
Abstract
Introduction
T
Studies indicate that up to 50% of patients undergoing conventional or standard chemotherapy, and up to 80% of patients undergoing high-dose chemotherapy as conditioning for a stem cell transplant will develop symptoms at some point during their treatment. 3,4 The incidence of oral mucositis varies widely, depending upon the specific type of cancer and on the treatment modality. 5
Because of severe painfulness, oral mucositis affects oral physiological functions and the patient's quality of life, causing difficulties in drinking, eating, swallowing, and speech. 6 Severe mucositis (World Health Organization [WHO] grades III and IV) should be prevented, because it may cause an interruption in the course of radiotherapy or chemotherapy, being one of the most frequent causes of treatment delay, dose reduction in the treatment of cancer, and increase in cost and frequency of hospitalization of oncologic patients. 3,5,7
Onset of oral mucositis is a biologically complex process that has been partially elucidated at the molecular level. 8 –10 Chemotherapy leads to the generation of reactive oxygen species (ROS), which in turn activates several signaling pathways in the submucosa and epithelium. 11 Among these, nuclear factor-B is thought to be important, as it mediates the release of cytokines and cytokine mediators, cell adhesion molecules, acute phase proteins, and stress response genes. This, in turn, leads to a decrease in the renewal of epithelial cells, apoptosis, atrophy, and ulcer formation. Amplification of these events can also occur during the subsequent infection of compromised mucosal barrier by oral bacteria. 9 It is also important to highlight the role of cyclooxygenase pathway in the pathogenesis of oral mucositis, which is responsible for increasing the release of pro-inflammatory cytokines, including tumor necrosis factor (TNF)-α and interleukin-1 (IL-1)β. 3,12
Laser phototherapy (LPT) has been used for the prevention and treatment of oral mucositis, because of its anti-inflammatory, analgesic, and biomodulation effects. 13 –17 Over the past few years, our research group has been studying the effects of LPT on oral mucositis induced by chemotherapy, chemoradiotherapy conditioning regimens for hematopoietic stem cell transplantation (HSCT), or radiotherapy. 13,14,18,19 The visible red wavelength reduced the severity of oral mucositis and pain scores. 13,14,19 Moreover, LPT can keep mucositis levels at grades I and II. 14,18
In addition to LPT, the use of light emitting diode (LED) to treat oral mucositis has been recently studied, showing promising results. 20 –22 Comparative clinical studies between LED and LPT protocols to treat oral mucositis have not been performed. Therefore, clinical trials are necessary to test the effectiveness of LED in comparison with LPT in patients with oral mucositis caused by cancer therapy. Therefore, the aim of the present study was to compare the effect of LED and LPT protocols in the treatment of human chemotherapy-induced oral mucositis and pain.
Patients and Methods
Patients
A prospective study was conducted at the Special Laboratory of Laser in Dentistry (Laboratório Especial de Laser em Odontologia–LELO), from 2009 to 2012. Forty patients with chemotherapy-induced oral mucositis (CIOM) participated in this study.
Ethical considerations
The protocols for this study were approved by the Ethics Committee of the Faculdade de Odontologia at the Universidade de São Paulo, Brazil, and written informed consent was obtained from all patients. Patient care throughout the study was conducted in accordance with the principles of the Helsinki Declaration of 1975, as revised in 2000.
Inclusion criteria
The inclusion criteria were as follows: patients with chemotherapy-induced oral mucositis grade I, II, or III, who were ≥18 years of age and willing to cooperate with the treatment process and visual analog scale VAS analysis, and able to read and sign the informed consent.
Exclusion criteria
Patients were excluded who did not meet the inclusion criteria or received other treatments for oral mucositis lesions, or who had oral mucositis grade 0 or IV (WHO).
Clinical procedures
At the physical examination, the medical history of the patient was recorded. Information on basic illnesses, and on the type and stage of chemotherapy treatment was collected during the entire treatment. After physical examination, oral hygiene instructions were given to patients.
Two different phototherapeutic protocols were used randomly from the time of the patient's registration to 12–15 days later (10 consecutive days of irradiation, except for weekends). Regardless of the protocol used, oral examinations were conducted at the ambulatory care facility during each irradiation session, and the degrees of mucositis and pain were recorded daily.
LPT
One laser phototherapy protocol was used. Dentists were trained to perform laser irradiations in a standardized manner. For randomized patients, a laser phototherapy protocol was used (G1, n=23). Irradiations were performed daily, for 10 consecutive days, except for weekends; using an InGaAlP diode laser (Twin Laser—MMOptics® Ltda, São Carlos, SP, Brazil) with a wavelength of 660 nm, according to Simões et al. and Campos et al. 14,19
The Irradiation mode was punctual, in contact, and perpendicular to the oral mucosa. The laser power used was 40 mW, energy density of 6.6 J/cm2, power density of 1.1 W/cm2, and energy per point of 0.24 J (23,24). Irradiation time was 6 sec per point based on the laser beam spot size of 0.036 cm2. Irradiations were performed intra-orally, as follows: 12 points on each buccal mucosa (right and left), 8 on the superior and inferior labial mucosa, 12 on the hard palate and 4 on the soft palate, 12 on the lingual dorsum, 6 on the lateral edge of the tongue bilaterally, 2 on the right and left pillar of the tongue, 4 on the floor of the mouth, and 1 on the labial commissure bilaterally.
Trials of LED phototherapy
One LED phototherapy protocol was used (G2, n=17). The dentists were trained to perform LED irradiations in a standardized manner. The irradiations were performed daily using LED (Fisio LED–MMOptics® Ltda, São Carlos, São Paulo, Brazil), for 10 consecutive days, except for weekends, with a wavelength of 630 nm and with the same energy per point as was used in LPT (0.24 J). The power output was 80 mW, the energy density was 0.24J/cm2, and the irradiation time was 3 sec per point based on the LED beam spot size of 1 cm2. The power density was 0.08 W/cm2. The Irradiation mode was punctual, in contact, and perpendicular to the oral mucosa. Irradiations were performed intra-orally in the same manner as for G1.
For all therapeutic protocols, before and after each session, power output was checked using a power meter (Coherent Molectron®, Santa Clara, CA). Irradiations were performed following biosafety rules.
Assessment of mucositis grade
Oral mucositis was assessed in the first visit and on each phototherapy session, always before irradiations. The dentists were trained to perform standardized mucositis assessment based on the WHO grading scale, as follows
23
: 0: Patients with no visible clinical alteration in the oral mucosa 1: Soreness +/− erythema, no ulceration 2: Erythema, ulcers; patients can swallow solid diet 3: Ulcers, extensive erythema; patients cannot swallow solid diet 4: Oral mucositis to the extent that alimentation is not possible
Pain assessment
Patient self-assessed pain was measured using a VAS. This scale rates pain from 0 to 10, in ascending order. This assessment was made before each laser/LED phototherapy session.
Statistical analysis
The general results of the assessment on mucositis and pain in the same group (laser or LED) were compared using the Kruskal–Wallis test. After that, for the following statistical analysis, patients' data were grouped according to their initial grade of mucositis (I, II or III; WHO). The number of days required to achieve WHO=0 and VAS=0 for laser and LED groups was compared using the Mann–Whitney test. On the other hand, when the comparison was made within the same group, the Kruskal–Wallis test was used. The Fisher test was applied to compare the frequency of patients who achieved score 0 for mucositis and pain in both groups. In addition, the Wilcoxon test was performed to compare the mean grade of mucositis/pain between laser and LED groups. The level of significance adopted was 5% (p≤0.05).
Results
Clinical analysis
A total of 40 patients were included in this study (Table 1). Laser and LED irradiations were well tolerated and no adverse side effects were reported. Breast cancer was the most common cancer observed in G1 (22%) and G2 (47%) and, regardless of the type of cancer, most patients underwent surgery to remove the tumor (52% for G1 and 82% for G2). All patients were treated with a combination of drugs according to the chemotherapy regimen used, in which fluorouracil (5-FU) and cyclophosphamide were the most used drugs in both groups (39% and 26%, respectively, for G1; and 35% and 23%, respectively, for G2). Doxorubicin had also been frequently used in G1 (26%) and G2 (12%).
WHO and VAS
The initial mucositis grades of both groups were similar (p>0.05), varying from I to III. When VAS and WHO scores for laser and LED patients were analyzed, regardless of the experimental day and the initial mucositis grade, they were significantly lower for patients treated with LED therapy, when compared with those treated with laser (Figs. 1 and 2). These scores decreased in both groups throughout the experiment. VAS scores decreased significantly in 5 days for the laser group and in 7 days for the LED group (Fig. 2). WHO scores decreased significantly in 7 days for the LED group and in 10 days for the laser group (p<0.05) (Fig. 1).
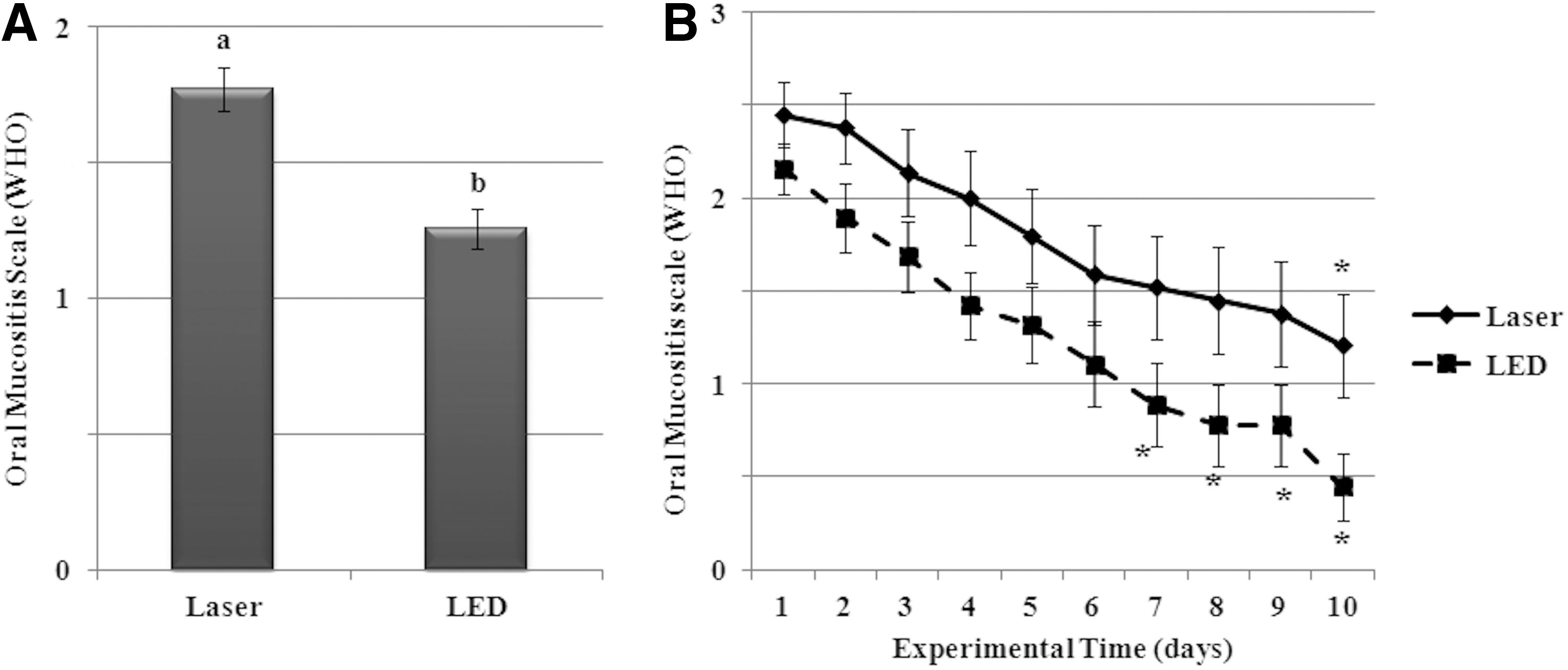
Data are shown as mean±standard error of oral mucositis score values (World Health Organization [WHO]) in
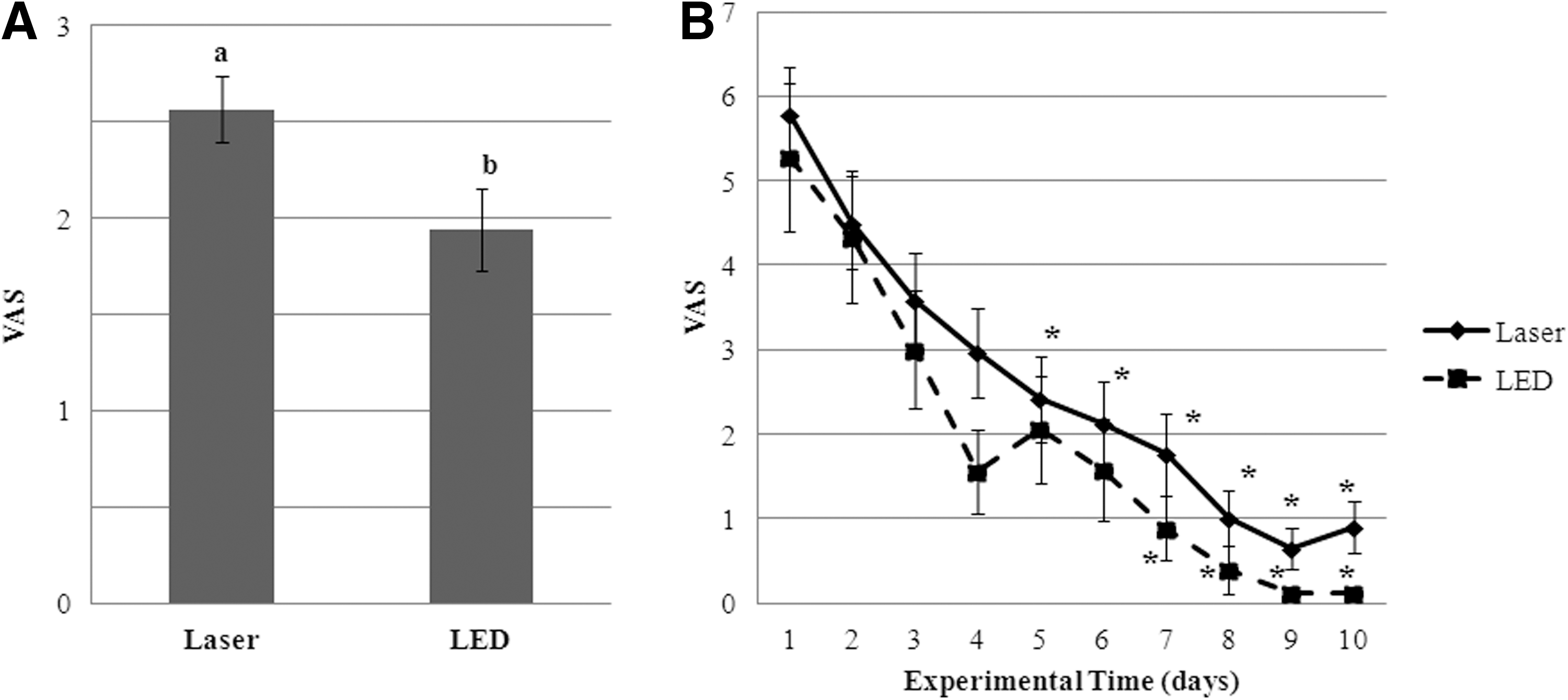
Data are shown as mean±standard error of the mean of the visual analog scale (VAS) in
Comparative analyses were performed grouping the patients according to their initial mucositis grade (I, II or III) to try to confirm if the difference between laser and LED phototherapies was consistent and not a reflection of their relative starting levels.
Analysis according to patient's initial grade of mucositis
The same number of days was required for patients from both groups, laser and LED, to achieve score 0 for mucositis, according to each initial mucositis score (WHO=I 4.6 and 4.5, WHO=II 5.8 and 5.2, and WHO=III 7.5 and 7.8, respectively, for laser and LED groups) (Table 2). In addition, although no statistically significant difference was observed, there was a clear trend: the higher the initial mucositis score, the greater the number of treatment sessions required to achieve score 0 for mucositis. Furthermore, we observed that all patients with initial mucositis score I achieved total healing of mucosa, whereas patients with initial mucositis score III showed the lowest percentage of total healing (25%).
p indicates comparisons between the groups (laser and LED), and letters indicate comparisons within the same group according to the initial mucositis score (WHO), where p≤0.05 and different letters indicate statistically significant differences.
WHO, World Health Organization; VAS, visual analog scale.
Concerning VAS scores, we observed that there was no statistically significant difference between the number of days required for the laser and LED groups to achieve score 0 for pain, according to each initial mucositis score (WHO=I 4.4 and 1.5, WHO=II 4.7 and 4.6, and WHO=III 6.0 and 8.0, respectively for laser and LED groups). In addition, patients of the LED group with initial score of severe mucositis (grade III; WHO) needed more days of treatment to achieve complete analgesia, when compared with patients with initial score for mucositis I or II (8.0; 1.5 and 4.6, respectively) (p<0.05). Furthermore, similarly to what occurred with mucositis healing, we observed that all patients with initial mucositis score I achieved total analgesia with both therapies. In addition, patients in the LED group with score III for oral mucositis also reached VAS=0. In addition, most patients with an initial score of mucositis II (G1 and G2) and III (G1) reached score 0 for mucositis (90, 90, and 65%, respectively).
WHO and VAS scores
Comparing the mucositis scores between the laser and LED groups according to patient's initial mucositis grade (I, II, or III), we observed that only for patients with initial mucositis score III (p=0.028), was the LED treatment more effective in healing oral lesions than the laser treatment (Table 3).
Indicates statistically significant difference.
VAS, visual analog scale; WHO, World Health Organization.
Comparing the mean of VAS score for G1 and G2, according to the patient's initial mucositis scores, the LED treatment was more effective for patients with initial mucositis scores I and II (p=0.012 and p=0.022, respectively).
Discussion
Some in vivo studies were performed to evaluate the effect of laser phototherapy (LPT) on the prevention and treatment of oral mucositis and pain. 13 –17,24 –28 However, to the best of our knowledge, there are no clinical trials comparing LPT with non-coherent LED therapy for the treatment of human oral mucositis and analgesia. Regarding the animal model, Freire et al., when comparing red LED and LPT in the prevention and treatment of chemotherapy-induced oral mucositis in hamsters, observed that both treatments stimulated healing and prevented the development of severe mucositis. In addition, the authors highlighted the importance of conducting further studies to compare the effects of these two therapies on the treatment of oral mucositis. 29
LPT has already been widely studied for the treatment of oral mucositis, 13 –17,24 –28 and some of these studies used a placebo-controlled group to determine its effectiveness. 13,25,27,28 Therefore, as the aim of this study was to compare a protocol already used (laser) with a promising therapy (LED), a control group was not used. Our data showed that VAS and WHO scores were significantly lower in the LED group. Moreover, our results suggest that patients with lower scores for initial mucositis have better results than those with initial mucositis score III (WHO), when treated with the two phototherapies.
Both LED and laser are light sources; however, the first one is produced primarily by the process of spontaneous emission, whereas the second one is produced by the process of controlled stimulated emission. 30 In addition, laser has high level of coherence (photons are well ordered), which is believed to be important for the laser therapy effect in deep tissues, 30,31 which is not true for superficial indications, as observed previously. 31 Clinically, LED light has a tip diameter larger than that of the laser, reaching a larger area and better distributing the energy. In this study, the energy per point (power×time) used was equal (0.24 J) for both therapies. The energy density, however, which is the measure of energy per unit of area (area of the laser or LED beam), was 6.6 and 0.24 J/cm2 for the laser and LED, respectively.
The LED power was twice as strong as the laser power (80 and 40 mW, respectively), resulting in 3 and 6 sec of irradiation per point, respectively. One advantage of the LED phototherapy protocol over the LPT protocol is that much less time is required to irradiate through the oral cavity.
Regarding LPT, it is known that these parameters significantly affect the treatment results. 30,32 Before examining these parameters, it is important to note that, although low light energy per point was used in this study (0.24 J) compared with other trials, 17,24,33,34 a key issue is the number of irradiation points and, consequently, the total energy applied. In this study, the number of irradiation points was 90, totaling 21.6 J for the total energy delivered to the tissue.
Considering the parameters used in this study, we can suggest that the analgesic effect observed in patients in the LED group could be, in part, produced by the higher power applied to this group. In a preliminary clinical study, Esper et al. analyzed the effect of two treatment protocols (laser and LED) on pain control in patients with orthodontic problems, and emphasized that the highest LED power was an important factor in producing the highest analgesic effect in the LED group, when compared with the laser group. 32 However, it is important to note that although the same energy density has been used, the LED side received 10 times more energy than the laser side, which may also have produced better results on pain relief in the LED group.
In a review of the literature regarding the effect of laser treatment on recurrent herpes labialis, Eduardo et al. reported pain reduction and modulation of the healing process related to the use of defocused high power laser. 35 In addition, Simões et al. also pointed out the importance of the use of defocused high power laser for analgesia of head and neck cancer patients with radiotherapy-induced oral mucositis. 14
Regarding wound healing, it seems that lower energy density is more effective, as LED therapy obtained better results. It is essential to highlight the importance of energy distribution, which was wider for the LED therapy because of its larger tip area (1 cm2 against 0.036 cm2). In addition, laser and LED equipments have different technologies, and the LED equipment has higher bandwidths.
Although the power output of the LED group was higher, and this group presented better results regarding wound healing, the correlation between power and healing is not conclusive. According to Lopes et al., hamsters that received lower power laser to treat 5-FU-induced oral mucositis showed improved healing. 36 Energy density, as mentioned, seems to inversely relate to wound healing, and on the other hand, there is no conclusive relation between power and healing. It is important to emphasize that the final effect was produced by the combination of all parameters used in this study. 32
LPT has been studied in the prevention and treatment of oral mucositis because of its anti-inflammatory, analgesic, and biomodulation effects. 13 –16,25,37,38 Our research group has been studying the effects of LPT on oral mucositis induced by chemotherapy, chemoradiotherapy conditioning regimens for HSCT, or radiotherapy. 13,14,18,19 The incidence of oral mucositis varies widely depending upon the specific cancer type and on the treatment modality used. 5 For example, in a retrospective study of clinical outcomes, oral mucositis was more frequent in patients treated with 5-FU than in those treated with other drugs. 4 In the present study, cyclophosphamide, 5-FU, and doxorubicin were the most frequent antineoplastic drugs used in the chemotherapy regimen for G1 and G2, and they are markedly mucotoxic agents. 39
Based on the results of our studies and studies of others, the advantages of using phototherapy for controlling signs and symptoms of oral mucositis in patients undergoing antineoplastic treatment are clear. 13 –15,18,19,25,38 However, the mechanisms underlying the effects of LPT in these patients are still not totally known. Our research group has shown, both in vitro and in vivo, that LPT can act on cell proliferation, cytokine production, and salivary gland stimulation, as well as on mast cell degranulation. 40 –45 In addition, LPT appears to reduce the severity of mucositis, at least in part, by reducing COX-2 levels. 37 These are physiological mechanisms related to inflammation and wound healing processes, which in turn could influence the positive effects of LPT in patients under radiotherapy or chemotherapy.
LED is a relatively new type of light source that has been used alternatively to laser. 20 It has been demonstrated that LED may have a healing effect similar to that of laser on skin and mucosal wounds, causing an increase in fibroblast proliferation. 46 In addition, depending upon the desired wavelengths, it is a less expensive alternative to LPT, and it has longer durability. 20
It is important to note that severe oral mucositis (grades III–IV; WHO) can have a significant impact on the cancer treatment plan, and efforts should be made as much as possible to prevent it. Both therapies analyzed in this study were efficient in preventing breaks in the antineoplastic treatment, promoted better health in patients, improved patients' quality of life, and reduced treatment cost and hospitalization period. In addition, lasers and LEDs are atraumatic and noninvasive techniques. As a result, their use in the oral cavity of oncologic patients is increasing.
Conclusions
These findings suggest that LED therapy is more effective than LPT in the treatment of COIM with the parameters used in the present study. However, both therapies analyzed in this study were efficient in preventing breaks in the antineoplastic treatment and promoted better health in patients.
Footnotes
Acknowledgments
The authors thank FAPESP (The State of São Paulo Research Foundation, #2010/03662-6, #2010/16122-0 and #2011/14013-1) for financial support. The authors also thank Antonio Muench for his valuable contribution to statistical analyses.
Author Disclosure Statement
No competing financial interests exist.