
Abstract
Introduction
E
Enterococcus faecalis is the most prevalent micro-organism involved in the pathogenicity of refractory endodontic infection in failed treatment cases. 6 This organism is a facultatively anaerobic gram-positive coccus, which can endure challenging environments, such as high alkaline pH (like that created by calcium hydroxide), desiccation, and high salt concentrations. 7 E. faecalis biofilm is a dynamic structure of bacterial community, which is embedded in polysaccharide matrix. 8 This organized structure provides resistance against antibacterial agents using three mechanisms: (1) failure of complete penetration into the biofilm, (2) cells that grow slowly because of nutritional limitations, and (3) adoption of the resistant phenotype. 9
By far, sodium hypochlorite (NaOCl) has been the most effective antibacterial irrigant with widespread use in endodontic treatment. This irrigant has been demonstrated to be a disinfecting agent with tissue-dissolving properties, being bactericidal with proteolytic effects. 10
Photodynamic therapy (PDT) is a biologically therapeutic modality using nontoxic photoactivable agents that are selectively localized in tissues and subsequently release reactive oxygen species by exposure to visible light, whereupon they become toxic against targeted cells and result in lethal photodestruction. 11 This method could kill bacteria organized in a biofilm and minimize the occurrence of bacterial resistance. 12
E. faecalis biofilm development is adjusted at three main stages: (1) attachment of bacteria and formation of microcolonies, (2) dissolution of mineralized dentin substrate and release of calcium and phosphate ions, and (3) progression of mineralization and calcification in biofilms. As the biofilm undergoes maturation within the root canal space, E. faecalis biofilm becomes calcified, resulting in persistent root canal infection. 13 Previous studies have shown formation of mature biofilm with signs of mineralization after 6 weeks of E. faecalis incubation. 14 This study aimed to investigate the bactericidal effect of PDT and NaOCl at three different stages of E. faecalis biofilm formation, including immature biofilm (4-week-old biofilm), mature biofilm (6-week-old biofilm) and old biofilm (8-week-old biofilm). In this study, different stages of biofilms were used to achieve an understanding about the relation between structural biofilm development and susceptibility to antibacterial treatment approaches.
Materials and Methods
Assuming that α=0.05, power=80% and σ/d=0.8, 120 samples were investigated in this in vitro study. A total of 120 human maxillary and mandibular central incisors that were extracted because of periodontal disease were used. Roots were fully developed, mature, straight, and without root caries or prior root canal treatment. Presence of one canal was confirmed using two radiographs (mesiodistal and buccolingual directions).
Endodontic Procedures
The teeth were stored in 0.5% chloramines T solution. All the calculi and periodontal tissues were removed with an ultrasonic device (Cavitron, Dentsply Ltd, Weybridge, UK). All the teeth were decoronated with diamond-coated discs (D&Z, Diamant, Germany) near th cementoenamel junction (CEJ) level to leave ∼12 mm of root length. The working lengths were measured using #15 K-files (Dentsply Maillefer, Ballaigues, Switzerland). Initially, the coronal two thirds of the canals were prepared with Gates-Glidden drills (Maillefer, Dentsply, Switzerland) with sizes varying from #4 to #1. Then the root canals were instrumented up to #60 K-file. Each canal was irrigated with physiologic serum during instrumentation using a 2 mL syringe and a 30 gauge needle. After instrumentation, 5.25% NaOCl solution was applied for 3 min; subsequently each root was immersed in 1 mL of 17% ethylenediaminetetraacetic acid (EDTA) for 3 min, followed by a final flush with phosphate-buffered saline (PBS). Aiming at exposing the dentinal surface, three teeth were sectioned longitudinally with a diamond disc for evaluation under a scanning electron microscope (SEM) (VEGA 2 Tescan, Cranberry, PA) (Figs. 1A and B and 2B).
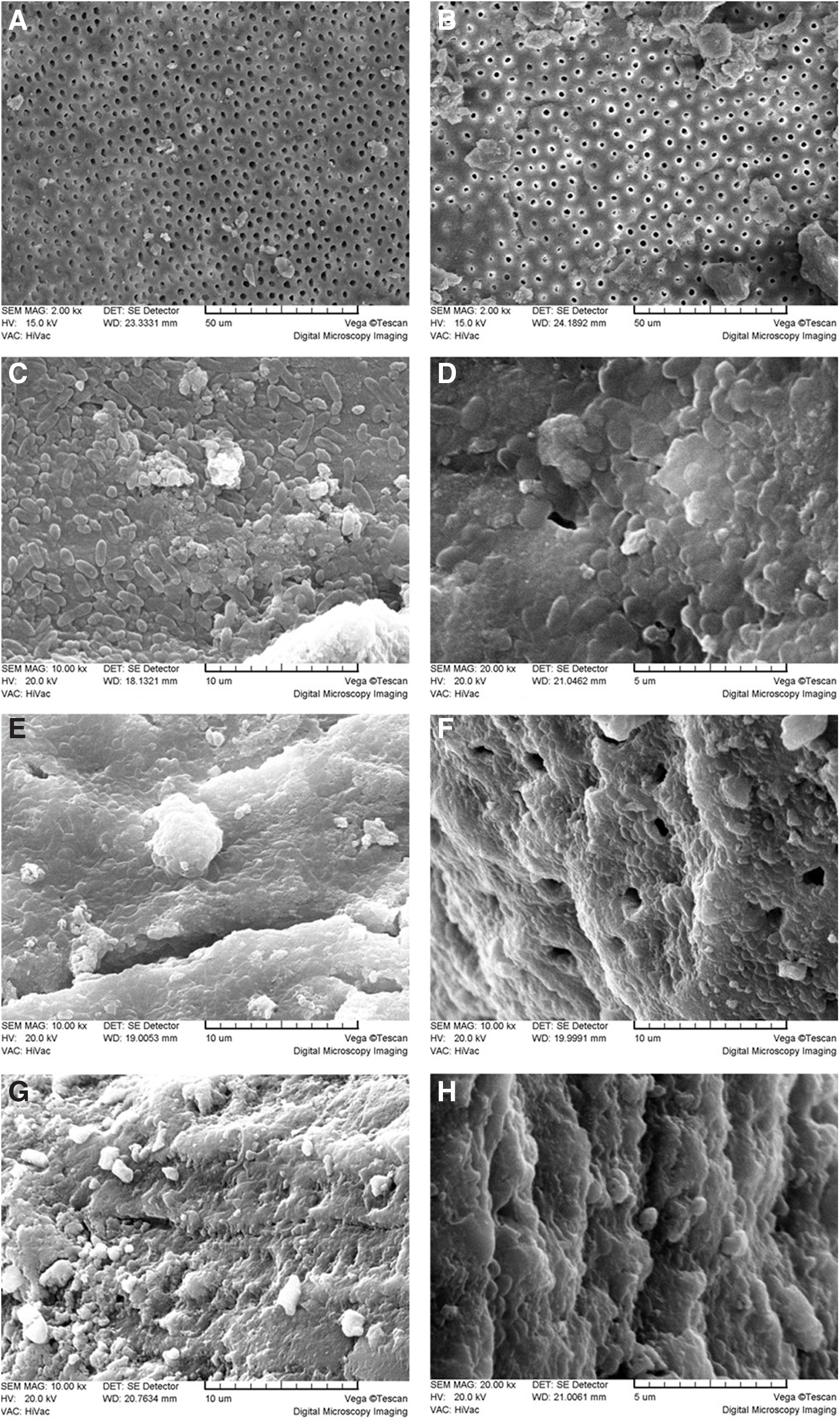
Scanning electron micrograph analysis of Enterococcus faecalis biofilm development on root canal dentine (
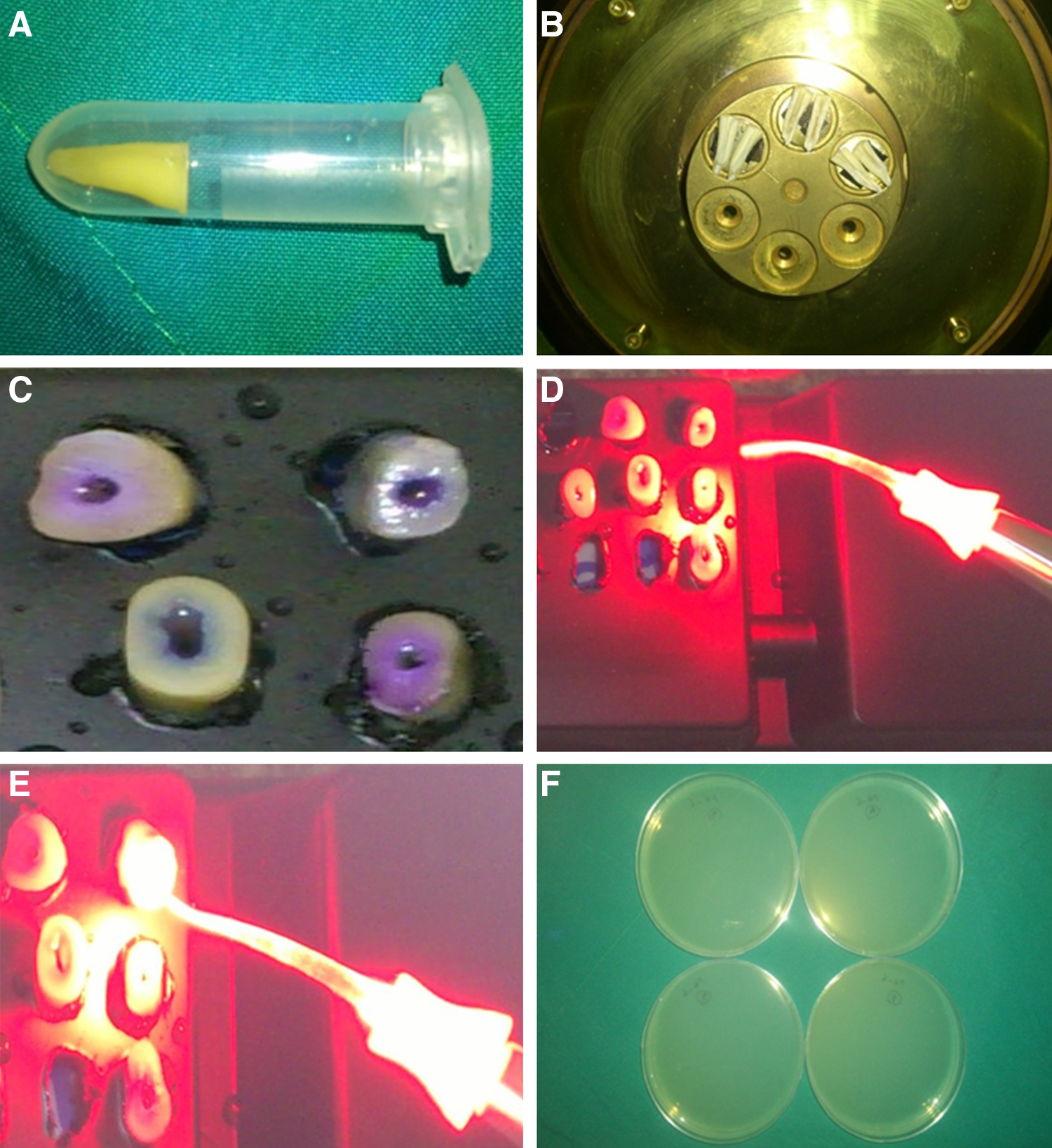
Photograph of experimental apparatus.
Microbiologic procedures
The samples were autoclaved at 121°C and 15 psi for 20 min, to kill all the organisms. Immediately, all the teeth were placed in brain-heart infusion broth (BHIB) (Merck, Darmstadt, Germany) at 37°C for 24 h to check the efficacy of the sterilization procedure. For the biofilm experiment, a pure culture of microorganisms was prepared in BHIB and incubated at 37°C overnight under 10% CO2. Then the bacteria were harvested by centrifugation and suspended. Cell counts were determined using a UV VISIBLE spectrophotometer at a wavelength of 600 nm; one optical density unit equals ∼108 cells/mL (equivalent to 0.5 McFarland solution). Then, each root was placed in a sterile tube which contained 2 mL of standard suspension of E. faecalis. Every other day, fresh nutrient was added to ensure the nutritional support and stability of the mediums, where the temperature was preserved at 37°C.
After 4, 6, and 8 weeks of biofilm growth, the roots were randomly selected and divided into four groups of 10 roots each, as described: Group I: phosphate-buffered saline Group II: photodynamic treatment Group III: 1% NaOCl Group IV: 2.5% NaOCl
Group I
The root canals were irrigated with 10 mL of PBS solution for 10 min.
Group II
In a dark room, the canals were filled with toluidine blue (TB) solution (25 μg/mL) at the level of the orifice using a Pro Rinse 30 gauge irrigation needle (Dentsply Tulsa Dental) for 5 min. The canals filled with TB dye were irradiated (Fig. 2C). Only fully developed and mature teeth with closed apex were used, in order to avoid dye draining.
For irradiation, a 625 nm diode laser was used (Fotoson CMS Dental, Denmark), with a fiber diameter of 200 μm, output power of 100 mW, power density of 1.4 W/cm2, spot size of 0.07 cm2, energy density of 214.28 J/cm2, and energy of 15 J for the 2.5 min of irradiation, in continuous mode. Light was applied for 2.5 min followed by a break of 2.5 min, and then a second light exposure was applied for 2.5 min, according to manufacturer's instructions, by means of a plastic and flexible optical fiber with cylindrical diffusers in order to distribute uniform light at 360o (Fig. 2D and E). The reason for the breaking period and the repeated irradiation is that free radicals would be reactivated, and subsequently they would become toxic against the remaining bacteria without destructive temperature enhancement. 15 This optical fiber with 200 μm diameter and a 0.03 taper could be inserted into the canals up to 3 mm short of the working length and could guide the light through the canal. Uniform cylindrical lighting using this tapered optical fiber increased the depth of penetration of light to inaccessible areas such as an isthmus, fins, and branching in the apical third (Fig. 2E).
Group III
The root canals were filled with NaOCl (1% v/v) for 10 min, removed with sterile paper points, and irrigated with normal saline solution.
Group IV
The root canals were filled with NaOCl (2.5% v/v) for 10 min, removed with sterile paper points, and irrigated with normal saline solution.
All groups
Subsequently, all the samples were placed in a refrigerator at −25°C overnight. The resulting precooling prevented E. faecalis killing because of drilling heat during the subsequent step. 16 After 24 h, a thin layer of internal root canal surfaces was removed using Gates-Glidden drills #5 and #6. Dentin chips were weighed using a sensitive electronic weighing machine (ASD Co., LTD, Japan) and 10 mg of dentin chips were weighed for each sample. Then, the chips were placed in sterile tubes, and 2 mL of physiologic serum was added to each tube and mixed for 20 sec. Ten tenfold serial dilutions were made up to a concentration of 10−7. At the next stage, 10 μL of each concentration was transferred to three Mueller-Hinton agar plates. The plates were then incubated at 37°C for 48 h. The number of colony forming units (CFUs) per millimeter was measured for the three plates with concentrations of 10−2, 10−3, and 10−4 (Fig. 2F).
After 4, 6, and 8 weeks of biofilm growth, three roots from each biofilm age group were selected for SEM evaluation in order to confirm biofilm formation. The teeth were sectioned longitudinally, and then dried for SEM imaging (Fig. 1 A–H). Statistical comparison of the means was calculated by using the Kruskal–Wallis test, and pairwise comparisons were conducted by Mann–Whitney U test, at a significance level of p<0.05.
Results
Kruskal–Wallis test revealed significant differences in bacterial counts between the four groups (p<0.001, df=3, χ2=84.85) and Mann–Whitney U test indicated no statistically significant differences between 2.5% NaOCl and PDT groups (p=1.000, Z=0.000), whereas other pairwise comparisons revealed statistically significant differences between the other groups at all the time intervals. The effects of PBS, PDT, and 2.5% and 1% NaOCl on decreasing E. faecalis counts at different stages of biofilm development are presented in Table 1, which depicts the means, medians, ranges, and standard deviations observed in all the groups. The treatment approach of groups II and IV achieved complete elimination of cell viability (100% bacterial killing). However, the 1% NaOCl (group III) exhibited 81.88%, 85.73%, and 78.62% reduction of bacterial counts at 4-, 6-, and 8- week biofilm growth intervals, respectively, in comparison with the PBS group (Table 1 and Fig. 3).

Effect of antibacterial approach against Enterococcus faecalis.
The same letters indicate no statistically significant differences among the groups.
PBS, phosphate-buffered saline; PDT, photodynamic therapy.
Discussion
Prevention of apical periodontitis is the principal goal of endodontic treatment. The microbiota of infected root canal play a fundamental role in apical periodontitis. Accordingly, reduction or elimination of the bacterial community of the root canal system may lead to improvement of treatment outcomes. 17
E. faecalis is the predominant microorganism detected in post-treatment apical periodontitis. This gram-positive coccid has various virulence factors that are responsible for resistance against antimicrobial agents. 18
Biofilm is composed of a glycocalyx matrix shielding the community with network channels in order to circulate nutrients through the biofilm structure. Eradication of sessile bacterial cells is up to 1000 times more difficult than their planktonic counterparts, because of the organized structure of the biofilm. 19
Shen et al. demonstrated that as the biofilm age increases, several changes occur in biofilm structure, influencing biofilm function physiologically. 20 Kishen et al.'s results showed that after 4 weeks of incubation, E. faecalis bacterial cells covered the whole dentin surface, and after 6 weeks, the mature biofilm exhibited a highly organized structure with signs of mineralization. 14 Accordingly, in the present study, from 6 weeks of incubation time onward, biofilms were considered to be mature with regard to their structural development. Previous results have shown that resistance of E. faecalis biofilms to antibacterial agents may be influenced by enhancement of incubation time (biofilm aging) and the physiological state of cells. 21,22 This study showed that bacterial counts after irrigation with 1% NaOCl in 6-week-old biofilm were 3.20-fold higher than in 4-week-old biofilm; in 8-week-old biofilm they were 5.94-fold higher than in 6-week-old biofilm, and in 8-week-old biofilms they were 19.08-fold higher than in 4-week-old biofilms. These results indicate that as the duration of incubation increases and biofilm undergoes maturation, elimination of bacteria becomes more difficult because of the calcified and highly organized structure of aging biofilms. In addition, mature biofilms provide a special environment for different metabolic activities of bacteria, which protects them against destructive agents (e.g., irrigants). During the incubation time from 6 weeks onward, carbonate and phosphate bonds of apatite at the surface of the biofilm are increased. Therefore, supersaturation of E. faecalis biofilms is seen. 14
Previous results have shown that NaOCl has a significant bactericidal effect on E. faecalis biofilm. 23,24 Radcliffe et al. showed that all the concentrations of NaOCl are effective on E. faecalis elimination, but at different times. 25 Gomes showed that 2.5% NaOCl with 10 min of exposure time can lead to complete killing of bacteria. 26 In this study, 1% NaOCl resulted in reduction of E. faecalis counts in comparison with the PBS group, in every three stages of development, whereas 2.5% NaOCl solution showed complete inhibition of growth of viable cells in three different stages of biofilm incubation.
Previous reports have indicated that PDT is an effective bactericidal agent in E. faecalis-contaminated root canals. Gram-positive bacteria (e.g., E. faecalis) are susceptible to PDT. It not only kills bacteria, but also may lead to detoxification of endotoxins, such as lipopolysaccharides, which stimulate the production of pro-inflammatory cytokines. Thus, PDT inactivates endotoxins by decreasing their biological activity. 27,28 Presence of microorganisms in inaccessible areas results in difficult delivery of antibacterial irrigants (e.g., NaOCl); however, PDT, using appropriate optic fibers, improves accessibility and penetration into the tubular network of the root canal system. Previous results have shown that antibacterial effectiveness of PDT depends upon duration of light exposure, photosensitizer concentration, photosensitizer absorbance, light energy, the introduction of an optic fiber into the canal, and light intensity. 29,30 In this study, special endodontic optic fibers with multiple cylindrical diffusers that uniformly distributed light at 360° were used for maximum penetration. Concentration of TB for endodontic purposes has been tested at ranges between 10 and 100 mg/mL, demonstrating that this range results in up to 100% killing of E. faecalis cells. 31,32 In the present study, according to manufacturer's instructions, 25 mg/mL concentration of TB was chosen. George and Kishen have shown that photosensitizer and light exposure combined with longer time of light exposure will lead to complete eradication of microorganisms. 32 In this study, the total duration of light exposure chosen was 5 min with a 2.5 min break between two exposures, according to manufacturer's instruction, in order to achieve complete bactericidal efficacy. In the present study, PDT resulted in complete eradication of E. faecalis (100% killing) in three different stages of biofilm incubation.
TBO is a cationic phenothiazine dye with high antibacterial efficacy. 33,34 Also, this photosensitizer has remarkably high affinity for polyphosphates, lipids, and membrane proteins; therefore, the bacterial cell membrane could be a critical target site for TBO-mediated photodestruction. 34,35 Usacheva indicated that both methylene blue (MB) and TB, eradicated all microorganisms (e.g., E. faecalis), but that complete inhibition was demonstrated at TB concentrations of 1.5– to 7-fold less than those of MB. TB exhibits a greater bactericidal efficacy than MB. 34 Another study showed that the ability to form dimers was greater for TB than for MB, and that the essential role of dimerization was bactericidal photodamage of dye. 36
The results of this study demonstrated that 2.5% NaOCl with 10 min contact time, and PDT with 5 min exposure time, can eradicate old and mature biofilm structures, whereas 1% NaOCl can lead to statistically significant reduction of CFUs but not to 100% killing. The results also showed that with an increase in the maturation of biofilms, efficacy of 1% NaOCl on biofilm eradication is decreased. Our results demonstrated that the effectiveness of NaOCl varies with contact time and concentration. The exposure time was the same in both groupings. A 1% concentration was not sufficient to kill all bacteria after 10 min. It probably needed more exposure time than the 2.5% NaOCl group, in which bacteria were completely eliminated after 10 min because of the increased bactericidal effect of the higher concentration. PDT also completely eradicated every stage of biofilm. This can be attributed to the production of free radicals and singlet oxygen. These toxic products can alter the local cell environment and result in reduced growth or bacterial death. In addition, using appropriate optic fibers, PDT improves accessibility and penetration into the tubular network when compared with the delivery of other disinfectant solutions.
However, no viable cells were detected with PDT or the 2.5% NaOCl approach, but more research is necessary to suggest new guidelines for resistance and treatment of refractory root canal infection. The results showed that bacteria in mature and old biofilms (≥6 weeks) were more resistant than cells in young biofilms to 1% NaOCl, and that overall survival and residual bacteria increase with biofilm aging. Nevertheless, there are not enough data and evidence to suggest that PDT is a more effective antimicrobial approach than traditional bactericidal agents. Furthermore, randomized long-term clinical studies and meta-analyses are necessary to prove the superior bactericidal efficacy of PDT.
Conclusions
The results showed that bacteria in mature and old biofilm (6 weeks and older) were more resistant than young biofilms to the 1% NaOCl solution. Overall survival and residual bacteria increase with biofilm aging. PDT and the 2.5% NaOCl solution were both more efficient in eradicating E. faecalis.
Footnotes
Author Disclosure Statement
No competing financial interests exist.