
Abstract
Introduction
Various methods of circumcision are used commonly worldwide today. For adult males, the forceps-guided method, the dorsal-slit method, and the sleeve resection method are the three most widely used methods of circumcision, with the dorsal-slit used most widely worldwide. 4 Although all of these techniques produce a good long-term result, there is a continuing need to improve the safety and efficacy of the circumcision procedure. Circumcision using a CO2 laser is a relatively new technique. Although first reported by Aynaud et al. in 1995, 5 there are few data using this technique available currently in the literature. 5,6 Although use of the CO2 laser for circumcision appeared promising, to the best of our knowledge, no clinical comparative studies between CO2 circumcision and conventional procedures have as yet been reported in adults. Therefore, our study was designed and developed to evaluate the benefits of the use of a CO2 laser versus the conventional dorsal-slit procedure for circumcision in adults. Also in this study, we present our modified technique for circumcision using a CO2 laser.
Materials and Methods
Patients
The present study was a prospective, randomized, patient-blinded study comparing conventional dorsal-slit circumcision with the modified CO2 laser circumcision technique. The ethical committee of our hospital approved the trial before embarking on the study. Patients were recruited for circumcision with the indications of phimosis, recurrent balanoposthitis, and patient requests. Written consent was obtained from patients prior to participating in the study. Exclusion criteria include active genital infections, sexual transmitted diseases, anatomic abnormalities of the penis, and medical conditions contraindicating surgery and those needing emergent circumcision for problems, such as paraphimosis or trauma.
From June 2010 to October 2010, 300 patients >18 years of age were recruited for this study at the Department of Urology in the Navy General Hospital of People's Liberation Army. Immediately before circumcision, using computer generated, sequentially numbered, opaque sealed envelopes, participants were randomized to either the CO2 laser circumcision (laser group) or the conventional dorsal-slit procedure (conventional group). The exact method of this randomization was to accomplish a correct balance to ensure an equal number of patients in both groups. The patients remained unaware of which group they were in throughout the procedure, because their view of the operation was blocked by a drape. They remained unaware of the group until their follow-up appointment at 3 months. At that point, they were informed of the circumcision type they had undergone after they had completed all the required follow-up examinations and questionnaires.
Operative technique
All procedures were performed under a penile-ring regional block anesthesia using 1% lidocaine. Circumcision was performed by two fixed urologists (Yansheng Xu and Zhiwei Li) who were well trained and experienced with circumcision practices.
Laser group
We used a Multipulse CO2 laser (KingLaser Technology Co. Ltd, Changchun, China) with a wavelength of 10,600 nm at a continuous power setting of 15 W. The laser energy was delivered to the prepuce in a noncontact mode by using a delivery system consisting of a reusable optical fiber coupled to a straight handpiece that focused the light beam onto a spot with a diameter <0.3 mm. We performed the laser circumcision in the following steps:
Step 1
After confirming adequate anesthesia, the fat pad around the base of the penis was compressed firmly to the pubic symphysis, and the glans was pulled forward as much as possible. Then, an aluminum sheet that was made from a tin can (Fig. 1A) and wrapped with moistened gauze was placed around the penis with the distal margin at the level of the coronal sulcus (Fig. 1B). The size of the aluminum sheet was ∼2.5×8.0 cm.
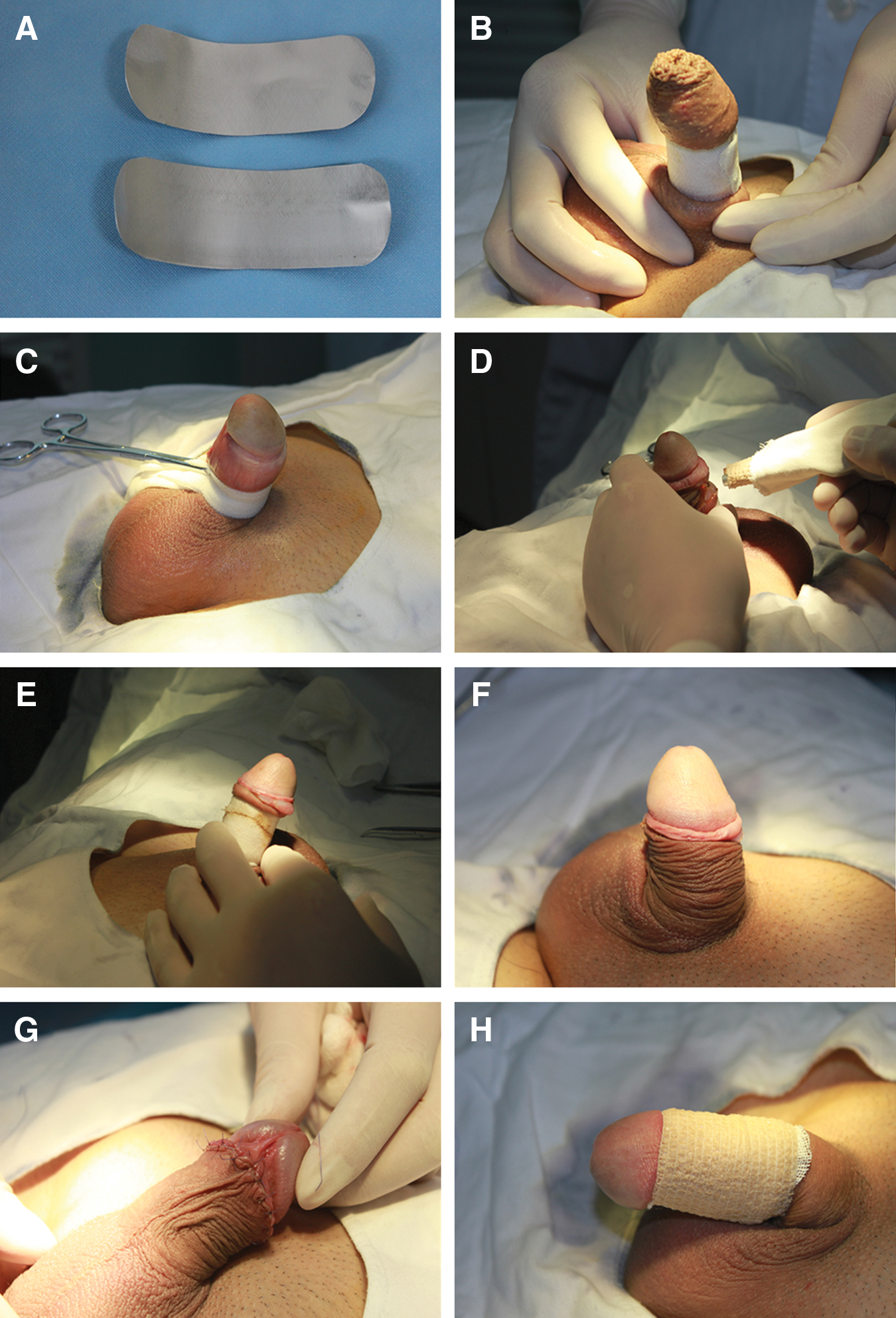
Surgical procedure for CO2 laser circumcision.
Step 2
The prepuce was everted completely over the gauze-covered aluminum sheet. The distal margin of the prepuce was marked and fixed by a piece of gauze and mosquito clamps (Fig. 1C). Adhesions between the glans and prepuce were removed bluntly. In patients with a true phimosis, a 1cm slit was made in the dorsal part of the prepuce before it was everted over the gauze-covered aluminum sheet.
Step 3
Beginning at the bottom of the frenulum, resection of the prepuce was performed with the CO2 laser with a noncontact technique, preserving a 0.5-cm-wide area of the preputial skin at the back of the penis and 1.0 cm at the bottom of the frenulum (Fig. 1D,E).
Step 4
After removal of the aluminum sheet, the occluded ends of the superficial dorsal vein were ligated using 4/0 absorbable sutures, and the cut edges of the skin and the preputial tissue were approximated with interrupted 4/0 absorbable sutures (Fig. 1F,G).
Step 5
The incision was covered by a vaseline gauze and wrapped moderately with an elastic bandage; this bandage was removed 24 h after the operation (Fig. 1H)
Conventional group
Using dissecting scissors and artery forceps, a conventional dorsal-slit method of circumcision was performed as described previously. 4,7 Monopolar electrocoagulation and ligatures were used for hemostasis. The cut edges of the skin and the preputial tissue were approximated with interrupted 4/0 absorbable sutures. Vaseline gauze and elastic bandages were also applied to cover the incision and removed 24 h after the operation.
Follow-up and data collection
The following parameters were recorded during the surgery: operating time and intraoperative blood loss. Operating time was defined as the time from when the patient was cleaned and draped until the last suture was placed. We recorded the blood loss by subtracting the dry weight of the gauzes from the blood-soaked weight of the gauzes.
After the operation, all patients were discharged to their homes on the same day. They received an oral antibiotic for 1 week to avoid infection. All the patients were advised to apply 0.5% Iodophor solution three times a day onto the operative site for 1 week after removal of the dressings, and to avoid intercourse and masturbation for 6 weeks after the procedure to prevent breakdown of the wound. The sutures were removed 7 days after operation. Follow-up of patients was performed by visiting the hospital at 1 day, 1 week, 2 weeks, 1 month, and 3 months postoperatively, and by phone calls at other times. In the follow-up, patients with any complaint at any time were encouraged to visit the hospital. As for pain assessment, participants were asked to rate their postoperative pain at 1 day and 7 days using a visual analogue scale (VAS) displaying numbers and words describing levels of pain from 0=no pain to 10=worst pain possible. Side effects were monitored closely during the postoperative period. In order to rule out the subjective bias, the people recording the intraoperative data, VAS score, and postoperative complications were blinded to the techniques.
Statistics
Univariate analyses of continuous variables were performed using Student t test. The χ2 and Fisher's exact test were used for univariate comparisons of categorical variables. SPSS 16.0 for Windows (SPSS, SPSS Inc., Chicago, IL) was utilized for the data analysis, and the significance level was set at 0.05 and all p values were two sided. Continuous data are presented as mean±standard deviations.
Results
Clinical data of the patients are displayed in Table 1. Patients in both groups had similar age distribution and indications for circumcision. The mean age of the patients in the laser and conventional groups was 26.9±7.5 and 26.4±8.7 years (p=0.957), respectively. Circumcision was performed for phimosis and recurrent balanoposthitis in the majority of patients. Comparison of the patients in the two groups demonstrated a 10 min decrease in the operative time in the laser-treated group (10.5±0.9 vs. 21.1±2.7 min, p<0.05). With respect to blood loss, there was almost no blood lost during the operation using the CO2 laser; whereas the mean blood loss was 7.2±1.5 g in the conventional group (p<0.05). The CO2 laser technique was associated with much less pain at both 1 day (2.9±1.9 vs. 4.9±2.5, p<0.05) and 7 days (1.2±0.5 vs. 1.9±1.3, p<0.05) postoperatively.
Data presented as mean±standard deviation.
p value of<0.05 was considered statistically significant.
The incidence of postoperative bleeding was 2.7%, and occurred only in the conventional group (four cases), within the 24 h after the removal of the wound dressing. These patients were treated conservatively with compressive management, and none required a second operation to control the hemorrhage. In the laser-treated group, wound dehiscence requiring re-suturing was observed in one patient after intercourse at 23 days postoperatively. No patients in the conventional group developed wound dehiscence. The incidence of postoperative edema was less in the laser group (2.0% vs. 8.0%, p<0.05), none of these patients required any further treatment, and the edema disappeared gradually within 2–4 weeks. The overall incidence of complications was less in the laser group (2.7% vs. 10.7%, p<0.05). No patients developed late complications, such as adhesion, secondary phimosis, buried penis, or scar. In both groups, follow-up visits demonstrated excellent cosmetic results, and no secondary operations were performed because of unacceptable appearance.
Discussion
Male circumcision is one of the oldest surgical procedures in practice today and is performed commonly in countries where infant circumcision is not routine. Although regarded as a simple and minor operation, circumcision, like any surgical procedure, does carry the risk of complications, which range from the insignificant to the tragic, including bleeding, infection, fistula, necrosis of the glans, buried penis, penile amputation, or even death. 8 –10
As with any operative procedure, bleeding is probably the most common complication of circumcision, 9 with an incidence that varies from 0.1% to 35%. 10 Bleeding may occur along the skin edges or from a discrete blood vessel, most commonly at the frenulum. Bleeding from larger blood vessels can be controlled easily by ligature or electrocoagulation. It is somewhat awkward to deal with the bleeding from the skin edges, where small vessels easily retract under the wound surface; direct pressure or electrocautery is usually applied on these occasions. Excessive electrocoagulation may expose the patients to the risk of electrical burns and necrosis, 11 whereas inadequate hemostasis gives rise to postoperative bleeding. In our study, the incidence of postoperative bleeding and intraoperative blood loss was significantly decreased in patients treated by the CO2 laser technique compared with those treated by a conventional method. These effects are attributed to the excellent hemostatic effect of the CO2 laser. Most energy from the CO2 laser can be absorbed by water, resulting in vaporization of intracellular and extracellular fluid, and carbonization. 12 At high-power density, small vessels can be cauterized, allowing for incision and coagulation at the same time during the resection of the redundant foreskin. Furthermore, less time is needed for hemostasis; the mean operative time was only ∼11 min in the laser group in our study, which was shorter by 10 min compared with that for patients who had circumcision by the conventional method.
Another advantage of the CO2 laser technique is the marked decrease in postoperative pain, which increased the comfort of the patients. Our study showed that patients treated with the CO2 laser had significantly less postoperative pain than did those who had had conventional surgery at both 1 day and 7 days postoperatively. This finding may be the result of the protein coagulum that forms on the wound surface in CO2 laser surgery acting as a biologic dressing that seals the ends of the sensory nerves. 13,14 Decreased postoperative pain in these patients might also be because they had less of an acute inflammatory response in the wounds created by the laser; 14 such inflammatory responses ordinarily cause postoperative pain by release of pain-inducing substances and increasing the responsiveness of the sensory system to these substances. 15
More cases of pronounced edema were observed among patients treated by the conventional technique than among the laser group in our study. This observation is presumably caused by the excessive thermal damage done to the preputial tissues by the electrocautery used for hemostasis in the conventional group. Thermal transmission to surrounding tissue by the CO2 laser is minimal, whereas the mean depth of damage produced by electrosurgery is much greater than that created by a CO2 laser. 16,17 In contrast to the sharply defined and limited necrosis after a CO2 laser, more extensive and irregular necrosis is found after electrocautery, resulting in a more severe inflammatory reaction than with the CO2 laser. 18 In addition, the CO2 laser can seal lymphatic vessels, which can minimize the leakage of lymphatic liquid into the tissue and its associated tissue swelling.
The only disadvantage associated with the use of CO2 laser observed in our present work is the possible delay of wound healing compared with the conventional method. Wound dehiscence was observed in one patient in the laser group, but the patient had had sexual intercourse at 23 days postoperatively, despite our admonition to avoid sexual intercourse for 6 weeks. Whether the CO2 laser technique led to delayed healing and predisposed to wound separation is unknown, because no other patient had problems with wound healing. It is possible that the thin layer of denatured collagen associated with laser wounds acts as an impermeable dressing that decreases initially the degree of tissue irritation; this delays inflammatory infiltrate migration and fibroblast formation. 13 Re-epithelialization and collagen conformation are shown to be delayed somewhat in CO2 laser wounds when compared with scalpel wounds. 13,19,20 Nevertheless, the regenerated dermal and epidermal thicknesses in the laser wounds were similar to those from scalpel wounds 6 weeks after incision. 20 Therefore, patients should be counseled extensively to avoid intercourse and masturbation for at least 6 weeks after undergoing circumcision by CO2 laser.
The incidence of postoperative complications in our study was much higher than what would be expected by most urologists. The principal reason is that the rate of complications depends upon multiple factors, including anatomic abnormalities, medical comorbidities, surgical technique, sterility of the conditions, and the patient's age. In addition, there is variation caused by methodological issues such as duration of follow-up, epidemiological study design, and definition of complications. 8 In most studies, edema is not regarded as a complication and is seldom included in the statistical analysis. If edema is excluded from the complications, the incidence of complications was 0.7% and 2.7% (p=0.176) in the laser-treated and the conventionally treated groups, respectively, in the present study, which was similar to that for previous series. 8,9 Therefore, when comparing our data with other reported series, we must keep this special circumstance in mind.
The CO2 laser may be applied widely for circumcision at the present time. Although few data are available, we speculate that the CO2 laser can be used as a replacement for scalpel or scissors when performing the forceps-guided, dorsal-slit or the sleeve resection circumcision. In our study, we performed laser circumcision in a modified version, which we believe offers several advantages. First, the prepuce is everted over an aluminum sheet that is wrapped by moistened gauze and used as a safeguard for the shaft of the penis; the glans and coronal sulcus are visible throughout the entire procedure (Fig. 1C) which minimizes the risk of injury to the glans penis and frenulum. In addition, under the protection of the aluminum sheet, injury to the corpus penis is avoided once the full thickness of the prepuce is cut by the high power CO2 laser beam (Fig. 1D). Second, after placing the aluminum sheet as described in Step 1, the exact amount of redundant prepuce can be confirmed easily (i.e., the part of the prepuce beyond the distal margin of the aluminum sheet, Fig. 1B). This avoids the risk of excessive or insufficient excision of foreskin. Excessive removal of foreskin leads to a spectrum of potential problems ranging from pain at the suture line at the time of erection to the “concealed penis syndrome”; 21 inadequate circumcision may result in secondary phimosis, fusion of the remaining foreskin with the glans, or an unsatisfactory cosmetic appearance. 22 Revisionary surgery may be necessary to correct these complications. In our study, follow-up visits demonstrated excellent cosmetic results after CO2 laser circumcision (Fig. 2). Third, with eversion and fixation as in Step 2, the prepuce is everted smoothly and neatly over the protective shield (Fig. 1C). The surgeon can make a rapid and continuous incision during the procedure, and the cut edges are smooth in contrast to edges cut by scissors.

Cosmetic outcome at 1 month post CO2 laser circumcision.
Conclusions
In summary, our study demonstrates that the CO2 laser is a safe and effective technique for circumcision in adult males. This technique provides excellent results with a decrease in operative time, less blood loss, and less postoperative morbidity compared with the conventional dorsal-slit method; the only potential disadvantage is a minor delay in wound healing. The modified technique we have introduced has proven to be easy and safe, and may be a useful alternative to the conventional surgical technique.
Footnotes
Author Disclosure Statement
No competing financial interests exist.