
Abstract
Introduction
I
It has been shown that a smear layer forms on the dentinal walls during root canal preparation 3 , and that this layer consists of organic and inorganic particles of dentin, remnants of pulp tissue, microorganisms, endotoxins, and blood cells. 4 This smear layer inhibits penetration of antimicrobial irrigants and medications into dentinal tubules, increases microleakage, and prevents sealer from adhering to dentinal walls. 5
Ethylenediaminetetraaceticacid (EDTA) is commonly used to remove the smear layer because of its capacity to act as a calcium chelating agent. 6 Studies have confirmed that a final rinse with 17% EDTA followed by sodium hypochlorite (NaOCl) may be effective in smear layer removal. 7,8
Additionally, various types of lasers, especially the infrared erbium-doped yttrium aluminium garnet (Er:YAG) and erbium, chromium: yttrium-scandium-gallium-garnet (Er,Cr:YSGG) lasers have been used in endodontics to promote root canal disinfection and the removal of the smear layer. 9,10 The mechanism of action of these erbium lasers is photoablation. During irradiation, the water content of the dentinal hard tissues evaporates immediately, and consequently, the laser irradiation ablates the surrounding tissues while causing only negligible thermal side effects. 11 A comparison between the two aforementioned lasers reveals that the Er:YAG laser utilizes a wavelength of 2.94 μm, which is absorbed by water, while the Er,Cr:YSGG laser utilizes a wavelength of 2.78 μm, which is absorbed by hydroxyapatite. 12
The Er,Cr:YSGG laser has specifically designed tips for endodontic use called “radial firing tips” (RFTs). These RFTs are flexible, 270 and 320 μm in diameter, and can be inserted up to working length. The tips have proven to be more effective for smear layer removal because of the dramatic cavitation effects they produce on canal walls. 13 Because of the 60 degree cone angle at the end of the radial firing tips, the irradiation from the laser effectively reaches homogeneous portions of the root canal as a whole. 14 Studies have shown that these tips are not hazardous to periapical tissues, 15 and improve the light irradiation inside root canals. 15,16
In order to achieve an optimal seal between root canal fillings and canal walls, the bond strength of the filling material to dentin should be as high as possible. 17 The development of the Resilon® urethane dimethacrylate (UDMA)-based root filling system has offered many advantages over conventional root canal fillings with gutta-percha. 18 A stronger bond between root filling and canal wall is produced with the aid of this system, the result of which is reduced apical leakage, likely increased fracture resistance, and improved clinical longevity of root-filled teeth. 17,19,20
RealSeal is a dual-curing methacrylate resin-based sealer in which the resin matrix consists of bisphenol-A-glycidyl methacrylate (BisGMA), ethoxylated BisGMA, UDMA, and hydrophilic difunctional methacrylate. The sealer bonds to core material and dentin using a primer. 20 Recently, the RealSeal Self-Etch (SE) system (SybronEndo Corp., Orange, CA) was developed. The primer component of the sealer has been eliminated, which allows for the creation of a resolute initial bond to the dentinal walls of the root canal. The system is composed of two components: RealSeal SE sealer and core material (Resilon). 21 Recent studies have shown higher push-out bond strengths for RealSeal SE than with other non-etching sealers. 21 In addition, the Resilon/RealSeal obturation system showed acceptable push-out bond strength when used with new polymeric endodontic obturation systems. 17 Two separate studies effectively showed higher fracture resistance of teeth obturated with the Resilon/RealSeal system than of teeth obturated with gutta-percha/zinc oxide eugenol, gutta-percha/AH26, or gutta-percha/AH plus. 20,22
Considering the effects of the Er,Cr:YSGG laser on smear layer removal and the potential effects on bond strength of resin-based sealers, the aim of the present study was to evaluate the effect of Er,Cr:YSGG laser irradiation on the push-out bond strength of Resilon/RealSeal SE sealer compared with a treatment using 17% EDTA+5.25% NaOCl as the standard protocol. The null hypothesis tested was that removing the smear layer using Er,Cr:YSGG laser irradiation would have no influence on the push-out bond strength of Resilon/RealSeal root canal fillings when compared with smear layer removal using 17% EDTA+5.25% NaOCl irrigation.
Materials and Methods
The present study was approved by the Dental School Ethics Committee, Tehran University of Medical Sciences, Iran. A total of 60 caries-free, single-rooted human teeth with straight canals were extracted for periodontal reasons, and selected for study. All teeth were radiographically assessed to ensure the absence of calcification, resorption, or curvature of root canals. The teeth were cleaned of soft tissue and calculus remnants and placed in 5.25% NaOCl for 2 h for surface disinfection. All samples were then stored in distilled water until the time of root canal therapy.
The crown of each tooth was sectioned at the cemento-enamel junction (CEJ) by a water-cooled low-speed diamond disk (Struers, Ballerup, Denmark), to create an average root length of 14–17 mm. A K-file #15 (Dentsply Maillefer, Ballaigues, Switzerland) was inserted into each root canal until it was visible at the apical foramen, and the working length was determined visually by subtracting 1 mm.
The root canals were prepared using Mtwo rotary files (VDW, Munich, Germany). Five instruments were used at the working length in each canal according to the manufacturer's instructions in the following sequence: (1) #15/0.05 taper, (2) #20/0.06 taper, (3) #25/0.06 taper, (4) #30/0.05 taper, and (5) #35/0.04 taper. Root canals were irrigated between each instrument using 5 mL of 0.2% Chlorhexidine (CHX) (Natural Pharma, São Paulo, Brazil). A final rinse with distilled water was used to remove CHX from root canals. The specimens were then randomly divided into two experimental groups based on the method used for removing the smear layer. One group (group 3) received no further treatment before obturation, and served as a positive control group (n=20 in each group).
In group 1, root canals were rinsed with 2 mL of 17% EDTA (DiaDent, Europe B.V. Almere, the Netherlands) followed by 5 mL of 5.25% NaOCl for 3 min. In group 2, the canals received 2.78 μm Er,Cr:YSGG laser irradiation (Waterlase Millenium, Biolase Technology, San Clement, CA), with a 320 μm RFT (RFT3 Endolase, Biolase Technology, Inc; calibration factor of 0.85) and the following parameters: output power of 1.5W, pulse duration of 140 μs, pulse frequency of 20 Hz, and 15% water pressure to 15% air pressure ratio. 23 The energy per pulse of 42 mJ and energy density of 5.25 J/cm2 was calculated. The laser tip was inserted into each canal at the working length, and manipulated continuously in a circular motion from apex to crown using a speed of 2 mm/sec. This irradiation procedure was repeated three times with a 20 sec break in between each irradiation. To ensure standardized and stable power outputs, a power-meter (FieldMaster, Coherent Inc., Auburn, CA) was used to calibrate the output power prior to each irradiation. All root canals were then irrigated with 5 mL of saline solution and carefully dried with sterile paper points #35 (Dentsply Ind. e Com. Ltda., Petropolis, RJ, Brazil).
Scanning electron microscope (SEM) evaluation
In order to evaluate the quality of smear layer removal, five roots from each group were randomly selected for assessment. A total of 15 root slices were prepared by sectioning the roots parallel to the long axis using a water-cooled diamond blade on a precision cutoff machine (Mecatome, Persi, France). Each slice was mounted on an aluminum stub, coated with 25 μm of gold-palladium, and examined under SEM (JSM-6400; JEOL, Tokyo, Japan).
Obturation of the specimens
RealSeal SE sealer (Pentron, Wallingford, CT) was mixed using an auto-mix syringe according to the manufacturer's instructions. Root canals (n=45) were obturated with #35/0.04 master cones using the cold lateral technique, RealSeal SE root canal sealer, and Resilon core material (SybronEndo Corp., Orange, CA). The excess material was removed with a heated instrument, and the surface of the filling material was light cured for 40 sec in order to create a coronal seal according to the manufacturer's recommendations. All samples were stored at 37°C and 100% humidity for 1 week to allow the setting of the sealer.
Preparation of root slices for push-out bond strength testing
Root slices were prepared by sectioning the middle third of each root, perpendicularly to the root long axis, into two 1.00±0.1 mm serial slices using a water-cooled diamond blade on a precision cutoff machine (Mecatome, Persi, France). In each group, 15 slices with a circular canal shape were selected for push-out testing. After measuring the thickness of each slice with digital calipers, the filling material was loaded with a cylindrical stainless steel plunger 0.7 mm in diameter in an apical-coronal direction. Care was taken to avoid any possible interference caused by root canal tapering. The plunger tip was positioned so that it would touch only the filling material, and not create stresses on the surrounding root canal walls. The loading was performed using a universal testing machine (Zwick-Roell Z050, Ulm, Germany) at a speed of 1 mm/min until debonding occurred. When the filling material was extruded from the root section and/or when a sharp decline was noted on the graph of a real-time computer program during compression testing, the bond was considered to have failed. 17
The maximum load (in Newtons), which was applied to the filling material before debonding occurred, was recorded. The bond strength in megapascals (MPa) was expressed as the proportion of the recorded load to the area of bonded interface, according to the following formula:
24
Where π is the constant 3.14, r is the root canal radius, and h is the thickness of the slice in millimeters.
Evaluation of failure modes
After the measurement of bond strength, tooth slices were examined under a stereomicroscope (NIKON Compatible Zoom Stereo Microscope sz6080, China) at×25 magnification to determine the mode of bond failure: 1, adhesive failure at the filling material/dentin interface; 2, cohesive failure within the filling material; or 3, mixed failure in both the filling material and dentin.
Statistical analysis
Data were analyzed using one way analysis of variance. Post-hoc pairwise comparisons were performed using Tamhane's multiple comparison tests. The significance level was set at α=0.05.
Results
Table 1 shows the mean and standard deviation (SD) of push-out bond strength of experimental and control groups. EDTA+NaOCl group (group 1) and laser group (group 2) showed significantly higher bond strength than did the positive control group [(p=0.010) and (p=0.004), respectively]. There was no statistically significant difference in push-out bond strength between group 1 and group 2 (p>0.05) (Table 2). SEM examination of the canal walls before obturation showed cleaned root canal walls with open dentinal tubule orifices in both groups 1 and 2 (Figs. 1 and 2). However, in group 2, debris was not completely removed from the canal walls (Fig. 2). SEM evaluation of root canal walls in group 3, which received no treatment, confirmed the presence of a thick smear layer (Fig. 3). Failure modes are presented in Table 3. There was a predominance of adhesive failures for all groups, indicating that the bond between sealer and dentin had been broken.
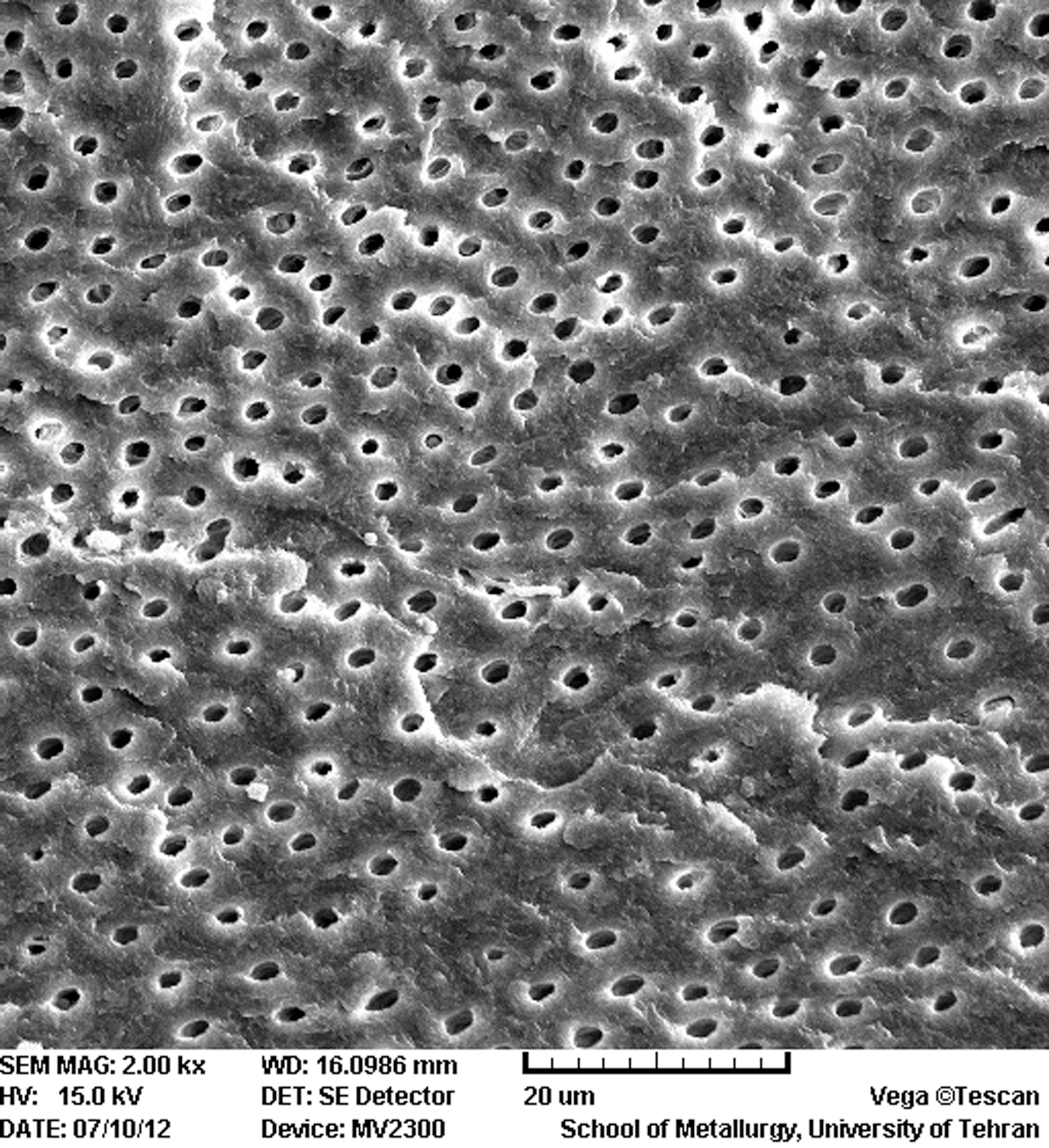
Effect of 17% ethylenediaminetetraacetic acid (EDTA) and 5.25% sodium hypochlorite (NaOCl) on middle third of the root canal wall [scanning electron microscopy (SEM); original magnification×2000].
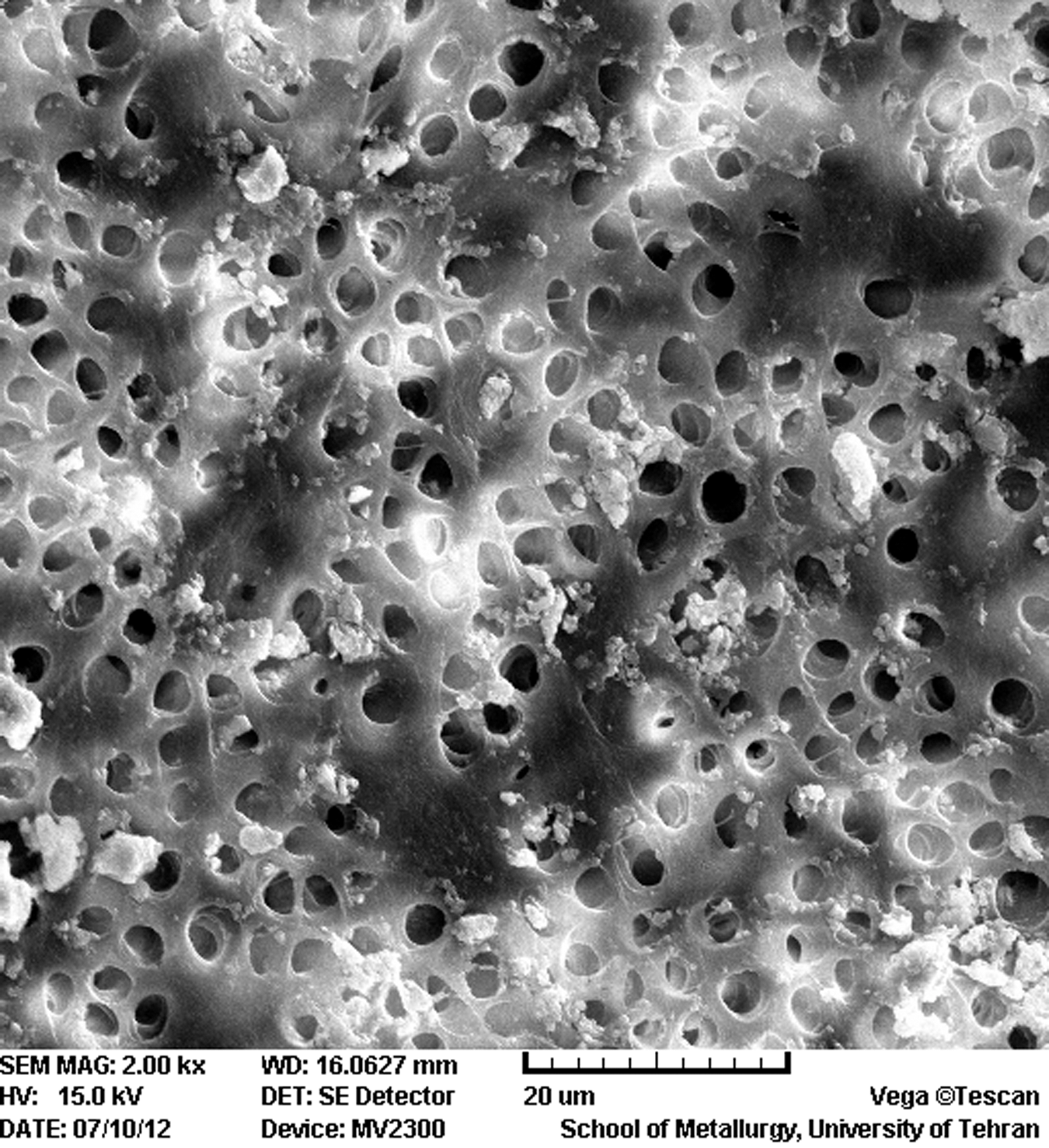
Effect of erbium, chromium: yttrium-scandium-gallium-garnet (Er,Cr:YSGG) laser irradiation on middle third of the root canal wall [scanning electron microscopy (SEM); original magnification×2000].
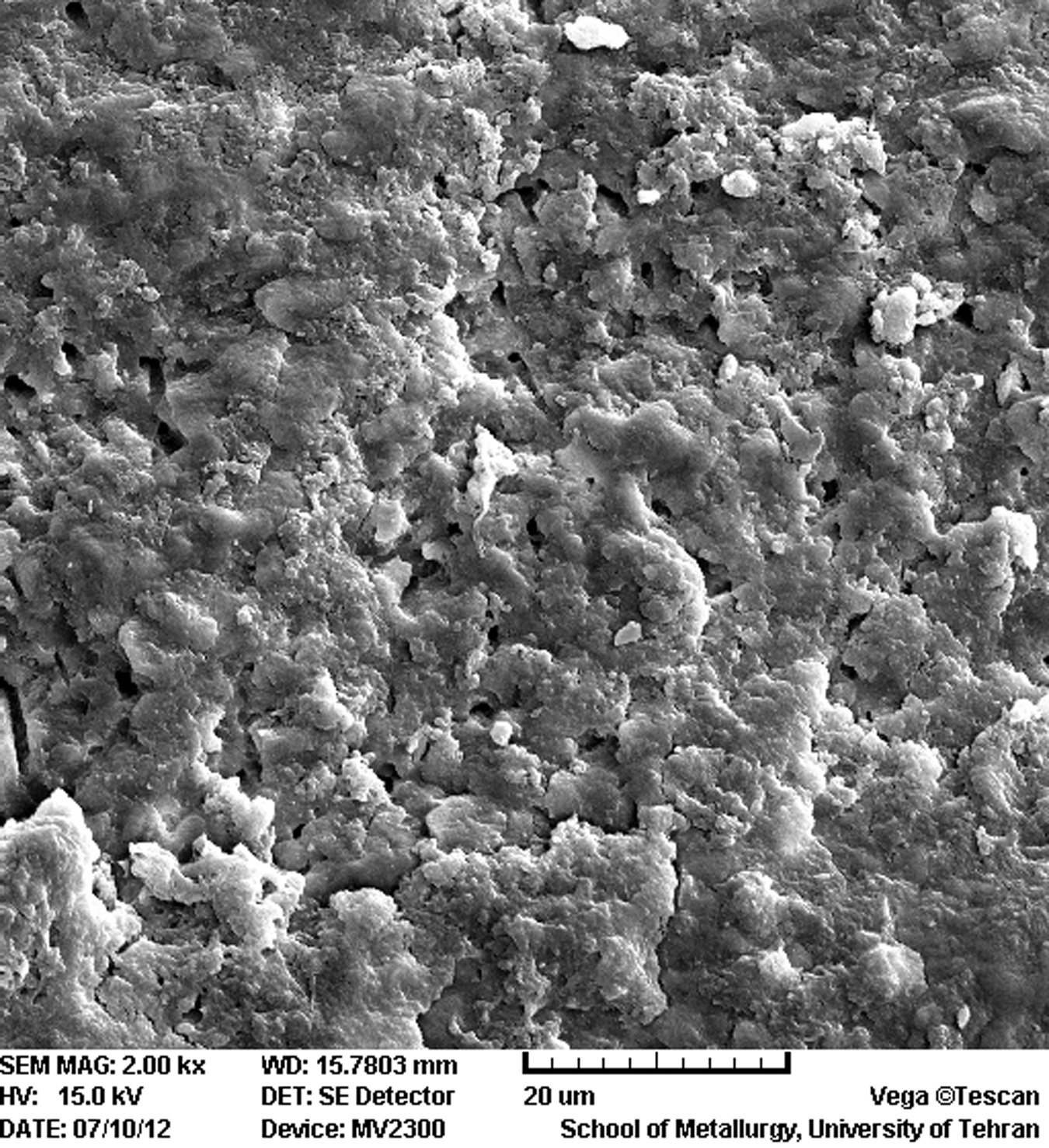
Scanning electron microscopic (SEM) image (original magnification×2000) of root canal wall in the positive control group. The image confirms the presence of smear layer.
EDTA, ethylenediaminetetraacetic acid; NaOCl, sodium hypochlorite.
The mean difference is significant at the 0.05 level.
EDTA, ethylenediaminetetraacetic acid; NaOCl, sodium hypochlorite.
EDTA, ethylenediaminetetraacetic acid; NaOCl, sodium hypochlorite.
Discussion
Recent studies have focused on seeking new ways to remove the smear layer to enhance the seal and adhesion of obturation materials. 25,26 Irrigation with EDTA followed by NaOCl has been established as a standard method for smear layer removal; 6,7 however, recent studies have raised concerns about this irrigation regimen. A study by Uzunoglu et al. 27 showed that using EDTA for smear layer removal reduces the fracture resistance of root canal treated mandibular incisors. Also, use of EDTA for >1 min can erode and damage root dentine. 28 Therefore, one can conclude that removing the smear layer without causing unfavorable changes in root structure poses certain challenges. In an attempt to try to circumvent unwanted changes in root dentin, researchers have recently focused on removing the smear layer using laser irradiation as a more conservative method. 25 However, because lasers might cause changes in dentin structure, the effects of laser irradiation on the adhesion of resin-based obturation materials bring about new questions that must be addressed.
Studies have shown that sealer can penetrate dentinal tubules following the use of EDTA for smear layer removal. 6 It has also been shown that a final rinse with 17% EDTA followed by NaOCl will remove the smear layer, because EDTA has the ability to dissolve inorganic components, whereas NaOCl can dissolve the organic components of the smear layer. 8 As in previous studies, 7,25 we used 2 mL of 17% EDTA followed by 5 mL of NaOCl 5.25% to remove the smear layer in group 1.
In group 2, the Er,Cr:YSGG laser was selected for the purpose of smear layer removal. It has been documented that the use of the Er,Cr:YSGG laser promoted increased cleanliness of surfaces compared with a combination of EDTA and NaOCl. 25 In addition, it has been demonstrated that lasers can effectively ablate dental tissues as well as remove the smear layer and debris. 23 According to previous studies, smear layer and debris removal can be achieved using Er,Cr:YSGG or Er:YAG lasers along with water irrigation during treatment. 26,29 Varella et al. 30 demonstrated that treatment of the dentinal walls with a laser promoted cleaner surfaces, and, subsequently, better adaptation of the filling material to the root canal walls when compared with a combination of EDTA and NaOCl. The application of an Er,Cr:YSGG laser with radial firing tips has brought about many advantages in root canal treatment, such as uniform coverage of root canal walls during irradiation. 14
An effective method for determining the strength of adhesion between endodontic materials and root structure is push-out bond strength testing. 31 Adhesion of sealer depends upon various factors, such as surface energy, cleanliness of root canal walls, sealer surface tension, and sealer wetting ability. 32 In the present study, we used Resilon/RealSeal SE, an alternative root filling material with increased adhesive properties. 18 Akisue et al. 33 showed that RealSeal had the highest adhesion to root canal walls among other resin-based sealers, as well as the highest mean shear bond strength. The aforementioned study also showed similar mean push-out bond strengths for specimens treated with an Er:YAG laser and Resilon/RealSeal, as compared with the results obtained in our study (4.02 MPa). Higher push-out bond strength of RealSeal sealer in comparison with non-etching sealers was shown by Babb et al. 21 The push-out bond strengths for RealSeal SE specimens were higher (12.6–14.9 MPa) than what we showed in this study. The differences in methods, including using sealer alone without core material, and the use of simulated canal spaces instead of true root canal spaces, might explain the differences in outcomes. Although the mean push-out bond strength of teeth treated with EDTA+NaOCl and filled with Resilon/RealSeal in our study was similar to what was shown by Onay et al. 17 (3.40 and 3.18 MPa, respectively); the mean push-out bond strength of teeth treated with the Er,Cr:YSGG laser in our study was higher (4.02 vs. 3.18 MPa) in comparison.
Previous studies have reported higher bond strengths of filling materials following Er,Cr:YSGG laser irradiation because of phase, compositional, and microstructural changes to dentin after irradiation; 34,35 other studies have shown no difference, 36 or lower push-out bond strengths with laser irradiation use. 37 The results of the present study showed no statistically significant difference between push-out bond strengths of the group treated with Er,Cr:YSGG laser irradiation (group 2) and the group treated with EDTA+NaOCl irrigation (group 1). Onay et al. 25 showed no difference between sealing ability of the resin-based sealers following smear layer removal with EDTA or Er,Cr:YSGG laser irradiation. In addition, they showed better adaptation of the root canal fillings to dentinal walls in specimens treated with EDTA than in those treated with laser irradiation.
The lowest push-out bond strength was evident in group 3 of the present study, in which we did not remove the smear layer. These results indicate the profoundly negative effects of remaining smear layer on push-out bond strength. The efficacy of the laser system in smear layer removal can be attributed to the ability of the radial firing tips to cover the whole of the root canal with irradiation in a homogenous and uniform fashion. 13,14 However, because the possibility of variable irradiation has to be considered (for example, the use of a tip size of 0.32 in the apical area of a canal prepared to a size of 0.35), we chose to conduct the push-out test on mid-root sections in order to ensure uniform laser irradiation in all samples. The highly correlative relationship between the results obtained from SEM evaluations of smear layer removal, and the push-out bond strengths determined from groups 1 and 2, indicate that the push-out bond strength test used to evaluate the adhesion of obturation material to dentinal walls is a decidedly reliable test. Nevertheless, the main purpose of this study was not to evaluate the quality of smear layer removal using the abovementioned protocols, and, therefore, we did not score SEM findings. This subject deserves further study.
Previous studies have demonstrated that the Er,Cr:YSGG laser causes minimal thermal damage to the pulp and surrounding tissues. 38 Other studies have shown that the increased temperatures precipitated by Er,Cr:YSGG lasers with an output power of 2 W neither melted root canal walls, nor damaged surrounding tissues. 39 The application of Er,Cr:YSGG lasers using radial firing tips with diameters of 300 or 400 μm, and an output power of 1.5 W, resulted in negligible temperature increases; the laser is, therefore, considered safe to use during root canal treatment. 14 Conversely, Altundasar et al. 40 assessed the ultramorphological and histochemical changes after Er,Cr:YSGG laser irradiation at an output power of 3W, and demonstrated areas of thermal damage, including carbonization and melting of dentinal tubules after laser treatment of root canals. It can be speculated that the higher output power led to thermal damage of root canal dentinal walls.
In the present study, failure modes were primarily of the adhesive mode in all groups (Table 3), which indicates failure at the filling material/dentin interface. Similarly to the findings of other studies, 31 it might be assumed that the RealSeal SE sealer adheres strongly to Resilon and weakly to dentin. Ungor et al. 31 showed that the failure mode results of push-out tests on the Resilon/Epiphany sealer were mainly adhesive. Another study on the bond strength of Resilon/RealSeal SE revealed that the failure modes were predominantly adhesive. 41 Conversely, Onay et al., 17 in a study on RealSeal sealer, asserted that the number of cohesive failures was distinctly more than that of adhesive failures. Other researchers have raised important questions regarding the concept of monoblock and the quality of bonding of Resilon-based root canal fillings/sealers to the root canal dentinal walls. 42 Recent studies on push-out bond strength of Resilon-based root canal fillings, including the present study, show that the failure pattern is largely adhesive. 31,43 Therefore, the concept of an effective monoblock for reinforcing root canal walls requires further study.
Conclusions
Within the limitations of this study, the application of Er,Cr:YSGG laser with radial firing tips did not adversely affect the push-out bond strength of RealSeal SE sealer to dentin. The use of this laser system with radial firing tips may be suitable for removing debris and smear layer from root canals. Additional studies are needed to further explore the effects of Er,Cr:YSGG laser irradiation with radial firing tips on root canal dentinal walls and removal of the smear layer.
Footnotes
Acknowledgments
This project was funded by grant #15778 from the Tehran University of Medical Sciences and Health Services. The authors express special thanks to Dr. Kharrazifard for his assistance with the statistical analysis of this research, and gratefully acknowledge Dr. Arabella Christian from the Post-Graduate Endodontic Department, School of Dentistry, University of Maryland in Baltimore for her English revision of this article.
Author Disclosure Statement
No competing financial interests exist.