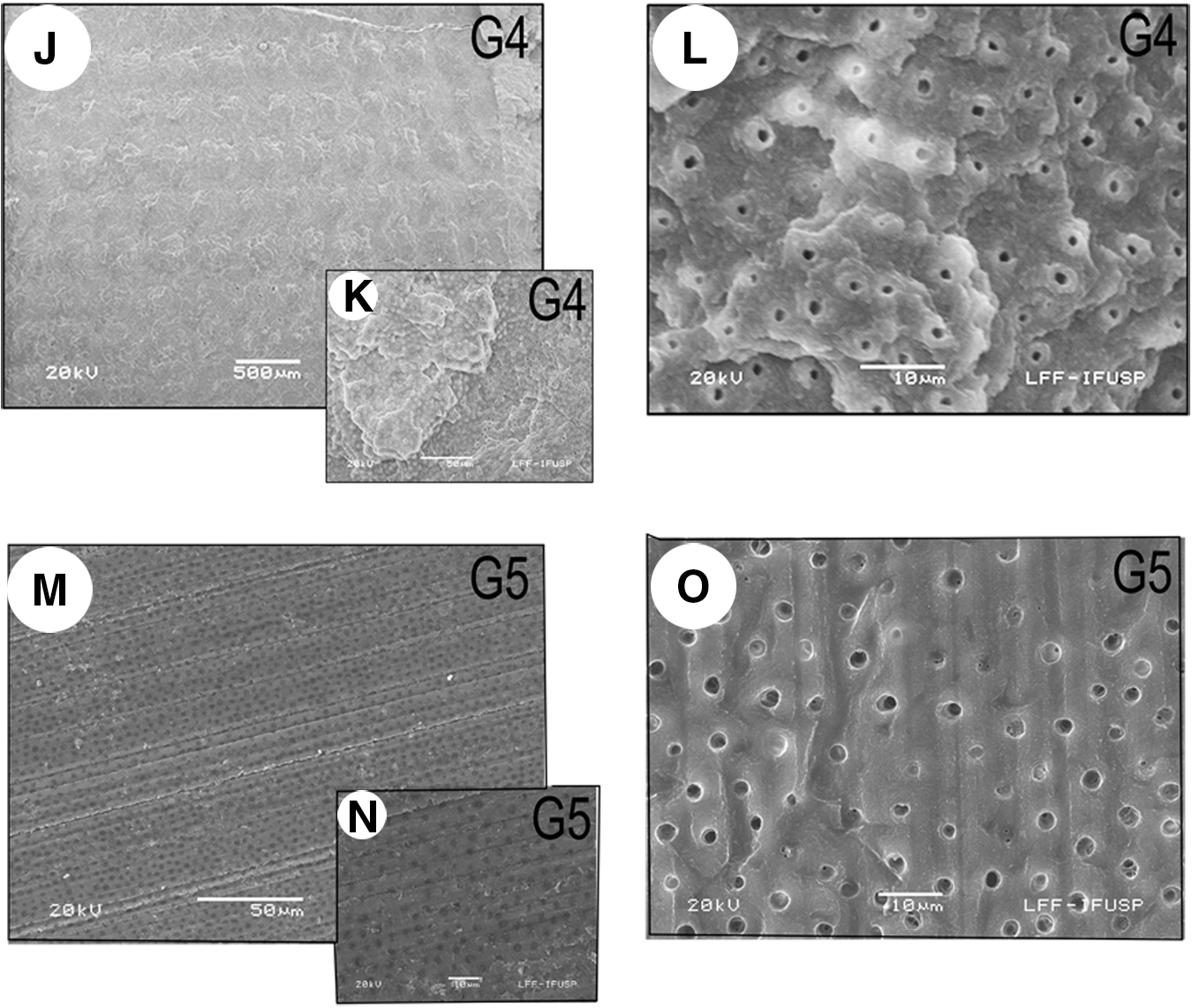
SEM micrographs of dentine surface conditioned with Er, Cr: YSGG laser with energy with energy density of 27 J/cm2, 1.5 W average power, 75 mJ/pulse (G4J–L); and dentinal conditioning with polyacrilic acid (G5M–O). In G4J (30×), the laser pulses are closer to each other and there is no smear layer between them, without a clear distinction of its pulse borders; in G4K (500×) the irradiated dentine is irregular, with open dentinal tubules; in G4L (2000×) peritubular dentine can be easily distinguished over the irradiated surface; in G5M (30×) a thin pattern smear layer can be observed on the entire surface; in G5N (500×) the dentinal surface is covered by a thin smear layer that enables detection of tubule apertures, but they seem to remain closed; and in G5O (2000×) in higher magnification, some open dentinal tubules are observed, but others remain closed.
As recommended by the manufacturer, G5 received dentinal conditioning with GIC liquid before sample construction. At lower magnifications, the location of dentinal tubules apertures could be easily detected, but they were closed (Fig. 2 G5M). On the other hand, at higher magnifications (Fig. 2 G5N and G5O), tubules were open in some areas and closed in others, indicating that acidic treatment was not efficient in removing the entire smear layer.
Micro-shear BS test
One way ANOVA indicated statistical difference among experimental groups (p<0.001). The expression G2>(G1=G5)>(G3=G4) is valid. The group with the highest value for BS was G2 (10.54±1.16 MPa), followed by G1 (4.79±0.82 MPa) and G5 (4.26±1.02 MPa), which were statistically similar, whereas there was no significant difference in BS values between G3 (3.73±0.53 MPa) and G4 (3.00±0.58 MPa), with these two groups presenting the lowest BS values observed in this study (Table 1).
Different letters indicate statistical difference.
Fracture pattern evaluation
After the staining of samples by immersion in 2% Ponceau S solution and the subsequent observation of the samples under the optical microscope, only adhesive and mixed fracture types were detected (Table 1). Is it important to point out that the high number of lost GIC tubes, recorded in the statistical analysis as 0 MPa, were observed in G3 and G4, indicating a very low BS resistance.
In the images obtained from laser-irradiated groups, an important difference was observed in the pigmentation of the pulsed area (Fig. 2). In G2, areas of irradiation pulses were more intensely stained by Ponceau S solution (Fig. 1A), whereas in G3 and G4, the pulse areas were not stained in red, but in white (Fig. 1B and C).
In the photomicrographs chosen to illustrate the fracture types, the adhesive fracture was captured at three magnifications (50×, 150×, and 600×), to ensure the precise visualization of the fracture. At 50×magnification (Fig. 3A), the area of the dentine on which GIC adhesion was performed was clearly visible. The specimen that was randomly chosen to illustrate this fracture type belonged to G3; therefore, at the same magnification, the locations of laser irradiation pulses could be identified. At higher magnifications, an irregular surface with open dentinal tubules was observed (Fig. 3B and C).

Images (20×magnification) of laser-irradiated dentine after immersion in 2% Ponceau S solution. Whereas in
The adhesion location for the mixed fracture specimen was easily identified at 50×magnification (Fig. 3D). As the randomly chosen specimen belonged to G2, equidistant laser pulses were also visible at 50×magnification. At both 50×and 150×magnifications, a smear layer and GIC remnants were observed (Fig. 4D).

Scanning electron microscopic (SEM) micrographs of the adhesive (
Discussion
The greatest challenge in the area of laser in dentistry, more precisely in dentin adhesion, is to identify an irradiation protocol that favors greater BS values between the substrate and the restorative material. The present study demonstrated that Er,Cr:YSGG laser conditioning with an average power of 0.5 W, 25 mJ per pulse, and an energy density of 9 J/cm2, significantly increased the BS values between conventional GIC and dentine. This result is unprecedented, as the currently available literature reports that for both cavity preparation and surface conditioning, Er,Cr:YSGG laser irradiation does not favor the adhesive procedure, but instead, decreases the adhesion between the GIC and the dental tissue. 6 –10,19
The superiority in BS provided by laser conditioning at 0.5 W and 9 J/cm2 suggests that this treatment not only preserves but most likely increases the ionic exchange between the dentine and the GIC. It has been previously observed that an erbium laser irradiation with low energy-density parameters, below the ablation threshold, increases the content of calcium, magnesium, sodium, and phosphate on tooth surfaces. 15 Authors 14 explain that conventional GIC adhesion to dentine occurs through the formation of an intermediary layer in which rapid ionic diffusion occurs: aluminum, silicon, fluoride, and strontium flow from the GIC to the dentine, whereas calcium and phosphorus flow from the dentine to the GIC.
In fact, the BS value of 10.54±1.16 MPa obtained in G2, which was twice as high as the BS values found for the other four groups, supports the above-described conjecture that laser conditioning increases the ionic exchange between the dentine and the GIC. It is important to point out that even polycrylic acid conditioning (G5) did not increase BS as expected; 8,10 however this result does not have a consensus in the literature. 20,21 This analysis, however, would not be complete without an assessment of the observed fracture patterns. Compared with other groups, G2 demonstrated the lowest percentage of adhesive fractures (48.9%) and the highest percentage of mixed fractures (46.7%), suggesting that the BS of GIC to dentine reached its highest level for this group, as micro-shear tests have determined that the GIC does not resist forces much higher than 10 MPa. 22
The literature consensus states that because the Er,Cr:YSGG laser has a higher affinity for hydroxyapatite and a lower dependence on water content than the Er:YAG laser, it will also have lower ablation power, particularly in the case of dentine. 23,24 Therefore, if the Er,Cr:YSGG laser is used at lower energy densities and an adequate water/air flow is used, the ablation process can be controlled to obtain the type of dentine surface desired. As the ablation threshold for dentine is 2.69 J/cm2,25 but the dentine suffers a reduction in its microhardness of at least 30%, if more than 33.9 J/cm2 of energy is applied to it, 24 using irradiation parameters with low energy densities appears to be the most appropriate method.
Another observation that makes us more confident of our results is the fact that the laser pulse locations demonstrated greater Ponceau S staining for the G2 group. As Ponceau S is a dye that has an affinity with organic compounds, the Er,Cr:YSGG laser irradiation parameters for G2 of 0.5 W and 9 J/cm2 must have removed the smear layer without altering the dentine's collagen matrix, as the dye was readily able to interact with and stain the irradiated dentine. However, in G3 and G4, higher irradiation parameters were used, and the laser pulse locations were not stained by Ponceau S when compared with other dentine areas, indicating that alteration of the dentine's collagen matrix had occurred.
Therefore, we are confident that the irradiation parameter of 0.5 W, 9 J/cm2, and 25 mJ/pulse for dentine conditioning by the Er,Cr:YSGG laser is able to increase the interaction of the irradiated substrate with conventional GIC. There is no previous report in the literature that tested these irradiation protocols.
Groups G3 and G4, which were irradiated with 1.0 W, 18 J/cm2, and 50 mJ/pulse of laser energy and 1.5 W, 27 J/cm2, and 75 mJ/pulse of laser energy, respectively, did not showed statistically significant differences when compared with each other. These groups demonstrated the lowest BS values and a high percentage of adhesive fractures and pre-test failures, indicating that the irradiation parameters for these groups do not provide appropriate dentine conditioning for conventional GIC restoration, as it induced structural alterations.
In addition, higher irradiation energies will cause the dissolution of hydroxyapatite crystals and produce lower carbonate content for the dentine, rendering the irradiated tissue more resistant to demineralization. 26 As a result, this irradiated tissue will be less susceptible to the action of the polyacrylic acid contained in the GIC liquid, thus impairing the GIC's interaction with the dentine. This reduced adhesion is also accompanied by a decrease in the bonding of polyacrylic acid to the carboxyl groups present in hydroxyapatite. 27
Another interesting consideration that helps to explain the low BS values found in G3 and G4 is the fact that any electrostatic forces of attraction between the collagen type I of the dentine and the polyacrylic acid of the GIC 28 will be reduced if this collagen is denatured during irradiation, compromising the BS in the highly irradiated groups. The presence of the denaturing process is demonstrated by the inability of the organic Ponceau S dye to stain the areas irradiated with G3 and G4 irradiation protocols, as this inability indicates the absence of intact organic content in the irradiated dentine.
Only two studies evaluating the effect of substrate conditioning by an Er,Cr:YSGG laser on the BS between GIC and dentine 8,10 are available in the literature. In the study by Jordehi et al., 8 dentine irradiation by an Er,Cr:YSGG laser at 1.0 W of power, 50 mJ/pulse, 65% air pressure, and 55% water pressure, significantly decreased the BS values of conventional GIC. These findings corroborate the results of the present study for the same irradiation protocol (G3). In contrast, another study 10 showed that irradiated groups demonstrated higher BS values than drilling groups. However, this article did not include the irradiation protocol that was used, thus preventing more direct comparisons.
It is important to note that in both of the mentioned studies, the test used to evaluate adhesion was a microtensile test, which involved a large percentage of cohesive-type fractures in the GIC. These results can interfere with the reliability of the data, as this fracture type occurs if the restorative material fails but the adhesive interface is preserved. Therefore, the BS values obtained by these earlier studies refer to the resistance of the restorative material rather than its capacity to adhere to the dental substrate.
For example, different wavelengths of laser can be used to produce different levels of absorption of the water present in the enamel and dentine of teeth 24 ; moreover, lasers of different wavelengths will produce microscopically varied topographies that may clinically interfere with the BS of the restorative material. In addition, small changes in the power and energy density parameters can produce changes in the dentine that range from slight surface alterations to the creation of an amorphous interface that is virtually inert concerning adhesive processes. 9,29
Our contribution to the laser knowledge is the establishment of an irradiation protocol that provides a dentine conditioning without affecting its organic structure, thus increasing the adhesion of conventional GIC to dentine.
Conclusions
The Er,Cr:YSGG laser irradiation treatment featuring at an energy density of 9 J/cm2, average power of 0.5 W, and 25 mJ/pulse, proved to be the most appropriate protocol for dentine surface conditioning before the use of conventional GIC.
Footnotes
Author Disclosure Statement
No competing financial interests exist.