
Abstract
Introduction
M
Therefore, clinicians should ideally find and adopt treatment strategies that could allow deeper penetration into dentinal tubules and eliminate microorganisms located beyond the host defense mechanisms. 13
The erbium, chromium:yttrium–scandium–gallium–garnet (Er,Cr:YSGG) laser, operating at a wavelength of 2780 nm, has been demonstrated to be a valuable tool to assist endodontic treatment without being hazardous to surrounding periodontal tissues, based on the high absorption coefficients in hydroxyapatite (OH-) groups and water molecules, and with consequent biophysical interactions. 14 –17
To overcome concerns related to the energy emission in axial direction and not toward the canal wall, the radial firing tips' (RFT) unique emission profile has been producing a significant improvement, as the beam expansion by the tip geometry not only reduces emissions in the forward direction but also favors homogeneous energy distribution along the root canal wall. 18 –20
In fact, erbium lasers have been demonstrated to induce shock waves in aqueous solutions inside root canals, and radial firing tips positively influence their configuration. 21 Hence, through the activation of aqueous solutions (e.g., water, EDTA) the Er,Cr:YSGG laser induces primary and secondary cavitation effects, useful for debris and smear layer removal. 16,22 –24
However, the best results in terms of thorough root canal disinfection with the Er,Cr:YSGG laser are achieved while operating in dry conditions, relying on the fact that–without water inside the main root canal–the ability of such wavelength to penetrate into the dentinal tubules is increased. 19,20,25
Both features–in the presence and absence of water–could justify this laser-assisted endodontic protocol as a straightforward method to achieve increased access and bactericidal effects into formerly unreachable parts of the tubular network. In addition, despite all in vitro reported applications, there is limited literature addressing the clinical outcomes of endodontic therapy using RFTs without the aid of chemical substances. 26
Therefore, the aim of this blind randomized clinical trial (RCT) was to evaluate the outcome of an Er,Cr:YSGG laser-assisted endodontic treatment compared with a traditional protocol in teeth with chronic apical periodontitis. The null hypothesis was chosen to demonstrate that the Er,Cr:YSGG laser could produce similar healing at 12 months when compared with 3% NaOCl irrigation and Ca(OH)2 dressing, using the periapical index (PAI) as outcome measure. 27
Material and Methods
Subject enrollment
Approval for the study protocol (N°682/068) was obtained from University of Porto Ethics Committee. Eligible participants were recruited from October 2009 to April 2011 from among patients who had attended the Faculdade Medicina Dentária Dental Clinic, at Universidade do Porto, Portugal, for initial nonsurgical root canal treatments. Those who met the main inclusion criteria, radiographic evidence of apical periodontitis (minimum size 1.0 mm in diameter) and a diagnosis of pulpless infected root canals confirmed by a negative response to sensibility pulp tests, were consecutively enrolled in the study. Whereas undergraduate students performed diagnosis, clinical and radiographic interpretations were verified by supervising faculty members. Single-rooted and premolar teeth with mature, fully formed apices were selected. Within-person assignment was allowed (two patients contributed with more than one tooth).
Patients were excluded if they were <12 years of age; pregnant; had a positive history of antibiotic use within the past month; had an indication for antibiotic prophylaxis (bacterial endocarditis or immunocompromising disorders); had uncontrolled hypertension or diabetes mellitus, chronic renal failure, hematologic diseases, HIV, osteoporosis treated with bisphosphonates; or were on steroid therapy >5 mg/day of prednisolone and prior to head and neck irradiation therapy. No compulsion was permitted in patient selection (e.g., prisoners). Teeth that were not restorable because of decay, teeth with abnormal root canal anatomy (more than 26 mm in length) and teeth with advanced periodontal disease were also excluded from the study. Effective rubber dam isolation technique was considered mandatory for inclusion in the trial.
Once eligibility was confirmed, one endodontic resident explained the study to the patient, and the patient was invited to participate. No financial incentive was offered (i.e., patients were responsible for the usual root canal treatment fee). All patients were advised that root canal treatment would be performed regardless of participation in the study. After oral and written informed consent (Helsinki Declaration 1973, revised in Edinburgh 2000) was acquired, participants were randomly assigned to either control (CON) or test (LAS) group using block sequences generated from a randomization computer program with a 1:1 ratio between groups. The flow of participants during the phases of the trial is detailed in Fig. 1.
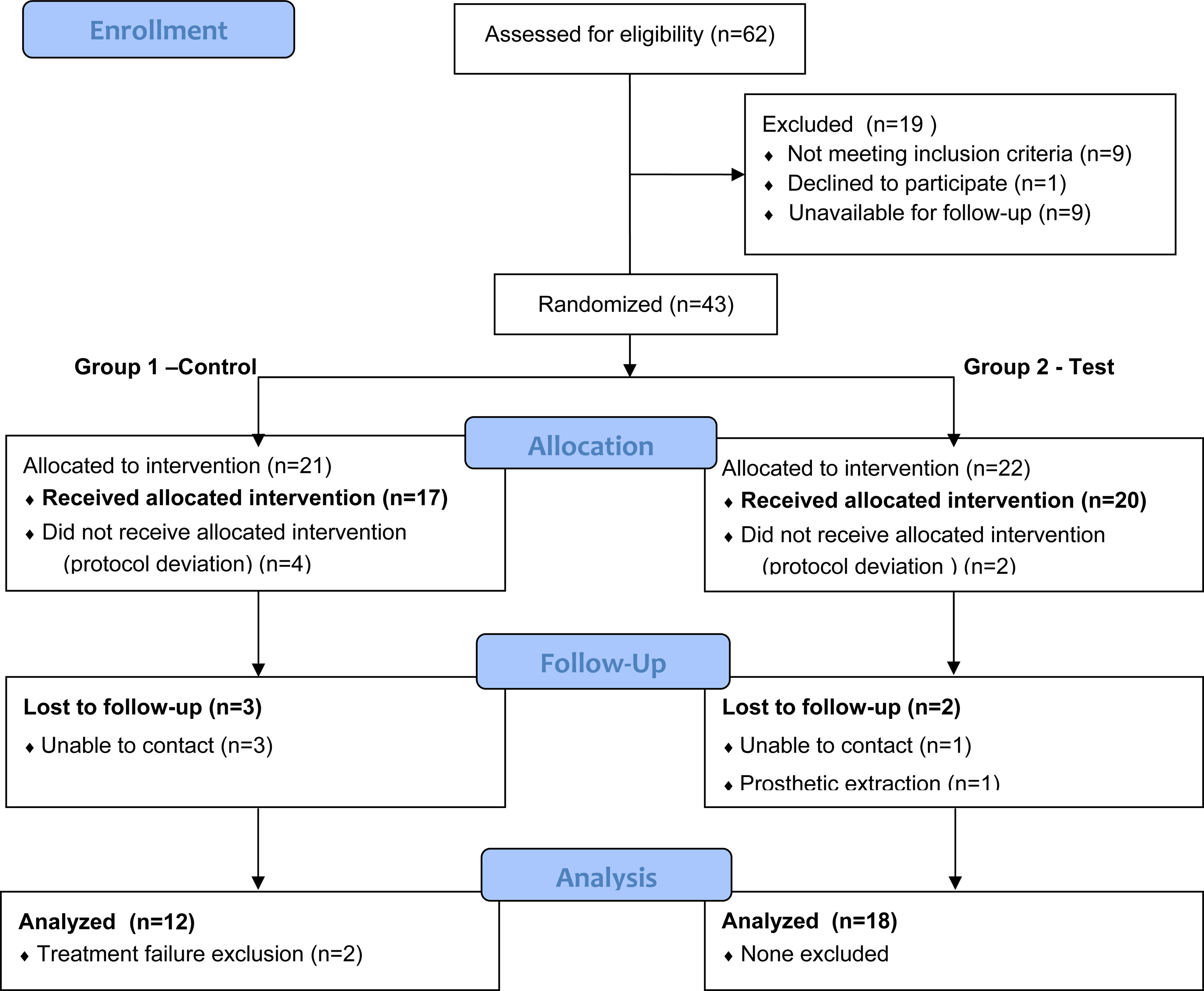
Consolidated Standards of Reporting Trials (CONSORT) flow diagram.
Allocation concealment and participants
Neither the undergraduate clinician nor the patient was aware of the group assignment before agreeing to participate in the study. Patient allocation was performed according to the sequence provided by the randomization tables, and all assigned interventions started immediately. If, for the same patient, more than one tooth was included in the study (within-person), the right or more mesial tooth was allocated to the control group. In consequence, the left or more distal tooth was allocated to the laser group. Laser irradiation was performed by the main investigator (M.R.M.). All other endodontic procedures were performed by enrolled 4th and 5th year students who were always supervised by staff who were not aware of group assignment. Two blinded and previously calibrated endodontic specialists (M.F.C., I.P.V.) independently scored the radiographs.
Standardized clinical procedures
Teeth in both groups were subjected to a common two-visit root canal treatment. All treatment sessions were performed by undergraduate students and each appointment was ∼3 h long. Local supraperiosteal anesthesia (2% lidocaine with 1:100,000 epinephrine, [Octocaine®] was administered as needed for patient comfort.
During the first visit, all carious lesions or previous restorations were removed. For each tooth, the access cavity was prepared and isolated with a rubber dam. Working length (WL) was established at 1 mm short of the biological apex of the root, with an ISO #15 K stainless steel file, being confirmed and adjusted using straight and angled radiographs. At the end of the first visit, a sterile cotton pellet soaked in Cresophène® (SEPTODONT, Kent, UK) was placed in the pulp chamber, and the access cavity was sealed with a reinforced zinc-oxide eugenol temporary cement (IRM®, Dentsply, Germany).
To complete the root canal preparation, the second visit was scheduled between 7–24 days after the first visit, and every patient was questioned for symptoms such as pain, sensitivity to percussion, or swelling. The tooth was then isolated with a rubber dam and the temporary filling removed, and the master apical file for each canal was set at least three sizes larger than the first file to bind at the WL. A minimum apical file of ISO #35 was required for all teeth. Subsequently, the canals were obturated using cold lateral compaction with handmade zinc-oxide eugenol as sealer (Zinc Oxide, Produts Dentaires SA, Switzerland) and gutta-percha (Gutta-Percha Points, ISO Color Coded–Dentsply, Maillefer). The access cavity was sealed with a reinforced zinc-oxide eugenol temporary cement (IRM), and a postoperative radiograph was taken. All teeth were restored permanently by the referring dentists within 30 days.
CON
During the first visit, root canal preparation was performed using the manual step-back technique with 1 mm increments using K-File instruments (Zipperer CC+ , VDW GmbH, Munich, Germany), and irrigated with 5.0 mL of 3% NaOCl after each increment until reaching the minimum enlargement of ISO #30 K file. Root canals were dried with sterile paper points and dressed with Ca(OH)2 paste. On the second visit, Ca(OH)2 paste was removed by using Hedstrom-type files (Zipperer, VDW GmbH, Munich, Germany) and copious irrigation with 3% NaOCl. Complete removal of the Ca(OH)2 paste was confirmed by visual inspection, and manual preparation was completed. After final irrigation with 5.0 mL of 3% NaOCl, the root canal was checked for the absence of suppuration or exudate, dried with sterile paper points, and obturated according to the previously described technique.
LAS
During the first visit, root canal instrumentation was performed as described for CON. However, irrigation was performed with 2.0 mL of sterile saline solution between files. After reaching the ISO #30 K file (Zipperer CC+, VDW GmbH, Munich, Germany), the main canal was filled with distilled water, and laser irradiation was performed with the 2780 nm Er,Cr:YSGG laser (Waterlase MD; Biolase Technology, Inc, San Clement, CA) and a 270 μm diameter radial firing tip (RFT2 Endolase, Biolase Technology, Inc; calibration factor of 0.55) with panel settings of 0.75 W, 20 Hz, 37.5 mJ per pulse, 14.0 J/cm2 energy density, 140 μs pulse duration, 0% water, and air. The tip was placed at the WL, and irradiation was performed at an approximate speed of 2 mm/sec−1 as the tip was withdrawn from the canal, until the most coronal part of the canal was reached. This procedure was repeated four times (two with the main canal filled with distilled water and the following two with the canal dry), with ∼15 sec between each laser irradiation. On the second visit, canal instrumentation was completed with saline solution as irrigant. A minimum apical file of ISO #35 was required for all teeth. The main canal was filled with distilled water, and laser irradiation was performed with a 320 μm radial firing tip (RFT3 Endolase, Biolase Technology, Inc; calibration factor of 0.85) with panel settings of 1.25 W, 20 Hz, 62.5 mJ per pulse, 23.6 J/cm2, 140 μs pulse duration, 0% water, and air. The laser protocol was identical to the first visit.
Following final irrigation with 5.0 mL of saline solution, the root canal was dried with sterile paper points, checking for the absence of any suppuration or exudate, and filled according to the previous obturation protocol.
Outcome classification and data analysis
The radiologic technique was performed by one operator (M.R.M.). The long-cone paralleling technique coupled to a film holder was used for both immediate postoperative and follow-up radiographs. Radiographic exposure settings (Trophy 70-X, USA Inc.) were recorded for each tooth, and follow-ups were reproduced under similar conditions. Radiographic images were coded and stored by two of the investigators (I.P.V. and J.A.C.).
The primary outcome measure for this study was change in apical bone density after 12 months. Presence of clinical symptoms or abnormal findings (e.g., spontaneous pain, swelling, mobility, and sensitivity to percussion or palpation) were recorded but not subjected to statistical analysis.
Follow-up radiographs were compared with those taken immediately after treatment, and the PAI was adopted to evaluate radiographic healing. 27 Radiographic evaluation was blinded and independently performed by two experienced, previously calibrated reviewers (M.F.C. and I.P.V.). Instructions for grading images with the PAI scoring system were adapted from Orstavik et al. 27 as follows: 1 (normal periapical structures), 2 (small changes in bone structure), 3 (changes in bone structure with some mineral loss), 4 (periodontitis with well-defined radiolucent area), and 5 (severe periodontitis with exacerbating features). All images were scored in a random order in a darkened room, using an illuminated viewer box mounted in a cardboard slit to block ambient light.
All reviewers (endodontists) were initially calibrated by evaluating 30 radiographic images not associated with the study sample, and representing a wide range of periapical bone densities. To assess intra-rater agreement, 1 week after the first session the examiners scored the same images; this method generated four PAI scores for each image, two from each of the two examiners. The examiners then met as a group to reach a consensus on cases that did not receive unanimous agreement, and reviewed all scores to enhance calibration and inter-rater agreement. A consensus score for each image was considered the definitive score to be used for statistical analysis.
Agreement between and within examiners was determined using the interclass correlation coefficient (ICC). Intra-rater reliability was measured with the single measure ICC (SPSS 17 for Windows; SPSS Inc, Chicago, IL), and inter-rater agreement was measured with the average measure ICC (also known as the inter-rater reliability coefficient). The adopted criteria regarding strength of agreement was: 0.00–0.20, slight agreement; 0.21–0.40, fair agreement; 0.41–0.60, moderate agreement; 0.61–0.80, substantial agreement; and 0.81–1.00, almost perfect agreement.
One week following the final calibration session, both reviewers randomly scored the study images, blinded to the treatment protocol used for each patient. When both reviewers agreed, the score was registered. When disagreement occurred, another reviewer (J.A.C.) decided the final score.
Sample size was determined to be the maximum number of participants who could be considered eligible during the recruitment period. To evaluate changes in PAI scores between groups and for each group from immediate postoperative to 12 month follow-up radiographs, the Mann–Whitney U and the Wilcoxon signed rank tests were respectively applied. The proportion of teeth in each group that could be considered unchanged, improved (decreased PAI score), or healed (PAI ≤2), was assessed with the χ2 Fisher's Exact Test. All hypotheses were conducted at 0.05 level of significance.
Results
Sixty-two patients were assessed for eligibility. Forty-three patients met the inclusion criteria and consented to participate in the trial. At the 12 month follow-up, 30 teeth were examined and subjected to statistical analysis, 12 in the CON group and 18 in the LAS group. Demographic characteristics for each group are listed in Table 1.
Failures were defined as the need for any additional treatment, and were not included in data analysis. There were two treatment failures before the 12 month examination (two in the CON group related to the presence of swelling and abnormal symptoms). In the LAS group, one tooth was extracted for prosthetic reasons before the 12 month examination, and was considered lost to follow-up. Five additional patients were lost to follow-up (Fig. 1). No adverse effects were found.
Before the consensus scoring meeting, intra-rater reliability score was 0.95, and the overall inter-rater agreement was 0.85, considered as almost perfect agreement.
For the CON group, two treatment failures were reported, and could not be accessed at the 12 month follow-up. The mean PAI score for the CON group was 3.83 (SD=0.89) at the immediate postoperative examination and 1.33 (SD=0.14) at the 12 month follow-up, a decrease of 2.50; the mean PAI score for the LAS group was 4.33 (SD=0.24) at the immediate postoperative examination and 1.72 (SD=0.16) at the 12 month follow-up, a decrease of 2.61. Whereas both groups exhibited a statistically significant decrease in PAI score (p<0.05) after 12 months of follow-up, no statistically significant difference was found between groups at either the immediate postoperative examination (p=0.14) or the 12 month evaluation (p=0.11) (Table 2).
Statistically significant differences are marked (*).
PAI, periapical index.
Despite the two treatment failures detected in the CON group that could not be assessed, there were no records of teeth with unchanged or increased PAI scores. In the CON group, all assessed teeth were considered healed (PAI ≤2); in the LAS group no treatment failures were detected, 88.90% of the teeth were considered healed, and 11.1% had improved (lower PAI score). These differences were also not found statistically significant (p=0.50). Characteristic examples of differences between immediate postoperative and 12 month follow-up radiographs can be found in Fig. 2.
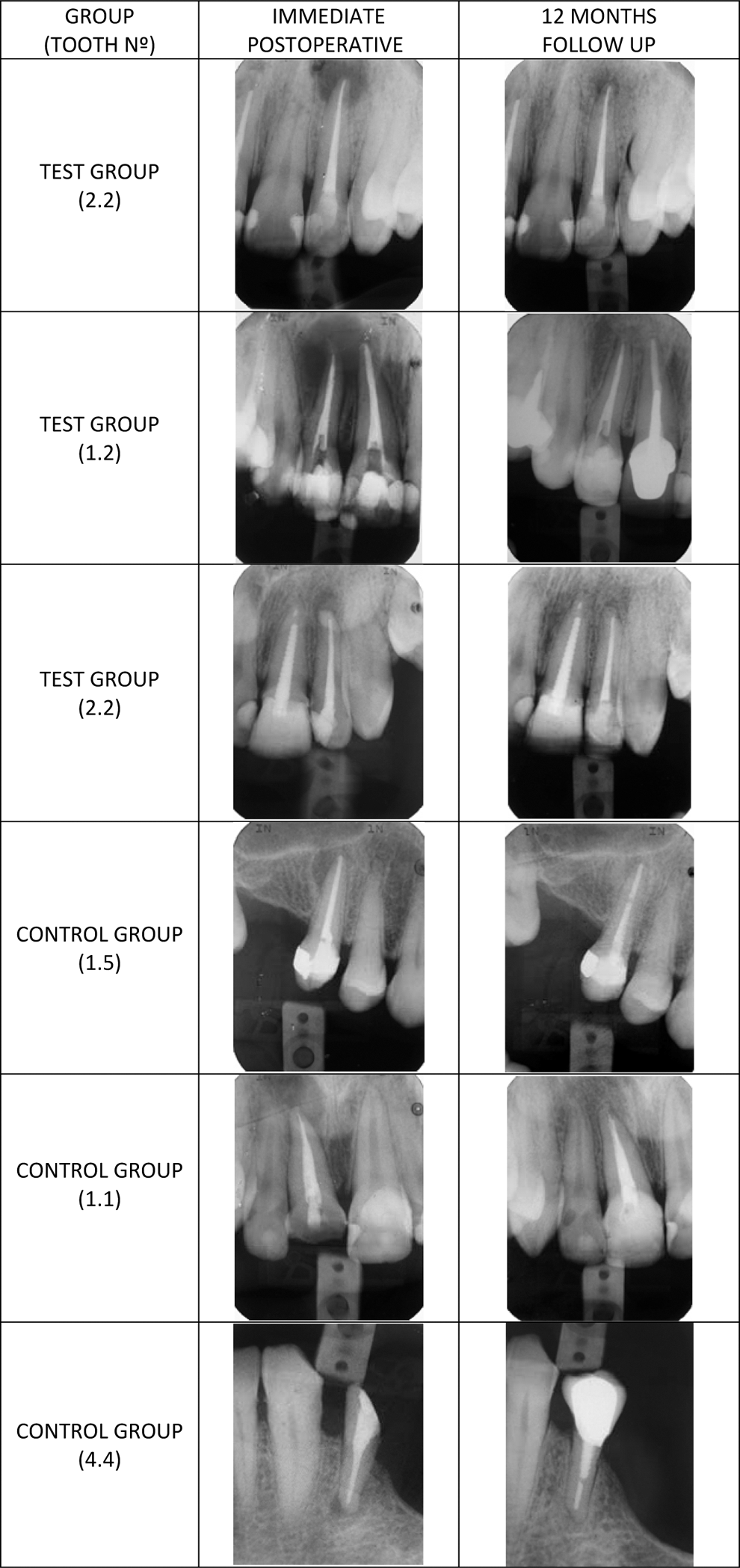
Characteristic examples of clinical radiographs for both test and control groups.
Discussion
To adopt a single wavelength treatment protocol that more reliably renders root canals free of smear layer and bacteria before filling seems interesting. Our findings confirmed the hypothesis that teeth treated with this novel laser-assisted protocol without the use of any chemical solutions would result in equal or superior outcomes when compared with conventional treatment.
The limited dentin penetration and consequent effectiveness of irrigating solutions such as NaOCl, against common endodontic pathogens, has caused some investigators to question its optimal concentration and use. 4 There is also no consistent evidence showing that two-visit root canal therapy with calcium hydroxide dressing would result in improved outcomes. In addition, given its low solubility, direct contact cannot always be achieved to effectively destroy bacteria harbored on untouched canal walls or dentinal tubules, and other anatomic variations. 6,28
Our findings are consistent with other well-designed endodontic clinical studies that found it difficult to report statistically significant differences while assessing conventional treatment outcomes. 9,28,29 Thirty patients from an original sample of 43 were randomly assigned and examined at the 12 month follow-up, 12 in CON and 18 in LAS. Although the participants and operators might not accurately represent the general population of patients and clinicians, this sample size can be considered arguably small, but typical, compared with similar trials. 5,30
All root canal treatments were performed by undergraduate students (according to a standardized protocol that represents the University of Porto consensus for best endodontic clinical practice) under close supervision and opportunity for assistance. Although undergraduates (4th and 5th year) can arguably be considered less skilled than general dentists, results of treatment under quality-controlled training conditions were found to be similar to those performed by experienced professionals. 31
In this study, the PAI score was not used as an initial inclusion criteria. However, the requirement that all teeth have a periapical radiolucent area ≥1.0×1.0 mm assured an initial PAI score ≥2. The mean immediate postoperative PAI scores were not significantly different between the two groups; therefore, difference between protocols was the only independent variable. Even though results can be influenced by unknown and uncontrolled variables (e.g., inclusion of smokers) that may predict poorer treatment outcomes, it was decided to exclude multirooted teeth from the study, as they appear to have lower probability for complete healing when compared with single-rooted teeth. 32
Although both groups were similar regarding basic demographic characteristics, in a randomized trial small baseline differences can be considered the result of chance rather than a source of bias (Fig. 1). In contrast, the mean dropout age was ∼10 years younger than the overall mean age, which can be found similar to findings obtained in another clinical trial. 28
Although clinical as well as radiographic data can be used to access treatment outcomes, the relative absence of clinical symptoms in CAP makes the assessment primarily a radiographic one. As a consequence, in endodontic controlled clinical studies, data generated by radiographic means are often used. 33 Radiographic diagnosis of apical periodontitis may be regarded as a complex task that is difficult to assess. However, systems for training and calibration of observers may improve diagnostic performance; namely, in the “periapical index” approach, which provides an ordinal scale ranging from “healthy” to “severe periodontitis with exacerbating features.” To validate and support the PAI reliability to measure radiographic changes in teeth with CAP, the ICC was used to determine the agreement between and within examiners. 28,34 A score of 0 represented no agreement beyond the level of agreement expected by random chance, whereas 1.0 meant perfect agreement. In this study, the intra-rater reliability and inter-rater agreement scores of 0.95 and 0.85, respectively, represented a very high level of agreement within and between examiners.
For this study, we were most interested in differences in apical healing between groups by measuring changes in the mean PAI score after 12 months. Results may verify whether predictable outcomes can be achieved with this protocol for the Er,Cr:YSGG laser-assisted endodontic treatment.
After 12 months of follow-up and with a 0.05 level of significance, there were no significant differences found between the two groups. In addition, both CON and LAS groups have been shown to be effective as independent treatment strategies, exhibiting significant differences between immediate postoperative and follow-up scores.
Conclusions
After 1 year of follow up, and in single-rooted and premolar teeth, the Er,Cr:YSGG laser has shown to be at least as effective as a conventional irrigation/medication regimen, reducing CAP significantly. Within the same clinical protocol, it can also confirm previous in vitro findings, suggesting that RFT could (1) remove smear layer in wet conditions, and (2) achieve deep disinfection in dry conditions.
These results should be considered preliminary, but relevant to clinically appraise the possible benefits of using RFT's physical characteristics either to achieve predictable outcomes or even to overcome conventional irrigation solutions' limitations. However, further studies should be performed to evaluate their efficacy with a larger sample size and in teeth that present additional challenges, such as intricate root canal morphologies and complex curvatures.
Footnotes
Acknowledgments
This research was not supported by any grants or manufacturers. The authors thank the Aachen Center for Laser Dentistry Institute (Aachen, Germany) for their personal motivation, and Daniela Abreu for the statistical evaluation done specifically for this study.
Author Disclosure Statement
No competing financial interests exist.