
Abstract
Introduction
I
Antimicrobial photodynamic therapy (APDT), which involves the use of photosensitizing drugs (PS), and visible light of a specific wavelength, is a promising therapeutic modality for the inactivation of bacteria causing wound infections. 4,5 This approach has the advantage that both antibiotic-sensitive and resistant strains can be successfully inactivated. The effect of APDT on inactivation of bacteria in wounds has been verified in real time using genetically engineered bioluminescent bacteria and a light-sensitive imaging system. 6 Apart from inactivating bacteria, APDT can also accelerate healing in bacteria-infected wounds. 6 –8 Nevertheless, results reported on healing are contradictory. There are reports that PDT does not influence wound healing, 9 –11 or may even cause epidermal necrosis, decrease in tensile strength, and delayed healing. 12 The variations in these studies 9 –12 might have arisen because of the differences in photosensitizer administration modes, light irradiation doses, and the random sampling by invasive techniques such as histology.
In bacteria-infected wounds, direct collagenolytic action of bacterial proteases 13 or bacterial protease induced activation of latent host collagenases 14 such as matrix metalloproteinases (MMP) 15,16 contribute to the degradation of collagen, causing delayed wound healing. Bacterial endotoxins are also known to inhibit development of wound tensile strength. 17 Therefore, inactivation of bacteria and the bacterial proteases 18,19 following PDT are expected to reduce inflammation and restore collagen remodeling in wounds. In our earlier study, 19 we observed that topical APDT in Pseudomonas aeruginosa infected wounds, reduced the hyperinflammatory response and improved wound healing. These observations were verified by histology. However, histology provides semiquantitative information on collagen remodeling and, because of its invasiveness, leads to random sampling.
Another approach used for monitoring wound repair is hydroxyproline assay. A limitation of this approach is that it provides an estimation of collagen content and does not indicate the collagen cross-linkage 20 required for wound closure. Collagen is birefringent and its ordering contributes to tissue birefringence, which can be quantified using polarization sensitive optical coherence tomography (PSOCT), a real-time, noninvasive cross-sectional imaging tool. Therefore, both OCT 21 and PSOCT 22,23 have been utilized for visualization of morphological changes in wound healing. In a previous study using PSOCT, we were able to quantify decrease in collagen remodeling in bacteria-infected superficial wounds by measuring birefringence of wounds. 24 In this article, we report on the effect of poly-L-lysine-conjugated chlorin p6 (pl-cp6)-mediated APDT on collagen restoration in murine excisional wounds infected with methicillin-resistant Staphylococcus aureus (MRSA) and P. aeruginosa (PAO), studied using PSOCT. These results have been validated by histology, hydroxyproline assay, and immunoblotting.
Materials and Methods
Bacteria
The bacteria used in this study were PAO (MTCC 3541, Chandigarh, India) and MRSA (ATCC 43300). Both bacteria were maintained routinely by subculturing in tryptone soya agar (TSA) (Himedia, Mumbai, India). For experiments, a colony of the bacteria was inoculated into TSA and was grown aerobically for 18 h at 37°C using a shaker incubator. Optical density of the exponential culture of bacteria was measured at 600 nm, and diluted to obtain required concentration.
Establishment of excisional model of wound infection and PDT of wounds
A total of 60 female Swiss albino mice (weight ∼25 g, 8 weeks of age) were used for all experiments. All animals were housed in individual cages under constant temperature (20±4°C) with a 12 h light /dark cycle, and had free access to food and water. In anesthetized mice, excisional wounds of ∼1.2×0.8 cm (length×width) were created on the dorsal skin. Infection of the wounds was initiated by applying ∼108 colony-forming units (CFU) MRSA or ∼107 CFU PAO growing in exponential phase. Mice with wounds were divided into following groups: (1) uninfected wound, (2) wound infected (with either MRSA or PAO) and untreated, (3) infected dark control (treated with only pl-cp6), and (4) infected PDT group (treated with pl-cp6 and light).
For PDT, 20 μL of 100 or 200 μM of pl-cp6, prepared as described by Sahu et al. 19 was applied topically to the wounds, at 48 h post-infection. After 30 min of drug application, wounds were exposed to light (660±25 nm) using light source LumaCare™ LC-122 (Ci-tek, USA) at a constant power density (∼100 mW/cm2), for 10 and 20 min to achieve light irradiation doses of 60 and 120 J/cm2, respectively. The Institutional Ethical Committee, in accordance with the institutional guidelines on animal care, approved all procedures involving animals.
PSOCT imaging of wounds in vivo
Figure 1 shows a schematic of the PSOCT setup used for imaging of the wounds, the details of which are described in our earlier article. 24 OCT (back-scattered intensity) image was obtained by summing the squares of amplitude of the orthogonal polarization components. The PSOCT (phase retardance) images are displayed as spatial maps of optical phase retardation obtained by computing the arctangent of the ratio of IH and IV. 25 The axial and lateral resolutions of the setup were ∼11 and ∼17 μm, respectively. The image acquisition time was ∼2 min for an image comprising of 200×1000 pixels. In each wound approximately six to eight different regions were scanned. Axial scan registration was performed to minimize the motion artifacts of breathing in anesthetized mice. The measured phase retardation as function of depth was averaged over 10 consecutive lateral positions (spaced by ∼17 μm). From this, the phase retardation per unit length was calculated by a linear fitting of the data. Each imaging measurement was repeated three times.
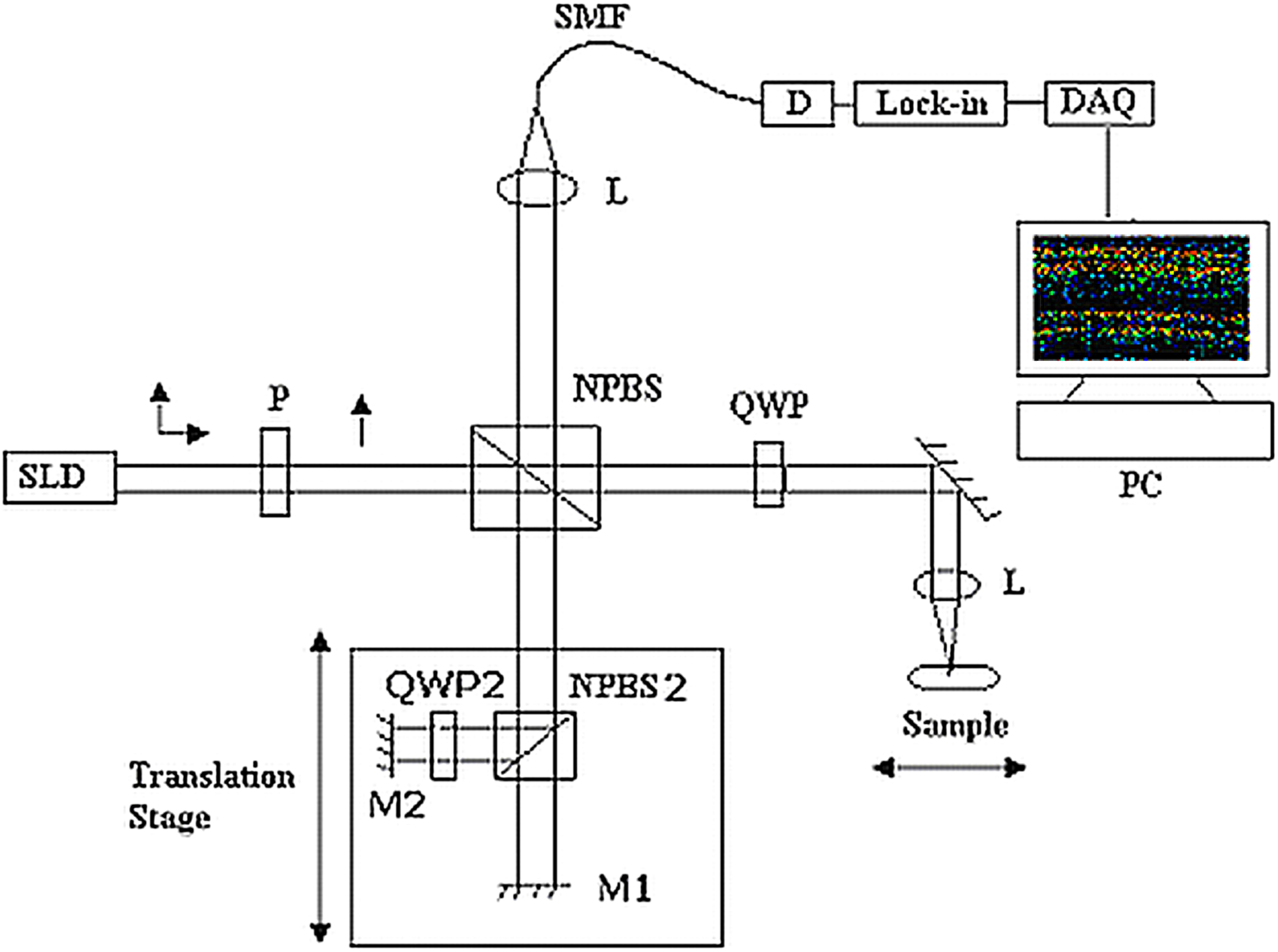
Polarization sensitive optical coherence tomography (PSOCT) setup used for imaging. P, polarizer; L, lens; M, mirror; NPBS, nonpolarizing beam splitter; QWP, quarter wave plate; DAQ, data acquisition board; SLD, superluminescent diode.
Histopathological analysis
On day 18, mice were euthanized by cervical dislocation. An ∼1×0.8 cm portion of dorsal skin including the wound region was excised. The tissues were fixed in 10% neutral buffered formalin for 24 h and processed using standard histological procedure. The deparafinized sections were stained with Masson's trichrome stain, and examined under a microscope to observe inflammation, re-epithelialization, and arrangement of collagen fibers.
Hydroxyproline assay
Mice were euthanized on day 18 and an ∼1×0.8 cm portion of dorsal skin including the wound region in the middle was excised, weighed, frozen in liquid nitrogen, and stored at −80°C until use. Hydroxyproline assay was performed according to the protocol described in Reddy and Enwemeka, 26 and the values were expressed as milligram (mg) hydroxyproline per gram (g) tissue weight.
Western immunoblot analysis
On day 5, mice were euthanized, and wounds along with ∼2 mm of wound margin were excised. The supernatant of wound homogenates, prepared according to the protocol, 27 was used for immunoblotting and protein estimation. Protein samples (∼50 μg) separated by sodium dodecyl sulfate-polyacrylamide gel electrophoresis (SDS-PAGE) were electroblotted to nitrocellulose membrane. The membranes were incubated with anti-MMP-8 (sc-8848), MMP-9 (sc-6840) antibodies (Santa Cruz Biotech, USA) followed by incubation with horseradish peroxidase (HRP)-conjugated secondary antibodies. Blots were developed using protocol described in an ECL kit (RPN2135, Amersham Biosciences, GE Health Care Life Sciences, USA). Chemiluminescence images were captured with an imaging system (Chemi-HR-16, Syngene, UK) and processed using GENESNAP software (Syngene, UK). Densitometry was performed using software GENETOOL (Syngene, UK). GAPDH was used as a loading control. Blot intensities of MMPs were divided with that of the GAPDH. To quantify treatment effect, intensities of the blots of uninfected wounds were divided with that of other groups.
Statistics
The results were represented as mean±standard deviation of three independent measurements performed in at least six animals. The statistical significance of the difference between means was assessed by one way ANOVA. P<0.05 was considered statistically significant.
Results
OCT imaging of MRSA-infected wounds subjected to PDT and comparison with histology
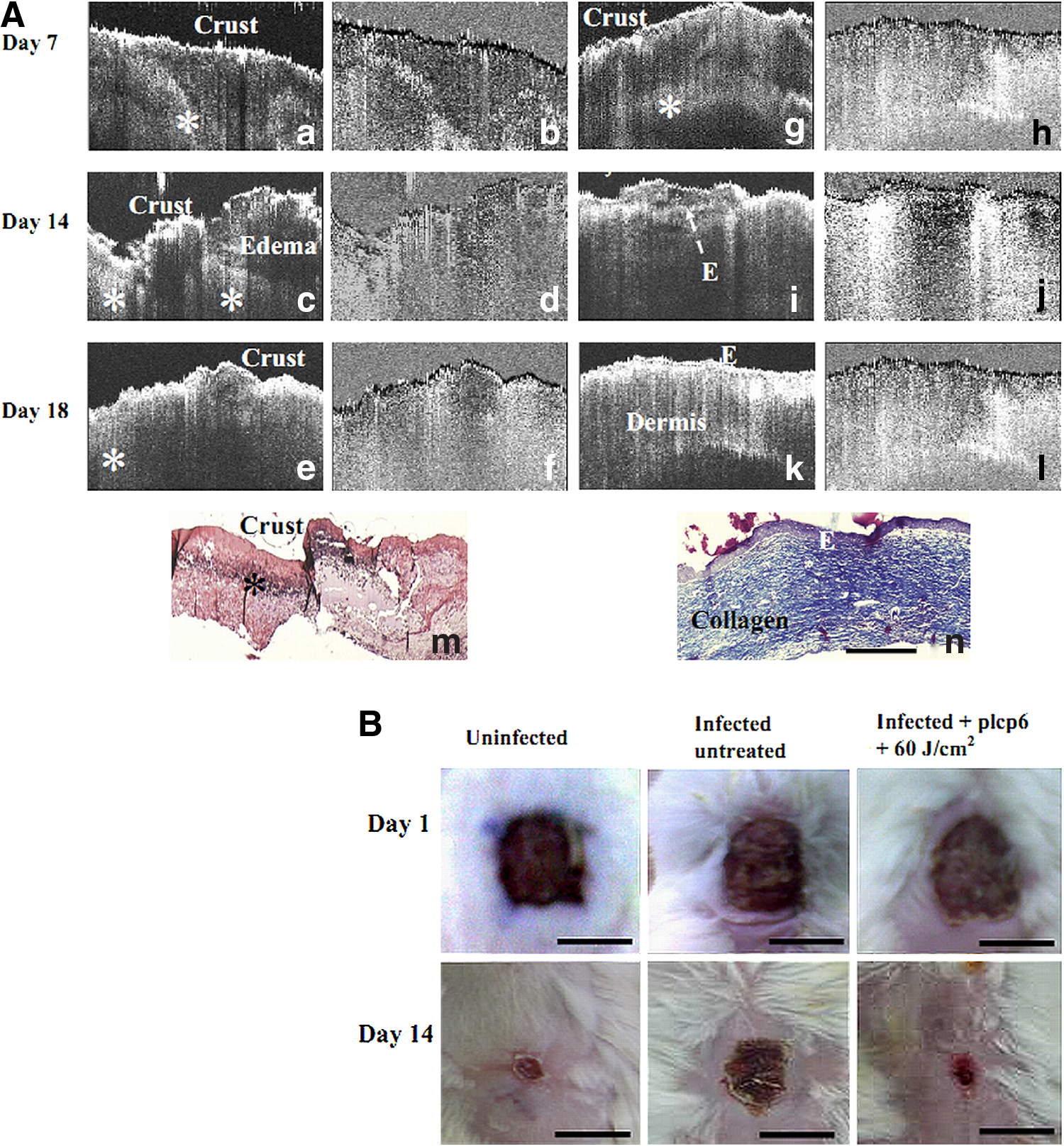
Figure 2 shows representative OCT, PSOCT, and histological images of uninfected and MRSA-infected wounds. In uninfected wounds, on day 7 (Fig. 2a), the back scattering images showed a highly scattering crust on the wound surface below which the newly formed epithelial layer was observed. The patches of scattering regions observed below the new epithelium layer (star mark, Fig. 2a) at wound margin indicate early granulation tissue. The corresponding retardation image (Fig. 2b) of the wound bed showed a relatively weak polarization contrast. 25 At this time point, phase retardance (∼0.03 degree/μm) of wounds was much lower than that of normal skin (∼0.2). On day 14 (Fig. 2c) and day 18 (Fig. 2e), the crust was completely absent and back-scattered intensity of wounds increased considerably. The birefringence images, on day 14 (Fig. 2d) and day 18 (Fig. 2f), also showed increased retardation compared with that of day 7. The phase retardance of wounds on day 14 and 18 were ∼0.05 and ∼0.07 degree/μm, respectively, indicating restoration of connective tissue.
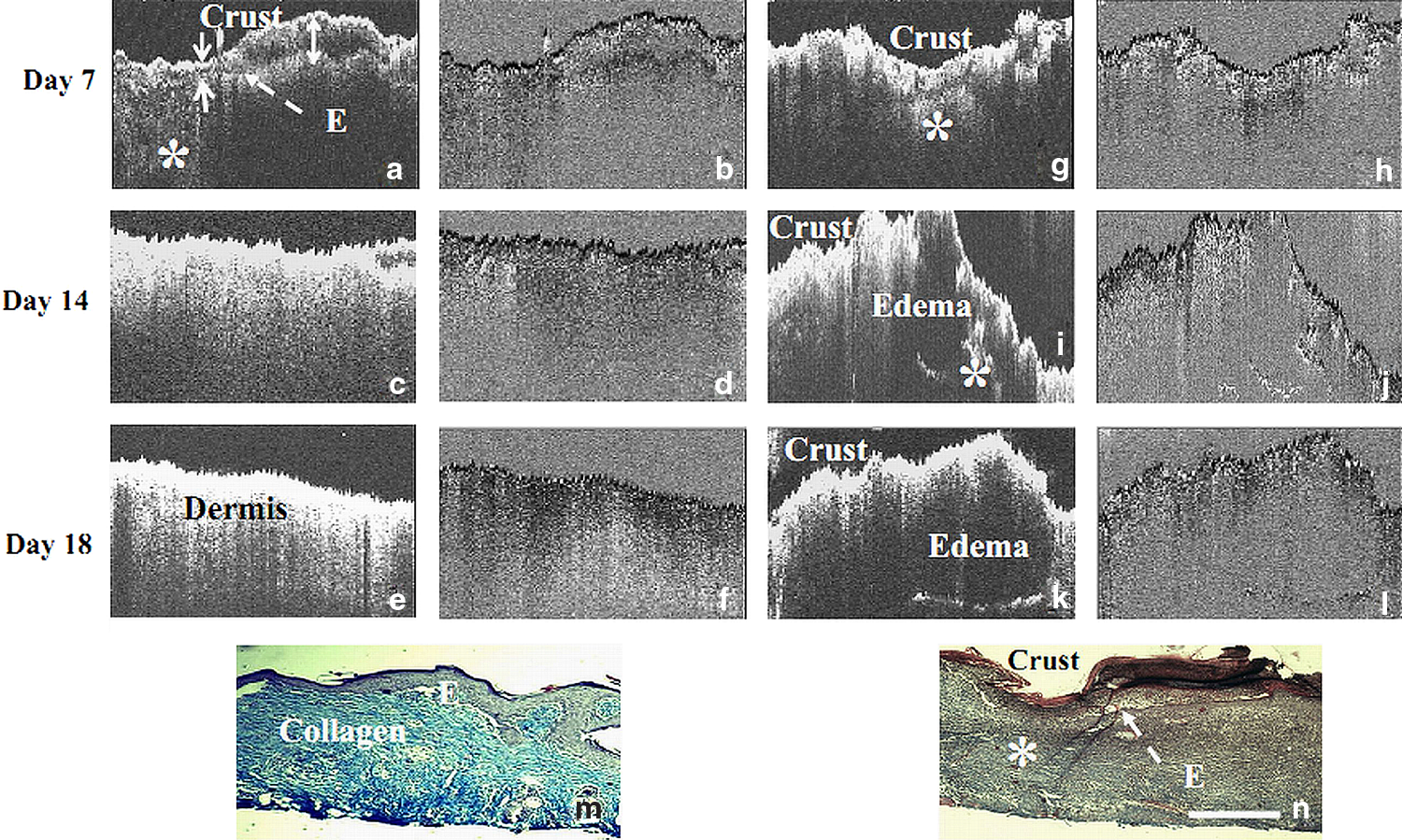
Time-dependent structural changes in uninfected (
The OCT images of MRSA-infected wounds (Fig. 2g, i, k) showed the presence of much thicker crust, and prolonged edematic response. Also, considerably less polarization contrast was observed at all the post-wounding time points (Fig. 2h, j, l). The phase retardance on day 18 was significantly lower (∼0.032 degree/μm) than that of uninfected wounds. The structural features observed in the OCT images of the uninfected and infected wounds were consistent with those of the histology images. Compared with uninfected wounds (Fig. 2m), infected wounds (Fig. 2n) showed more inflammatory exudates, incomplete epidermis, and lesser trichome staining, indicating less ordered collagen.
Figure 3 shows OCT, PSOCT, and histological images of wounds of MRSA- infected dark control and PDT (60 J/cm2) group. The scattering and phase retardance patterns observed in the OCT images of the infected dark control wounds, on day 7 (Fig. 3a, b), 14 (Fig. 3c, d), and 18 (Fig. 3e, f) were similar to those of the untreated infected wound (Fig. 2g–l). In contrast, infected wounds subjected to PDT on day 7 (Fig. 3g, h), 14 (Fig. 3i, j), and day 18 (Fig. 3k, l) showed increased back-scattering and fewer edematic regions. The phase retardance of the treated wounds on day 14 (∼0.045 degree/μm) and day 18 (∼0.06 degree/μm) were significantly higher (p<0.05) than the phase retardance values of both untreated and pl-cp6 (100 μM) treated wounds on day 18 (∼0.032 degree/μm). Consistent with the PSOCT images and calculated retardance, histological analysis of infected wounds subjected to PDT showed lesser inflammatory cells, a completely formed epidermis, and denser trichrome staining than MRSA-infected dark control (Fig. 3 m, n) wounds. Infected wounds subjected to a higher light dose (120 J/cm2) showed no significant differences in the scattering features, birefringence, and trichrome staining pattern (data not shown).
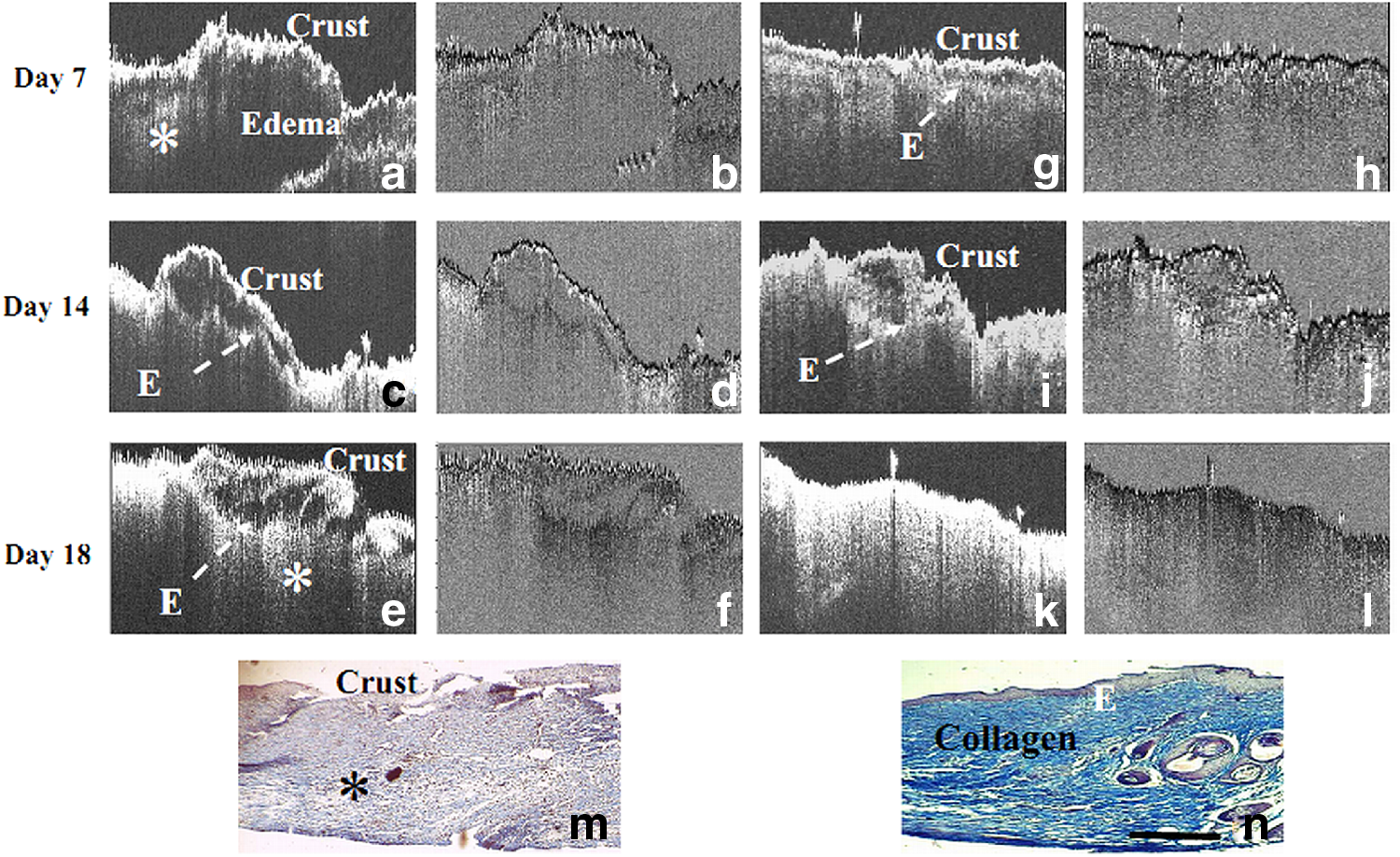
Time-dependent structural changes in methicillin-resistant Staphylococcus aureus (MRSA) infected wounds treated with pl-cp6 in dark (
Effect of PDT on hydroxyproline content of MRSA-infected wounds
In order to confirm the changes in retardance and collagen staining pattern observed in the wounds, hydroxyproline content was estimated on day 18. The results (Fig. 4) showed that in infected wounds subjected to PDT, hydroxyproline contents were approximately threefold higher (p<0.05) than those of untreated or dark control wounds. However, there was no PDT dose-dependent difference in the hydroxyproline level of the wounds (p>0.05).
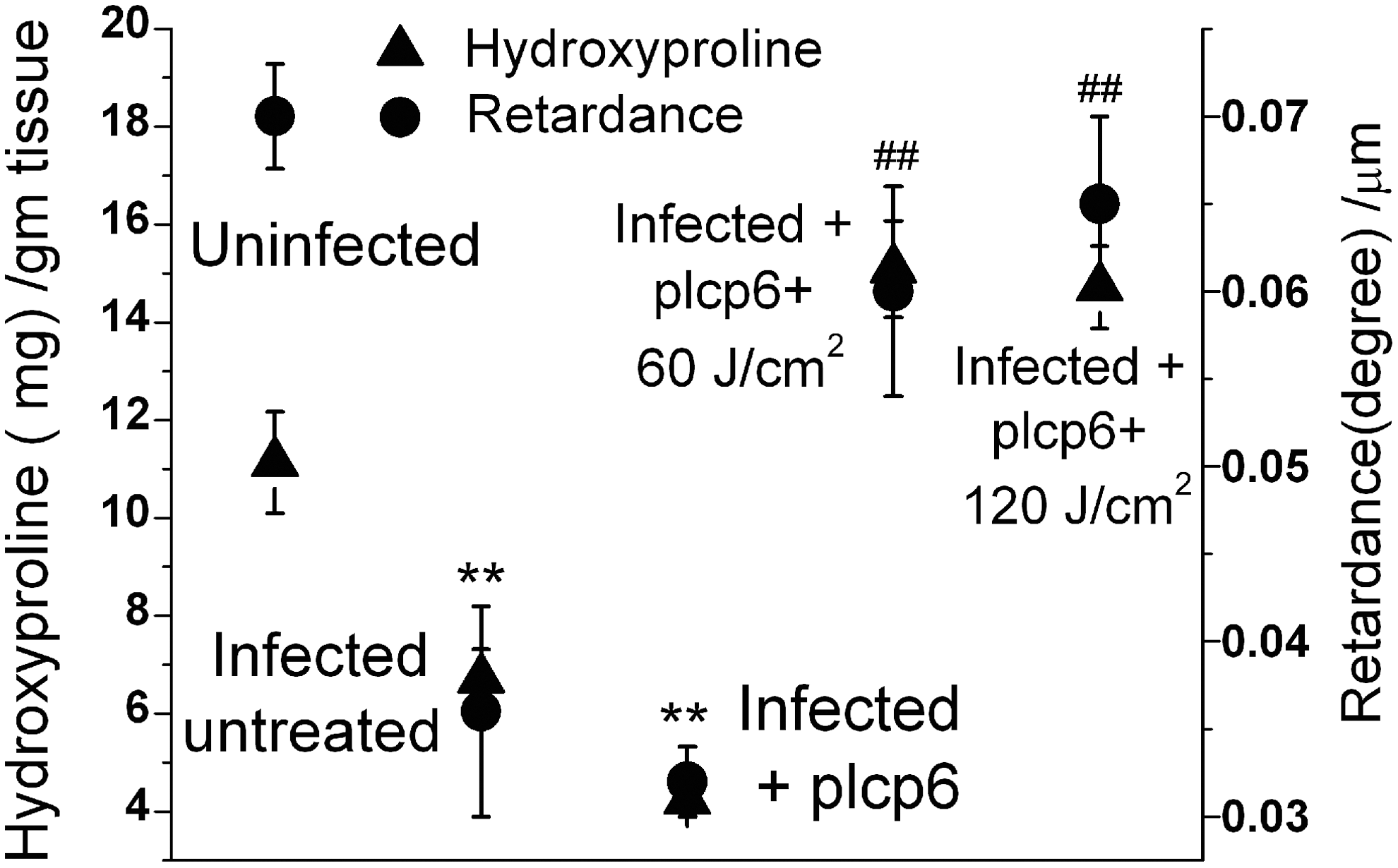
Photodynamic treatment induced changes in hydroxyproline content and calculated phase retardation (mean±SD) of methicillin-resistant Staphylococcus aureus (MRSA) infected wounds on day 18. **p<0.05 compared with uninfected wounds. ##p<0.05 compared with untreated and pl-cp6 treated.
Optical imaging of PAO-infected wounds subjected to PDT and comparison with histology
In Figure 5A OCT, PSOCT, and histological images of the untreated and photodynamically treated PAO-infected wounds are shown. The OCT and PSOCT images of untreated and dark control wounds were almost similar, and showed the presence of thick crust, more signal poor regions indicative of infection induced edema, and lower retardance on days 7 and 14 (Fig. 5A a–f). On day 18, the phase retardance in untreated and pl-cp6 treated infected wounds was much lower (p<0.05, ANOVA) than that of uninfected wound. However, in photodynamically treated wounds (Fig. 5A g–l), re-epithelialization occurred much earlier and there was significant increase in the phase retardance (∼0.052 degree/μm). Histological analysis of photodynamically treated wounds shows lesser inflammatory cells, complete epidermis, and more compact dermis than infected dark control (Fig. 5 A m, n). The photographs of uninfected and PAO-infected (untreated and photodynamically treated) wounds at day 1 and 14 are shown in Fig. 5B. In conformity with PSOCT and histology data, faster closure was observed in wounds subjected to PDT.
Effect of APDT on MMP expression in PAO-infected wounds
PAO toxins are known to stimulate overproduction of MMPs, 15 which can degrade collagen. Therefore, we studied MMP expression in PAO-infected wounds. The results (Fig. 6) show that in the untreated infected wounds MMP-8, 9 protein levels were overexpressed. In the photodynamically treated wounds, however, MMP levels were reduced considerably (p<0.001).
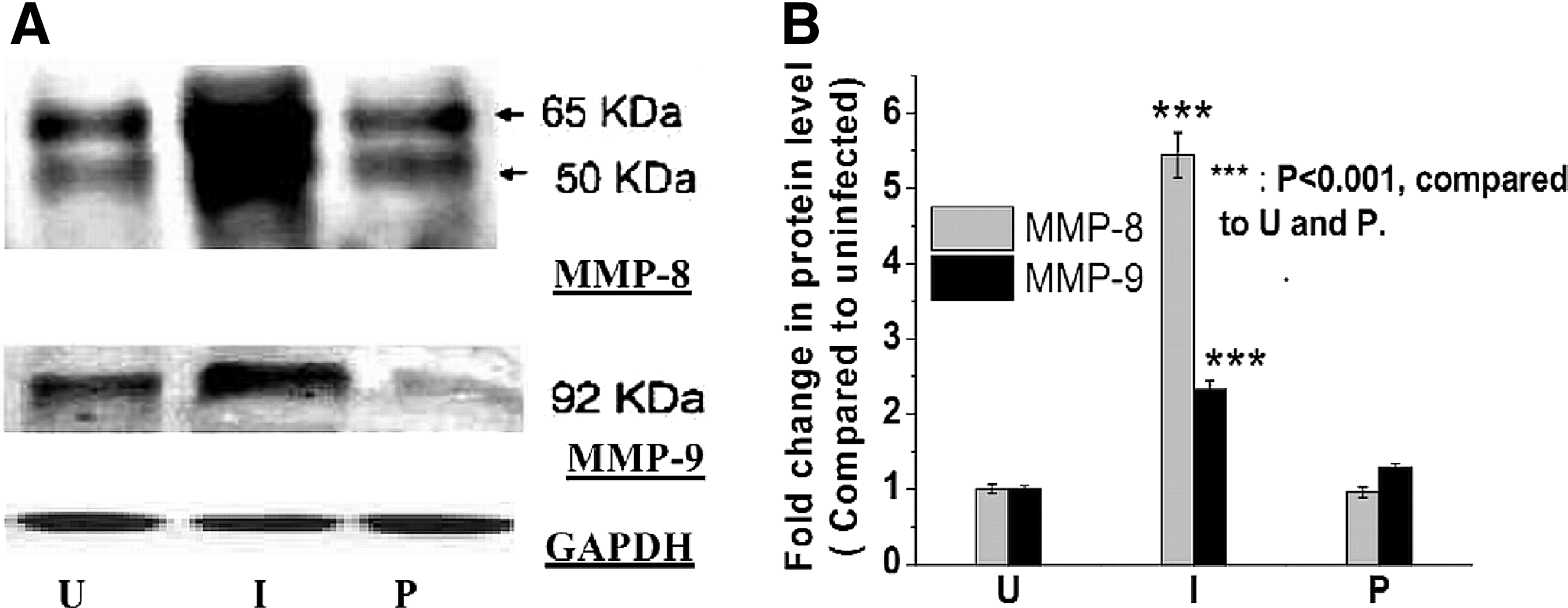
Effect of photodynamic treatment (PDT) on metalloproteinase (MMP) expression in Pseudomonas aeruginosa infected wounds on day 5.
Discussion
It is known that in bacteria-infected wounds, collagen remodeling is compromised because of the collagenolytic enzymes secreted by bacteria, 13 which in turn might stimulate collagenase 14,15 production by host cells. This affects collagen fibril arrangement and tensile strength during the scar maturation phase of the wound. Therefore, in order to assess the effect of an antibacterial therapeutic intervention in wounds more accurately, monitoring collagen remodeling is necessary.
Results presented in Figs. 2, 3, and 5A showed persistence of scattering poor regions and lower retardance in PSOCT images even during the 3rd week, indicating prolonged edematic and collagen degradation response caused by bacteria infection. 24 It is known that the toxins produced by S. aureus cause extensive host tissue damage, by eliciting either apoptotic response in epithelial cells, 28 or hyperinflammatory response. 29,30 There may also be S. aureus infection induced increased interstitial MMP 16,31 production by inflammatory cells. Similarly, PAO elastase can cleave directly to collagen type III 13 of the early granulation tissue. PAO infection can stimulate local overproduction of proinflammatory mediators such as tumor necrosis factor (TNF)-α 19 and pro-MMP. 15 TNF-α inhibits collagen I synthesis, 32 and promotes higher MMP production. 33 MMP-8 degrades type I collagen into gelatins that are substrates for MMP-9. 16 Excess MMP-9 (Fig. 6) leads to reduced collagen IV at the leading edge of the epithelial tongue. 34 Therefore, MMP-8, 9 overexpression in infected wounds delays collagen restoration.
The results presented in Figs. 3 and 5A show that collagen remodeling in photodynamically treated MRSA and PAO-infected wounds was faster than for wounds treated with pl-cp6 in the dark. The faster collagen remodeling in mice wounds was confirmed by hydroxyproline measurement (Fig. 4), histology, and PSOCT measurements (Figs. 3 and 5A). Increased (approximately threefold) retardance, more ordered collagen fibrils, and higher hydroxyproline content (approximately four times) in photodynamically treated MRSA-infected wounds compared with untreated infected wounds confirmed the faster collagen remodeling (Fig. 4). Similarly, significant increase in retardance and parallel collagen fibers in PAO-infected wounds following PDT also suggests better scar maturation. The faster recovery in treated wounds may be because of the abrogation of hyperinflammatory response and collagen degradation induced by bacterial toxins. 14,19 Our previous study has shown that APDT mediated by pl-cp6 reduces expression of IL-6 (approximately fivefold) and TNF-α (approximately fourfold) in PAO-infected wounds, which may be responsible for the faster collagen restoration by lowering the MMP production (Fig. 6).
The results of our study show that phase retardance of wounds, like wound tensile strength, 20 increases with post-wounding time. As both wound tensile strength 20 and birefringence 35 reflect collagen arrangement, PSCOT-based retardance can be a good indicator of tissue tensile strength and wound repair. In contrast, hydroxyproline level, beyond a certain time point, does not increase along with wound tensile strength, 20 and in several situations, although the hydroxyproline content of wounds subjected to therapeutic intervention may be the same, the tensile strength may differ significantly. 36 Hence, predicting an outcome based on hydroxyproline level may be erroneous.
Conclusions
Collagen remodeling response, post-APDT, in excisional wounds of mice infected with antibiotic-resistant and virulent strains of bacteria, could be quantified by PSOCT-based retardance measurements. The data on retardance were in accordance with the changes observed in MMP-8, 9 expression, hydroxyproline content, and histology. This suggested that topical APDT induced by pl-cp6 and red light expedites collagen restoration in bacteria- infected wounds of mice by attenuating collagen degradation caused by bacterial infection. It benefits wound repair in bacteria-infected wounds by significantly enhancing epithelial layer migration, hydroxyproline content, and collagen fibril arrangement.
Footnotes
Author Disclosure Statement
No competing financial interests exist.