
Abstract
Introduction
D
The feasibility of applying Ilizarov's principles to various craniofacial deformities was not considered until several decades after his pioneering work in the peripheral skeleton. The earliest reports of craniofacial distraction osteogenesis were published in the early 1960s, when rapid expansion of the palate was performed in growing patients. In 1973, Snyder first described the Ilizarov technique to lengthen a surgical osteotomy of the canine mandible. In 1992, the first clinical results of craniofacial distraction osteogenesis were reported by McCarthy et al. 3 in a small series of patients with congenital mandible deformities.
The underlying principle of distraction osteogenesis is the mechanical induction of new bone between bony surfaces that are gradually distracted. Following surgery and insertion of the distraction device, a waiting period (the latency phase) is allowed to elapse during which bone healing is initiated at the bony gap. In this early period, periosteal integrity is restored, and callus formation begins. The bone segments at either end of the gap are then progressively distracted over a period of several days (the distraction phase) during which osteogenesis is induced, thus producing a so-called regenerate of immature bone laid down between the cut bone ends. Over time, the bone remodels into a more mature state (the consolidation phase), and the surrounding soft tissues adapt to their new positions and lengths. 1
Ossification occurs as the primary mineralization front advances from either end of the fibrous central zone, resulting in a bridge of immature bone across the distraction gap. Bone remodeling begins during the consolidation phase and continues over a period of 1–2 years, eventually transforming the regenerated bone into a mature osseous structure similar in size and shape to the adjacent bone.
Although the volume of the new bone is comparable with that of adjacent bones, animal studies show that its mineral content and radio density are ∼30% lower, as is the tensile strength of the regenerated segment. 2,3,4 –9
The longest of the five clinical periods in distraction osteogenesis is the consolidation period, 10 and the mechanism of bone formation during this period is unique. Although the distraction regenerate develops predominantly via membranous ossification, isolated islands of cartilage may also be observed, suggesting endochondral bone formation. 11 In addition, focal regions of chondrocytes surrounded by a mineralized matrix may be observed, suggesting a third type of bone formation, transchondroid, 12 –15 in which cartilage is formed, possibly because of decreased oxygen tension. 16
However, this cartilage is directly transformed into bone rather than by the traditionally accepted endochondral pathway. 17 A longer consolidation period increases the risk of device complications and functional and psychosocial problems for the patient. 17 Corcoran et al. 16 reported that 10 out of 29 devices used for mandibular distraction, including devices for costochondral reconstruction, caused complications during the treatment, including pin infection, transient numbness of the lower lip, hardware failure, hypertrophic scar, and fibrous malunion. Accelerating the process of bone regeneration and ossification would reduce the duration of treatment by distraction osteogenesis and thus reduce the associated risks.
Low-level laser therapy (LLLT) is a modality of clinical treatment that results in nonthermal effects on the treated tissues, and its biological effects cannot be attributed to heating. The magnitude of the effects depends upon the physiologic status of the cells or the clinical stage of the condition before irradiation. Therefore, positive photobiomodulation (PBM) may not always be detectable. 18 –25
A unique parameter responsible for photobiological responses has not been identified, but combinations of several parameters and their interaction appear to play a role. It remains uncertain whether bone stimulation by laser light is a general effect or whether the isolated stimulation of cells is possible.
The results of our studies and others indicate that bone irradiated mostly with infrared (IR) wavelengths shows increased osteoblastic proliferation, collagen deposition, and bone neoformation when compared with unirradiated bone. Repeated irradiation is necessary to maintain the process; a single dose is insufficient. Three to four sessions per week for 2 weeks are recommended. 18 –25
It has been suggested that irradiation can biostimulate undifferentiated mesenchymal cells to differentiate into osteoblasts and osteocytes. 18 –25 We were unable to find previous investigations on the effect of LLLT on new bone formation during mandibular lengthening by distraction osteogenesis. A possible positive response of the association of LLLT with distraction osteogenesis may translate into the acceleration of the bone regeneration and ossification process, allowing for earlier removal of the distraction device, and, therefore, reducing treatment time, increasing patient acceptance, and reducing the occurrence of problems associated with treatment. The aim of the present study was to devise an experimental animal model to evaluate the effect of LLLT on quality and timing of bone regeneration and ossification on distraction osteogenesis.
Materials and Methods
Eighteen healthy male white New Zealand rabbits weighing 2000–2700 g were used for this study. The animals were divided into two groups: a study group (with laser stimulation), and a control group (without laser stimulation). This study was approved by the Medical Ethics Committee of the Isfahan University of Medical Sciences (permit No. 384212).
After the animals received intraperitoneal sedation with ketamine (10 mg/kg, Darupakhsh, Tehran, Iran) and intramuscular cefazolin antibiotic prophylaxis (10 mg/kg, Darupakhsh, Tehran, Iran), local anesthesia with 2.0% lidocaine and 1:100,000 epinephrine and Rompum® (2 mg/kg, Darupakhsh, Tehran, Iran) as a sedative, a longitudinal, full-thickness incision was made along the inferior border of the left mandible, beginning from 2 cm behind the lower incisor and extending to the posterior, just anterior to the masseter muscle, to avoid damage to the facial artery. After subperiosteal dissection and the identification of the mental neurovascular bundle, we chose to insert the anterior and posterior pins before corticotomy to prevent cortical weakening and fracture during pin insertion. The pins were inserted parallel to and 5 mm away from the proposed corticotomy line in the inferior border; a corticotomy was then performed in the lateral cortex, just anterior to the first premolar to prevent injury to the lower incisor root. The same corticotomy line was performed through a periosteal pocket in the medial cortex. We attempted to protect the inferior alveolar and mental neurovascular bundles and minimize subperiosteal dissection for a better vascularization of the distraction site. After the completion of device insertion and suturing, the first dose of GaAlAs (λ: 810 nm; power (P) 200 mW) laser light was administered to the study group, directed at a right angle to the surgical site, medially and laterally at two points. The practitioners wore safety glasses and other protection. The laser beam [λ: 810 nm; P, 200 mW; irradiation mode, continuous wave (CW), energy density (ED):3 J/cm2; time, 7.5 sec; power density (PD), 400 mW/cm2, energy (E), 1.5 J, and spot diameter:0.8mm] (THOR Photomedicine Ltd) was delivered at every other day for 14 days. We used power meter 5000 W-LP (OPHIR, Israel) and Joule meter LA300W-LP (OPHIR, Israel) to measure the actual power and energy of the laser, respectively. The control group received no laser treatment. The defects were allowed to heal for 5 days while the distraction devices remained passive (the latency period), and then the lengthening was started at a rate of 0.5 mm/day.
The device was designed and fabricated by the authors to match the anatomy of the mandibles of the animals and activated over 10 days (the distraction period). The devices were then left inactivated (the consolidation period), and three animals from each group were euthanized at 10, 20, and 40 days after the consolidation period (Fig. 1).

Experimental protocol for distraction osteogenesis, laser exposure, and euthanasia, 228×61 mm (300×300 DPI).
The animals were euthanized by the vital perfusion method, 26 and each specimen was divided into two pieces, one for light microscopy analysis and the other for SEM analysis. The specimens for SEM analysis were held in a desiccator for 24 h before assessment. The SEM specimens were placed on an aluminum sheet in a Ball-tec coater for gold coating. The light microscopy specimens were prepared by the hematoxylin and eosin (H&E) staining method. The number of fibroblasts and the amount of collagen fiber and the number of ossification centers were used as criteria to rank the SEM images. For the ranking of the histological analysis results, the amount and orientation of collagen fibers and the amount of woven and lamellar bone were considered (Tables 1 and 2). The Mann–Whitney test was used for the biostatistical analysis. The examiner blindly evaluated the specimens and SEM pictures, and statistical significance was defined at p≤0.05).
Results
Macroscopic analysis
On gross examination of the distraction site, there were no differences in color, texture, and surface between the regenerates in the study and control groups.
SEM analysis
In the first phase of euthanasia (the 10th day of consolidation), mostly in the center of distracted area, dense collagenous networks were observed in the study group (Fig. 2), whereas in the control group, the active fibroblasts predominated, and much less collagen fiber was produced (p≤0.05) (Fig. 3).
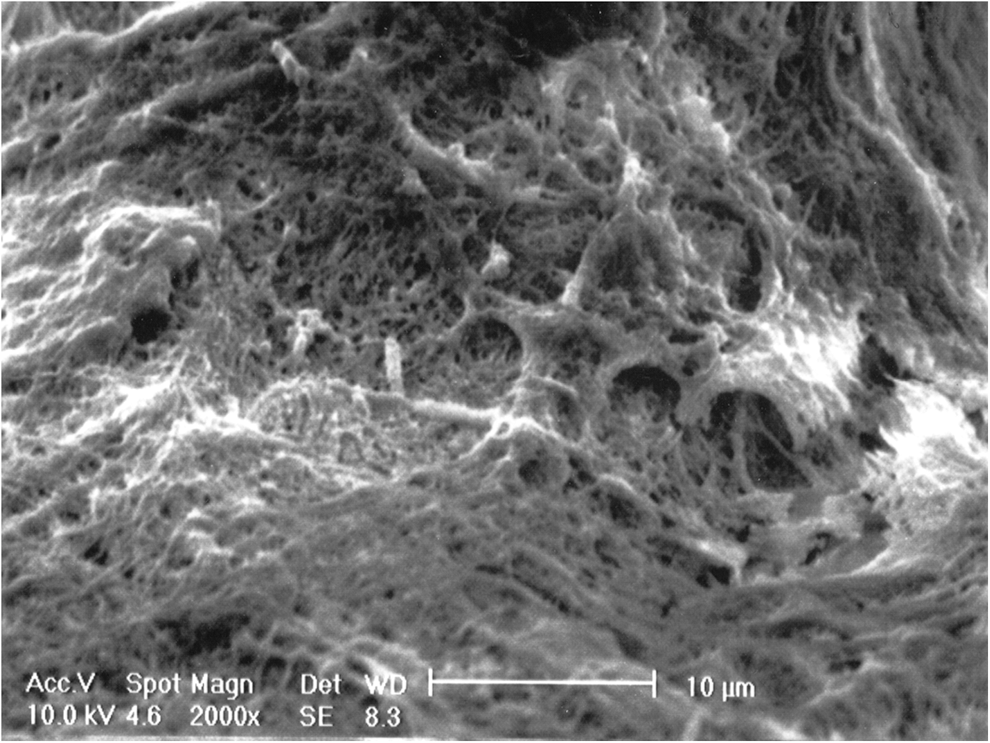
Scanning electron microscopic (SEM) view on the 10th day of the consolidation period (case group). Note the dense collagenous network, 89×67 mm (300×300 DPI).
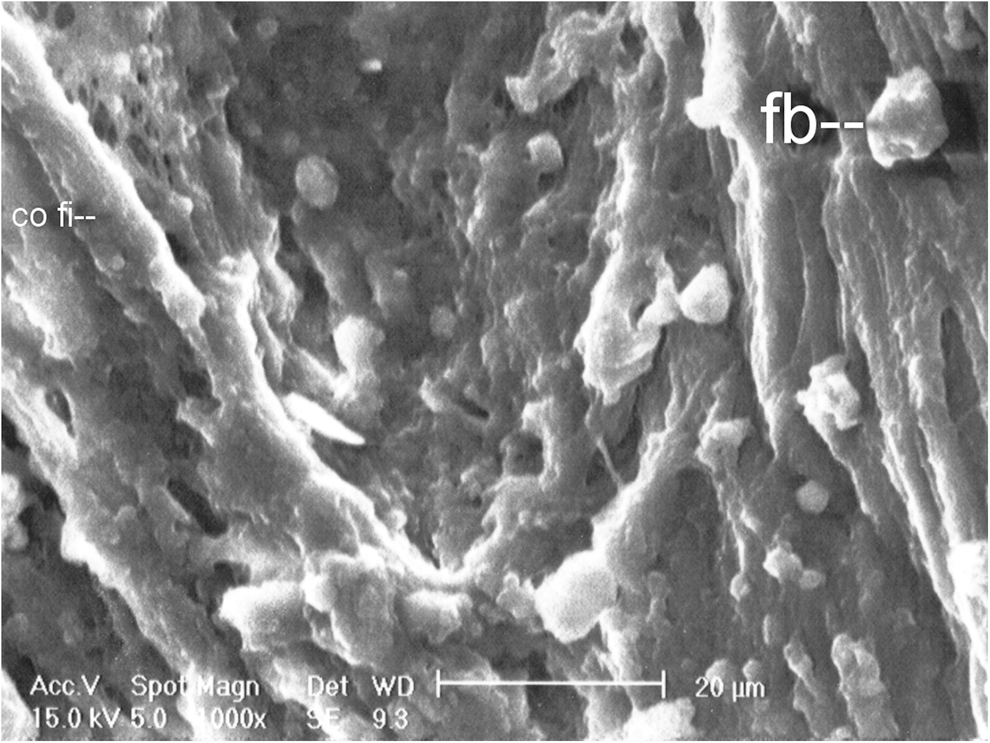
Scanning electron microscopic (SEM) view on the 10th day of the consolidation period (control group). Note the fibroblasts (Fb) on the collagenous network (collagen fibers: [co fi]), 88×66 mm (300×300 DPI).
In the second phase of euthanasia (the 20th day of consolidation), there were multiple ossification centers forming on the collagenous framework.
The centers in the study group were more developed than those in the control group (p≤0.05) (Figs. 4 and 5).
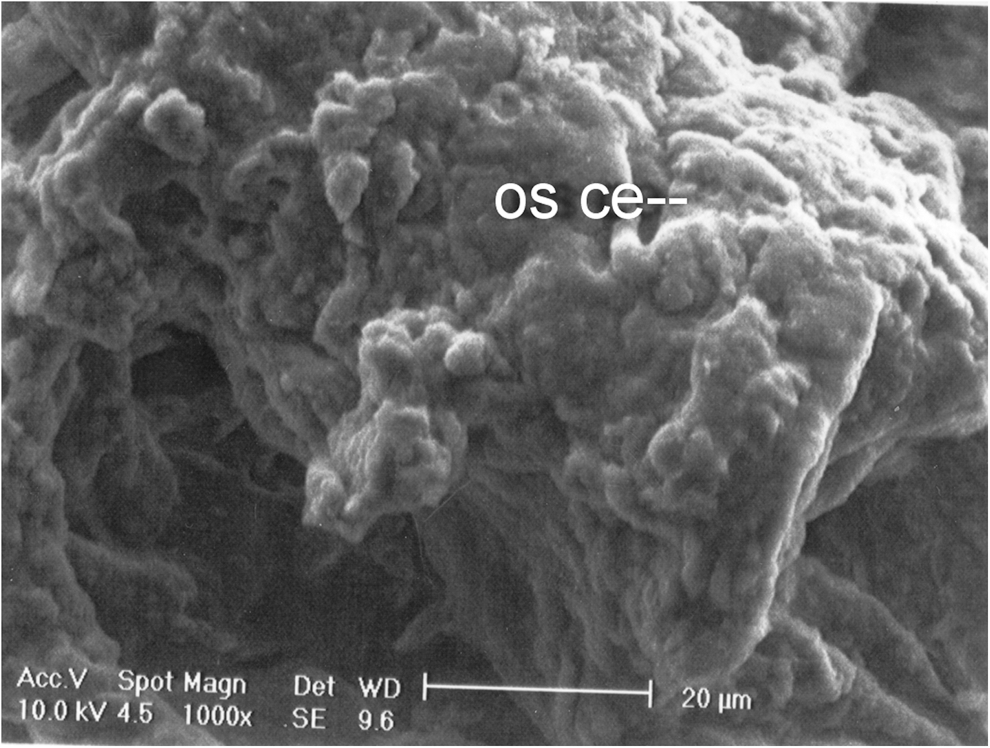
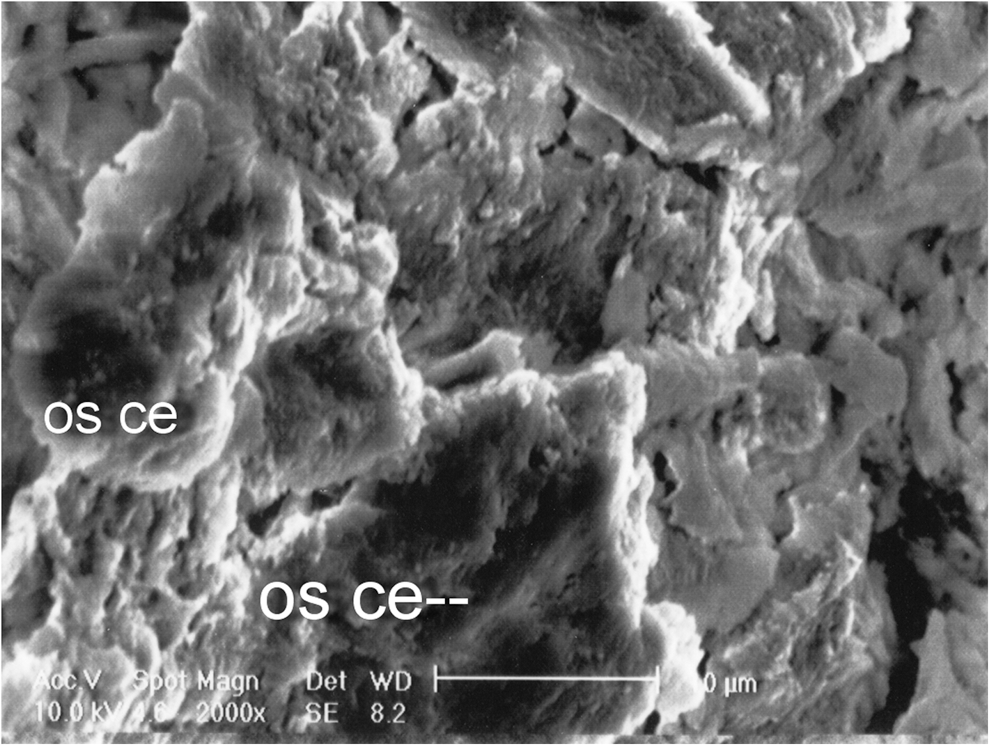
Scanning electron microscopic (SEM) view on the 20th day of the consolidation period. Note the ossification centers (os ce) on the collagenous network, 89×67 mm (300×300 DPI).
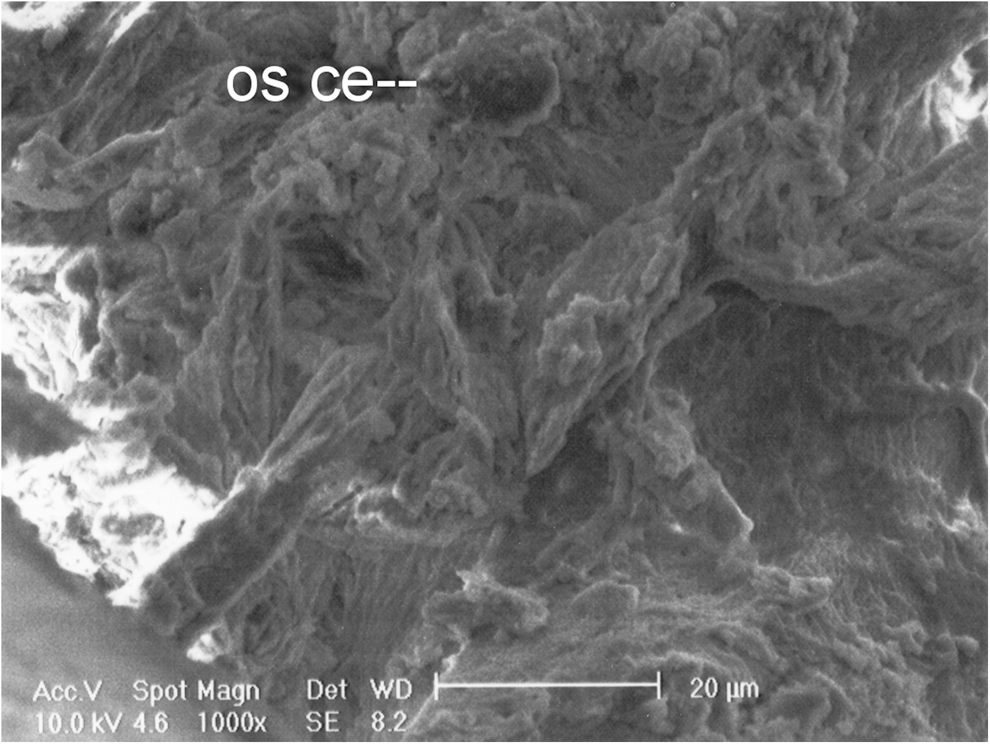
Scanning electron microscopic (SEM) view on the 20th day of the consolidation period (control group). Ossification centers (os ce), 90×67 mm (300×300 DPI)
In the third phase of euthaniasia (the 40th day of consolidation), there were no significant differences between the study and control groups. Gross ossification centers were observed, and the cells were embedded in the collagenous framework (Figs. 6 and 7).
Scanning electron microscopic (SEM) view on the 40th day of the consolidation period (case group). Ossification centers (os ce), 90×68 mm (300×300 DPI)
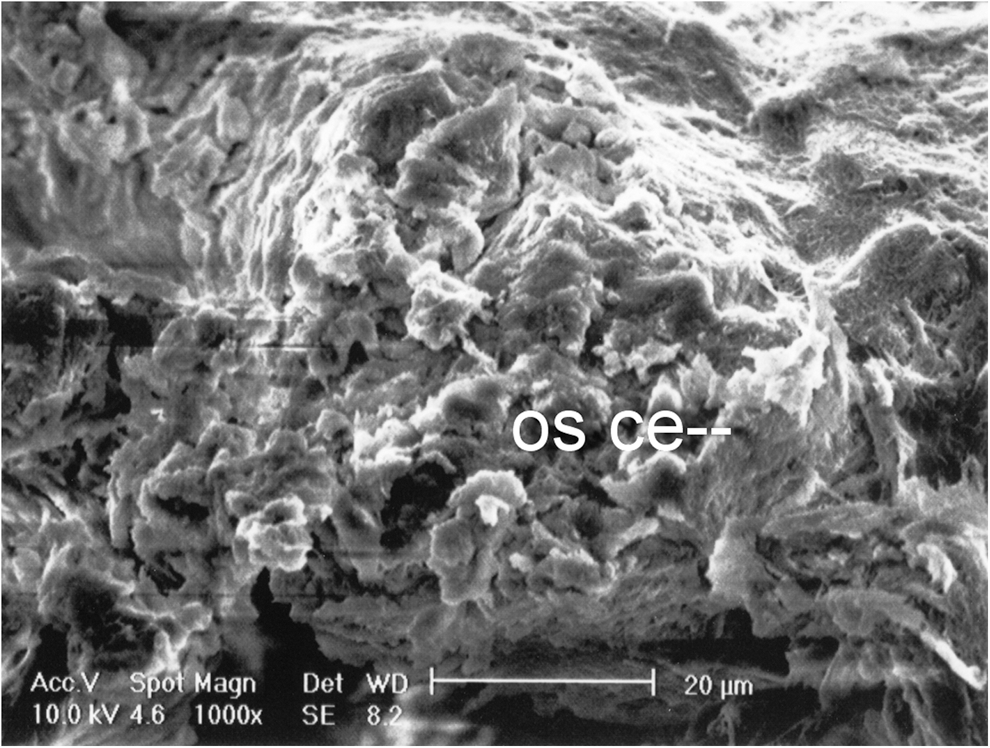
Scanning electron microscopic (SEM) view of the 40th day of the consolidation period (control group). Ossification centers (os ce), 90×68 mm (300×300 DPI)
Histological analysis
On the 10th day, mostly in the center of the study, the experimental group showed several well-oriented collagen fibers parallel to the distraction vector, and the fiber-to-cell ratio was very high, whereas in the control group, the fiber-to-cell ratio was very low, and the orientation and parallelism of the collagen fibers was less prominent than in the study group. On the 20th day, the fiber pattern had changed to hyaline cartilage in the study group, and a small amount of woven bone was observed at the periphery, whereas in the control group, the dominant feature was still the presence of collagenous tissue with a small amount of woven bone. At the end of the experimental time, lamellar bone dominated in both groups, with a small amount of woven bone, but there was no significant difference between the groups.
After statistical analysis, the results showed that the histological and SEM examinations yielded parallel and identical results. The mean rank of the first phase of euthanasia (the 10th day of consolidation) showed significant improvement of the bone formation process in the study group compared with the control group, in both histological and SEM examinations (p≤0.043), (p≤0.05) (Table 2). In the second phase (the 20th day of consolidation), significant improvement was observed (p≤0.05, p≤0.05), but the difference in mean rank between the study and control groups was decreased compared with that in the first phase (Table 2). In the third phase (the 40th day of consolidation), there were no significant differences between the two groups in either the histological or SEM examinations (p<0.340, p<0.317) (Table 2). These results indicate that GaAlAs (λ : 810 nm) laser at a power of 200 mW and a density of 3 J/cm2 accelerates new bone formation in the early consolidation period, but has no significant effect in later stages.
Discussion
The effects of therapeutic lasers on bone healing have been discussed many times in the literature. In contrast to bone healing after a fracture, in which the bone segments are fixed together at the fracture site to encourage anatomical healing, distraction osteogenesis is a dynamic process, and the mechanism of bone healing may be different with this technique. This treatment is time consuming and causes much discomfort for the patients. Reducing the treatment time would be very helpful in making this technique more popular. There are little data in the literature addressing the effects of laser irradiation on bone healing during distraction osteogenesis. Because there was no suitable distraction device available for animal use, we fabricated a device for use in this study by altering a common dental instrument (Fig. 1).
We combined SEM and histological modalities for a more accurate analysis of whether the changes at the molecular level paralleled those at the cellular level or there was a delay. The results confirmed the simultaneous occurrence of molecular and cellular changes. LLLTs are typically dose dependent, and differences between the study and control groups in our study might have been more significant in the later stages if we had continued laser delivery to the surgery site, although significant bone formation in early stages of this investigation can decrease the complications of distraction osteogenesis., such as fibrous union, infection, and device loosening, which usually occur early during distraction osteogenesis treatment.
There are conflicting reports in the literature concerning the effects of low-level lasers on bone formation. Nagasawa et al., 18 Yamada et al., 27 Trelles et al., 28 Luger et al., 29 Lomnitskiĭ et al., 30 Horowitz et al., 31 Ozawa et al., 32 Ueda et al., 33 and Yaakobi et al. 34 reported significant and positive effects of low-level lasers on the process of bone formation and repair, but Gorjestani et al. 35 and David et al. 36 did not report positive results.
Other investigators such as Lizarelli et al. 37 and Satio et al. 38 claim that low-level lasers can be useful in the early stages of bone formation, but are not effective in later stages. The results of this study are similar to those of Satio et al. and Lizarelli et al., which may be the result of redox regulation phenomena in the cells exposed to laser light.
Redox (reduction-oxidation) mechanisms control many biochemical reactions in living cells. 39
Increasing evidence suggests that living cells are more sensitive to in the oxidative state. In the postoperative period, several intercellular mediators secreted by cells cause inflammation and the production of free radicals; consequently, the pH is reduced. These processes may shift as a result of external stimuli, such as laser irradiation, possibly resulting in differentiation and mitosis. In later stages, when the inflammation has subsided and chemical mediators have been washed out, the pH returns to its normal value, and the redox equilibrium is balanced, which is a more stable cellular position and a less sensitive state to external stimuli. In our study, the first doses of laser light were directed only postoperatively; therefore, the mesenchymal cells are likely more stable and less sensitive to laser light.
There are several other theories regarding the mechanisms of LLLT on bone healing in the literature.
Several investigators have suggested that the transcription of certain nuclear proteins, such as rhodopsin-kinase, may be photosensitive at certain wavelengths, which may be responsible for the accelerated healing capabilities of LLLT. 40 Others have hypothesized that the nuclear factor kappa-B (NF-κB), a transcription factor, helps to induce the transcription of certain genes, and as a result, the LLLT-treated hard and soft tissues allow transcription of NF-κB in the nucleus to exert its effect on tissue protein repair elements. 40
Fujimato and colleagues suggested that low-level laser irradiation stimulates in vitro mineralization via increased expression of bone morphogenic protein (BMP) and transcription factors associated with osteoblast differentiation, 41 whereas Shimizu believes that the stimulatory effect of bone formation is at least partly mediated by the expression of insulin growth factor 1 (IGF-1); 42 moreover, Kiyosaki found that increased IGF-1 and BMP production is mediated by runt-related transcription factor 2 (RUNX2) gene expression and phosphorylation in osteoblasts. 43
Another study reported that low-level laser irradiation may enhance DNA replication and play a role in stimulating the proliferation of osteoblasts through the enhancement of minichromosome maintenance complex component 3 (MCM3) gene expression. 44
Other investigators found increased expression of the osteoglycin gene (1.2- to 2-fold higher) at 2–4 h after LLLT compared with the unirradiated control cells in the early proliferation stage of osteoblastic cells. The authors concluded that this increased expression may play an important role in the stimulation of bone formation in concert with matrix proteins and growth factors. This conclusion may also explain the significant effect of low-level laser irradiation in the present study during the early phases rather than in the late phases. 45 Although some other investigators, such as Kan et al., 46 reported similar results as our study because the optimal doses, intensities, treatment intervals and wavelengths for various indications remain clear, and the distraction protocol (latency period, rate, rhythm, and strain) can alter the process of bone formation per se, it is obvious that other experimental models should be designed to determine the optimal distraction protocol and laser exposure protocol for best results in this field. There are other modalities that may be used to improve distraction osteogenesis treatment, such as the transplantation of progenitor cells and the administration of growth factors or platelet rich plasma (PRP), but there is no consensus protocol, and these modalities require further investigation.
Conclusions
The results of the present study indicate that a GaAlAs (λ: 810 nm) laser at a P of 200 mW, ED of 3 J/cm2,irradiance of 400mW/cm2, T of 7.5 sec, promotes new bone formation only in the early stages of the consolidation period, and has no significant effects in later stages.
Footnotes
Author Disclosure Statement
No competing financial interests exist.