
Abstract
Introduction
T 1. Compound odontomas, consisting of malformations with representation of all dental tissue types, and exhibiting organized distribution, in which numerous tooth-like structures known as denticles are present 2. Complex odontomas, that is, malformations in which all dental tissues are likewise represented, but that show a disorganized distribution.
2
–5
Other types of odontomas also sometimes occur, presenting combinations of the characteristics of compound and complex odontomas (i.e., mixed odontomas).
Epidemiologically, compound odontomas are the most frequent type, and in different reports account for 22–67% of all odontogenic maxillary neoplasms. 6,7 With regard to location, most occur in the areas around the maxillary incisors and canines, followed by the antero- and posteromandibular regions. Complex odontomas are more often found in the vicinity of the second and third mandibular molars. 7 The prevalence of these hamartomatous lesions is higher in children and adolescents, with little difference between the genders. 8 Clinically, the growth of both subtypes is typically slow and painless, 2 –5 often associated with alterations in the eruption of permanent or deciduous dentition.
These lesions are usually discovered on the occasion of routine radiological studies (panoramic and/or intraoral radiographs) to evaluate the cause of delayed tooth eruption. Radiologically, odontomas are usually unilocular and contain multiple radiopaque, miniature tooth-like structures known as denticles; alternatively, they may appear as a dense radiopaque mass surrounded by a thin radiotransparent rim. 6 The lesions tend to be located between the roots of erupted teeth, or between the deciduous and permanent dentition. 8 Confirming diagnosis through histological examination, odontomas are composed of various dental tissue formations, including enamel, dentin, cement, and, sometimes, pulp.
Conventional surgery is considered to be the treatment of choice for odontomas, although lasers have also been successfully used in treating cutaneous and mucosal lesions. 9,10 It is known that the erbium-doped yttrium aluminum garnet (Er:YAG) laser, emitting at a wavelength of 2940 nm, and the chromium-doped yttrium scandium gallium garnet lasers (Er,Cr:YSGG) laser, emitting at a wavelength of 2780 nm, possess suitable properties for treating not only soft but also hard tissues, because of their characteristic wavelengths, which are to a great extent absorbed by water. 11,12 These laser systems provide the capability to ablate bone effectively, without producing major thermal side effects to adjacent tissues. In 1983, Eriksson et al. 13 introduced the concept that, during bone surgery using rotary instrumentation, the tissue temperature should not rise >47°C for 1 min, in order to avoid permanent cellular damage. The prime mode of ablative laser–tissue interaction is photothermal, and this concept may be expected to apply equally to the use of lasers. The damaging effects can be minimized by using the laser in a pulsed emission mode, and by applying cooling systems in the form of water or air spray. It is also reported that the Er:YAG laser, set at operating parameters of 5.0 Watts Average Power and 20 Hz, provides good dental hard tissue cutting capacity without causing carbonization; it is further said to possess significant antimicrobial activity. In a recent animal study, Mizutani et al. 14 demonstrated the effective and safe application of the Er:YAG laser for granulation tissue removal and root surface debridement, finding that new bone formation was promoted at the periodontal surface.
The aim of this retrospective study was to evaluate the efficacy of conventional surgery and erbium laser treatment (Er:YAG laser and Er,Cr:YSGG laser) in managing odontomas, in terms of clinical outcome, and to assess postsurgical pain.
Materials and Methods
All odontoma patients had been referred to the Department of Oral Pathology, San Martino Hospital, Genoa, Italy by their general dental practitioners, between 2007 and 2012. In most cases, the lesion had been detected on routine radiographs, or during investigation of disturbances of tooth eruption or bone swelling. All 35 cases included in this series were diagnosed based on clinical history, physical examination, radiological studies (panoramic, occlusal and periapical radiographs) (Figs. 1 and 2) and histological study of the surgical specimen. Surgery, whether conventional or laser assisted, was performed via the intraoral approach. Fifteen patients were treated with Er:YAG 2940 nm (Fidelis Plus II–Fotona, Slovenia, EU), 10 with Er,Cr:YSGG laser 2780 nm (Waterlase, Biolase Inc., CA) and 10 with conventional surgery. In cases in which the lesion was of considerable size and closely associated with a permanent tooth that had failed to erupt, the lesion and the tooth were removed. Other teeth, which could be repositioned in the dental arch, received orthodontic treatment. In almost all cases, filler material (bone mineral) was required to repair bony defects for single lesions; in cases of multiple lesions, guided bone regeneration techniques were used to prevent formation of a significant bone defect, through the additional use of a resorbable membrane after lesion removal.

Pantographic radiograph shows a collection of tooth-like structures and apical deciduous canine. The structures have disrupted eruption of the permanent canine.

Endoral radiograph shows a small collection of tooth-like structures in the anterior maxilla.
The visual analog scale (VAS) score was employed to assess pain intensity after treatment; this scale has been shown to be a reliable and valid measure of pain, and consists of a standard 10 cm line with verbal anchors indicating “no pain” at 0 cm and “severe pain” at 10 cm. 15
Conventional surgical procedure
The procedure consisted of raising a mucoperiosteal flap, making an ostectomy to reveal the lesion, resecting the odontoma and, if necessary, extracting the affected tooth. All phases of conventional surgery (mucosa incision, osteotomy, resection) were performed under local anesthesia, making an incision with a 15c scalpel blade and raising a full-thickness flap, after which an osteotomy was performed with the traditional technique; the high-speed rotary handpiece and burs employed were of tungsten carbide. A no. 35 round bur manufactured by Komet (Milan, Italy) was used initially, and subsequently the smaller no. 23 bur was used to remove the odontoma.
The lesion was then removed, in all cases without difficulty. The flap was sutured with interrupted sutures of 3/0 braided silk thread, needle v-5 Ethicon, and with 3/0 PTFE suture thread, needle 3/8 Gore-Tex®. The excised tissue was sent for histopathological study to confirm diagnosis.
Laser surgery procedure
In cases treated by laser, surgery was likewise performed with the patient under local anesthesia. A full-thickness mucoperiosteal flap was raised, after which laser osteotomy was performed (Fig. 3). The osteotomy area and the surrounding zone were decontaminated with laser photonic energy, where possible. Decontamination and biostimulation were performed with the laser at a power setting of 50 mJ, 15 Hz, variable square pulse (VSP) mode, handpiece R07-Ti, fiber 800 μm, 60 sec, for three applications, with fluence ranging from 27 to 54 J/cm2 and irradiance from 0.15 to 0.30 W/cm2.

Pantographic radiograph post-surgery.
In all cases, the lesion could then be removed without difficulty. The flap was sutured in place using interrupted sutures of 3/0 braided silk thread (needle v-5 Ethicon) and with 3/0 PTFE suture thread (needle 3/8 Gore-Tex®). The excised tissue was sent for histopathological study to confirm diagnosis.
Laser treatment protocol
With the patient under local anesthesia (2% carbocaine and 1:100.000 adrenaline) a full-thickness mucoperiosteal flap was raised. Laser characteristics and settings were as follows: • Er:YAG 2940 nm, pulse width 100 msec, curved handpiece, truncated cone HPX tip, 400 μm with the following parameter settings to open the mucoperiosteal flap: power 250 mJ, frequency 12 Hz, air/water spray 80 mL/min. The parameters for each pulse are calculated as follows: spot size=r
2
×3.14=0.02×0.02×3.14=0.00125 cm2, peak power=0.25 J/0.0001 sec=2550 W, fluence single pulse=0.25 J/0.00125 cm2=200 J/cm, PD single pulse=2550 W/0.00125 cm2=2040000 W/cm2. • To treat hard tissue: osteotomy and removal of the lesion, with HPX 600 μm tip, power 400 mJ, frequency 15 Hz, air/water spray 100 mL/min. The parameters for each pulse are calculated as follows: spot Size=r
2
×3.14=0.03×0.03×3.14=0.0028 cm2, peak power=0.4 J/0.0001 sec=4000 W, fluence single pulse=0.4 J/0.0028 cm2=142.8 J/cm2, Power Density (PD) single pulse=4000 W/0.0028 cm2=1428571 W/cm2. • Er, Cr :YSSG, laser 2780 nm to open the mucoperiosteal flap: power 2.5 W, frequency 15 Hz, air/water spray 40 mL/min, mode 600 μm, MG6 tip, pulse width 750 μsec variable. The parameters for each pulse are calculated as follows: spot size=r2
×3.14=0.02×0.02×3.14=0.00125 cm2, peak power=0.25 J/0.0001 sec=2550 W, fluence single pulse=0.25 J/0.00125 cm2=200 J/cm, PD single pulse=2550 W/0.00125 cm2=2040000 W/cm2. • To treat hard tissue: osteotomy and removal with 600 μm MG6 tip, length 6 mm, power 3.5 W, frequency 20 Hz, 55% air/45% water spray, H (hard tissue) mode, pulse width 190 μsec variable. The parameters for each pulse are calculated as follows: spot size=0.0028 cm2; power peak=0.167 J/0.00019 sec=879 W fluence single pulse=0.167 J/0.0028 cm2=59.6 J/cm2, PD single pulse=879W/0.0028 cm2=313928 W/cm2.
Postoperative treatment and follow-up for both patient groups
Pharmacological treatment comprised administration of amoxicillin 1 g capsules, two capsules per day for 5 days. In cases of intolerance to penicillin, spiramycin (3,000,000 U capsules, two capsules per day for 5 days) or azithromycin (500 mg capsules, one capsule per day for 3 days) were prescribed. For patients who were particularly sensitive to pain, an analgesic was administered: ibuprofen 200 mg two capsules per day for 3 days. Most patients treated by conventional surgery requested the analgesic, whereas no analgesic was requested in the majority of cases treated by laser.
Patients were instructed to use gel-bearing trays to apply 0.2% chlorhexidine-based gel to the treated zone, for 5 min twice daily for as long as the sutures remained in place. Patients were monitored through orthopantomography (Fig. 4), preoperative and postoperative intra-oral prescription, repeated at 3 months, 6 months, and yearly after surgery.
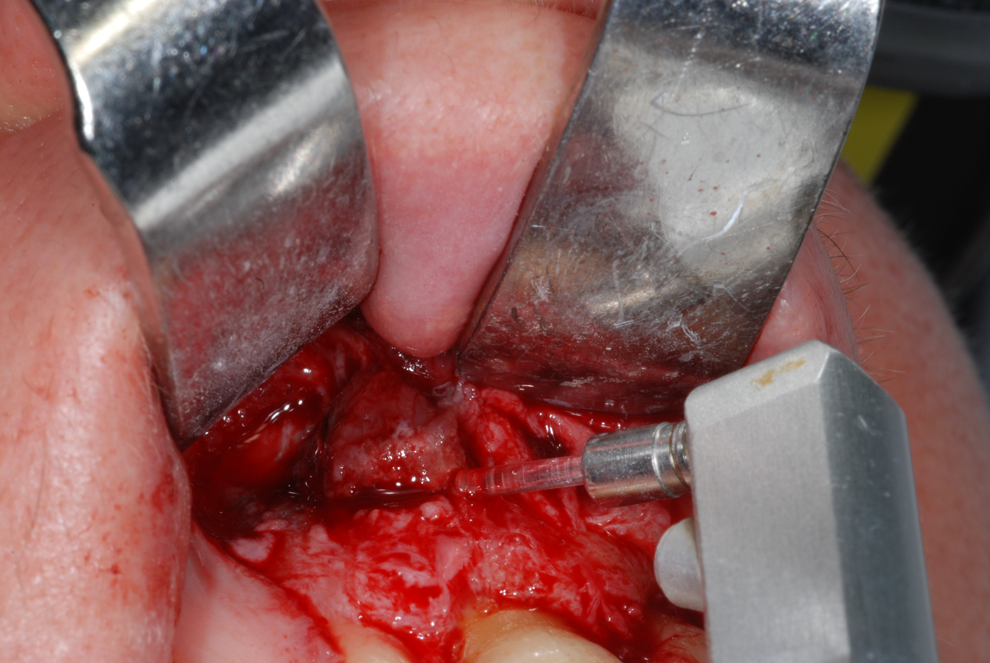
Cinical view during surgical management with Erbium laser.
Pathological findings
Biopsy specimens were fixed in 10% buffered formalin and embedded in paraffin wax, sections (4 μm thick) were prepared and stained with hematoxylin and eosin (H&E). In all cases, the histopathological specimen allowed diagnosis to be confirmed, as follows: 1. Complex odontoma, showing haphazardly arranged hard tissues of tooth-like dentin and globules of cementum-like material, with primary or immature dentin as the predominant component, although enamel was also present (Fig. 5). 2. Compound odontoma, showing a mixture of dental hard tissues resembling a tooth, dentin being the predominant tissue, with an enamel matrix, cementum, and fibrous connective tissue surrounding the denticles (Fig. 6).
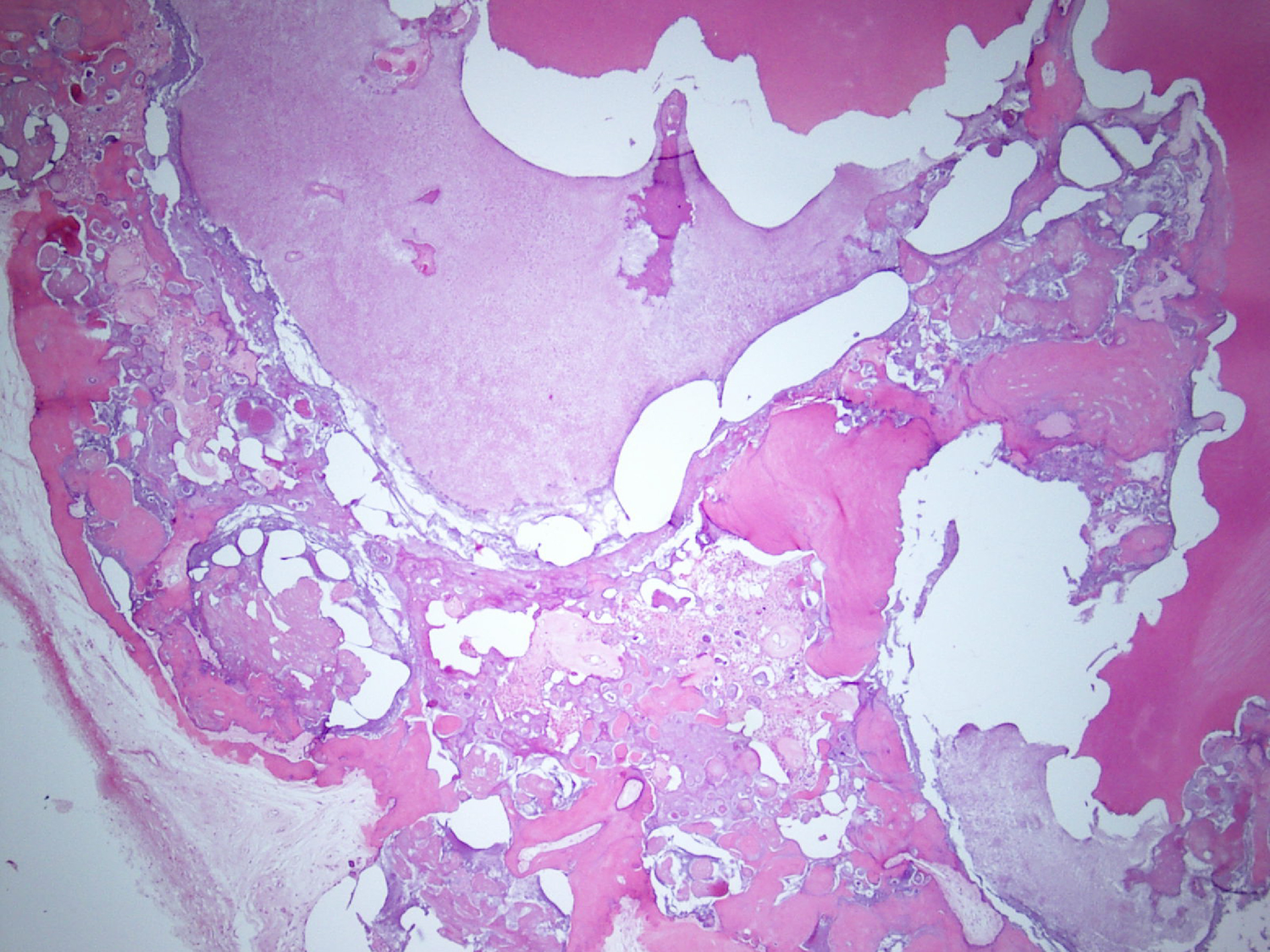
Photomicrograph shows different tissues such as pulp, dentin, enamel, exhibiting variable organization. (Hematoxylin and eosin original magnification 10×).
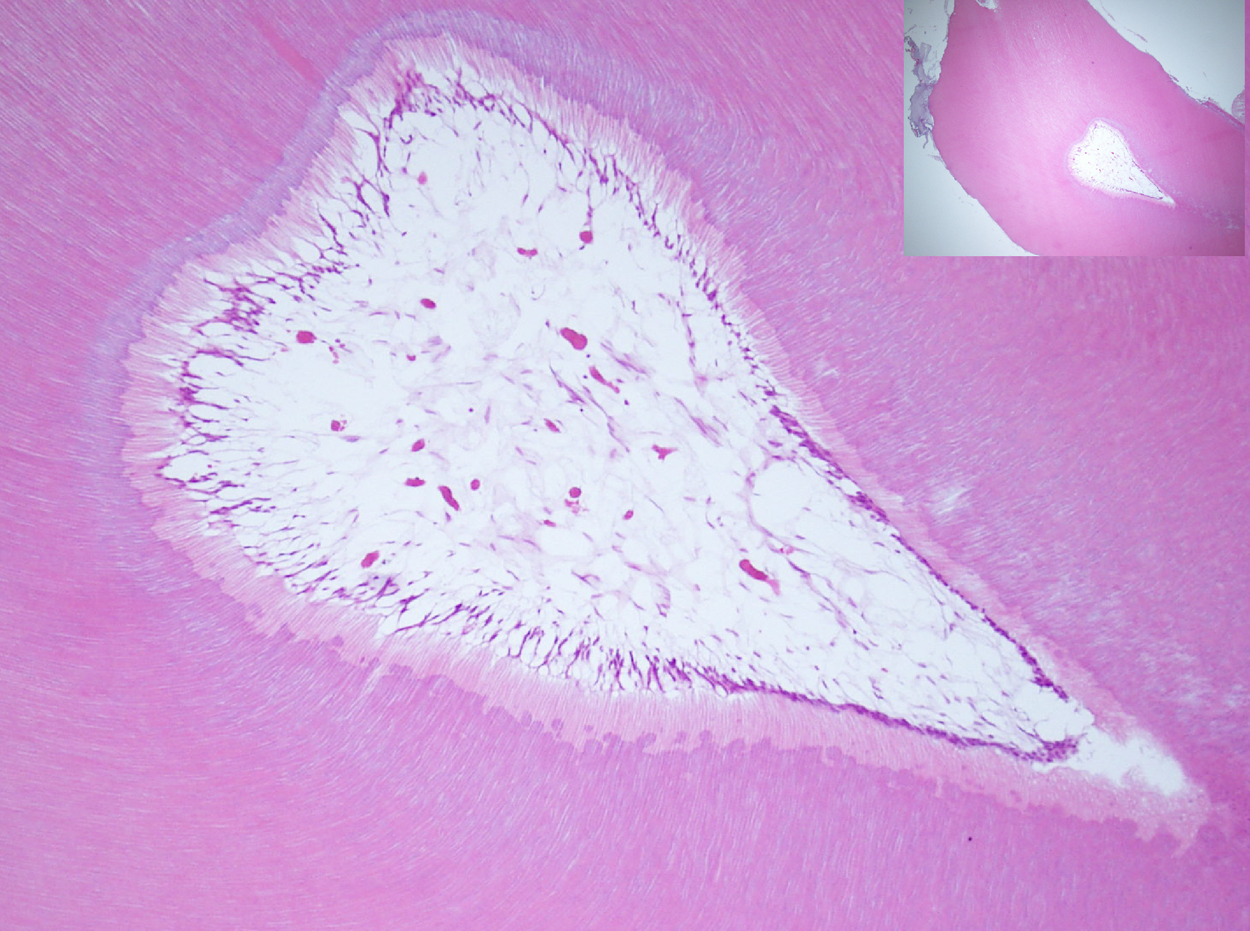
Photomicrograph shows pulpal tissue adjacent to predentin and mature dentin. The inset highlights a relationship very similar to that of normal teeth (hematoxylin and eosin, original magnification 40×).
Pain assessment
Pain was assessed using a 10 point pain VAS. Low pain was defined as a VAS score of 0–3, moderate pain as 4–6, and severe pain as 7–10. Patients were questioned at the start of treatment and were advised to notify physicians of any changes in their pain at other times. The VAS scale was determined on days 3 and 7 post surgery.
Statistics
The Shapiro–Wilk normality test was applied to assess the distribution of all continuous variables. Correlations between VAS scores and other variables were evaluated using nonparametric univariate analysis. In particular, the Mann–Whitney U test and the Kruskal–Wallis test were applied to check any statistically significant differences in VAS scores between any two subgroups (gender, tumor location, type of surgery) or set of subgroups (type of tumor).
Spearman's rank correlation test was applied to evaluate the degree of correlation between continuous variables (VAS and age). All analyses were computed using SPSS v.20 (IBM Corp.). A value of p≤0.05 was considered statistically significant.
Results
The VAS scores did not show any statistically significant difference for tumor localization (p=0.11), patient gender (p=0.51) or tumor type (p=0.55). No correlation was found between VAS score and age (p=0.86).
As shown in Fig. 7, there was a statistically significant difference (p=0.016) in VAS score between patients treated with traditional scalpel surgery (median=4.00) and patients undergoing laser surgery (median=3.00).
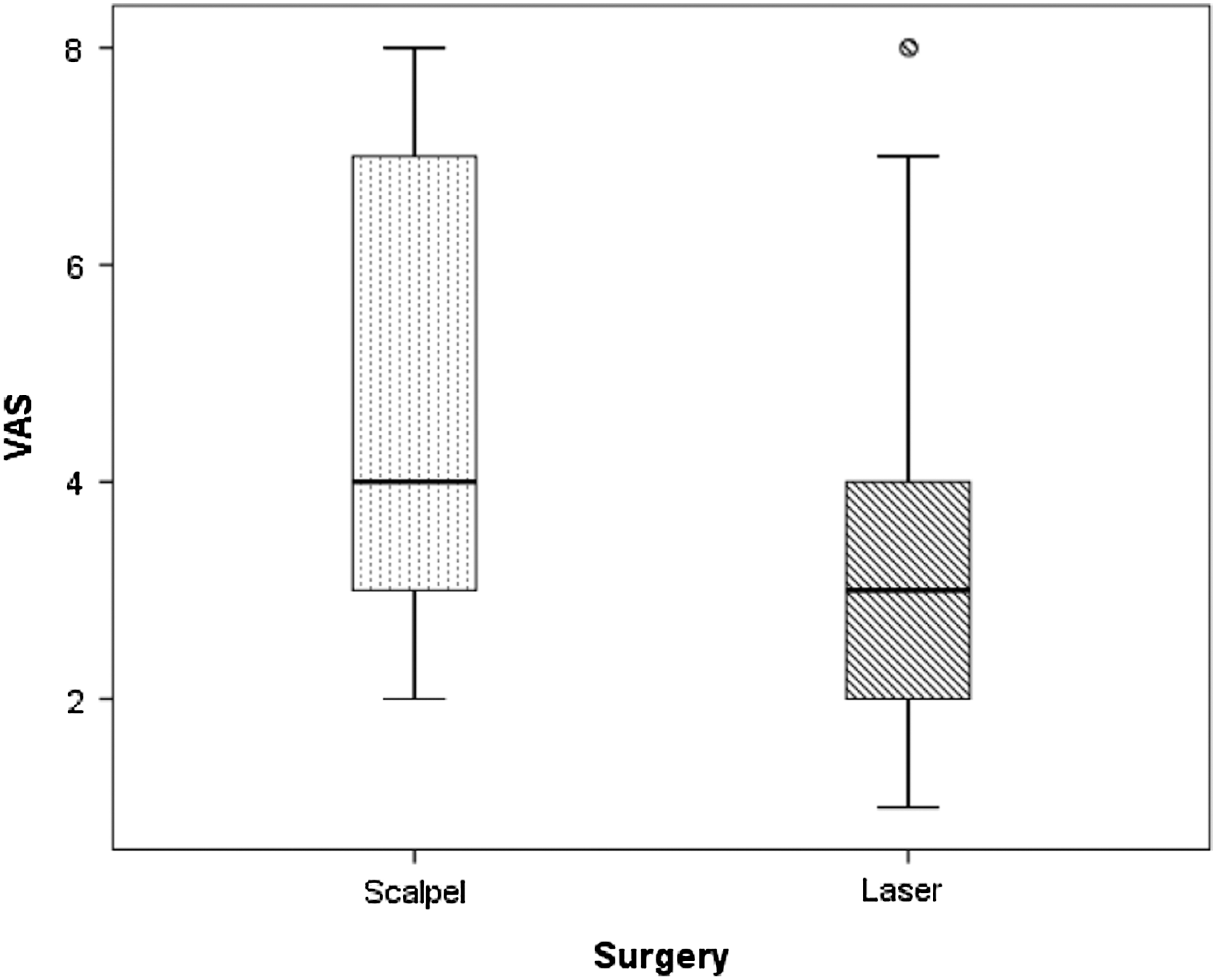
Difference in visual analog scale (VAS) score between scalpel surgery and laser surgery.
Of the 35 cases in this series (Table 1), failure only occurred in one case, which had been treated by conventional surgery. At 3 year follow-up, there was one case of relapse, which was resolved by surgical retreatment. At 5 year follow-up, there were no relapses. In all other cases healing was excellent.
VAS, visual analog scale; IQR, interquartile range.
Fifty-four percent of cases were diagnosed as compound odontomas, 32% as complex odontomas, and 14% as mixed odontomas. Of all cases, 24 affected the maxilla (69%) (21 anterior, 3 posterior), and 11 the mandible (31%) (5 anterior, 6 posterior). The anterior portion of the jawbones was the most common location (60% of all cases).
Only in 10 cases was orthodontic treatment applied, in order to displace an impacted permanent tooth to its normal position, applying traction to the unerupted tooth with an arch and a direct-bonding system. Acceptable occlusion was achieved in these 10 cases 5 years after surgery.
In patients who had undergone laser treatment, no postoperative complications were noted at 2 and 5 year checkup, and there were no recurrences.
The VAS scores were as follows: for patients treated with laser, the range of VAS scores was min 0.0, max 3.0; median VAS score (without analgesics) was 3.0 (min 0.0, max 4.0); for patients treated by conventional surgery, median VAS score was 4 (min 0.1, max 6.0).
Discussion
Odontomas are relatively common benign hamartomatous malformations that are asymptomatic and often only diagnosed via routine radiological studies. In some cases, there are signs such as delayed tooth eruption, or patients may report pain and present suppuration. 16,17 Approximately 70% of cases are associated with other conditions, including tooth impaction or malposition, as well as malformation, resorption, and devitalization of adjacent teeth. 8
It is reported that the ratio of compound to complex odontomas is 2:1. 1 –5,7,18 Compound odontomas are usually located in the anterior maxilla, either above the crowns of unerupted teeth or between the roots of erupted teeth. Conversely, complex odontomas are generally found in the posterior mandible, above impacted teeth, and may achieve several centimeters in size. Of our 35 cases, 18 were compound and located in the maxilla (51%) (15 anterior, 3 posterior), and 7 were complex and located in the mandible (20%) (2 anterior, 5 posterior). This coincides with reports that these lesions appear more frequently in the maxilla, 4,7,8,18,19 although some sources make no distinction between the two jaws. 7,20 –22 In our series, the average age at onset of these tumors was in the second decade of life for both complex and compound odontomas, the mean age (14.2 years) was in agreement with most other reports. 3 –5,7,8,12,19
Some studies have found a correlation between patient age and type of odontoma, with compound lesions being more frequent in younger patients, whereas complex odontomas appear to be more common in older patients. 7 Further, studies of the relation between patient age and location suggest that older individuals are more likely to present odontomas in the molar region. 19 In our series, no significant relationship was found between patient age and odontoma type.
In order to diagnose odontomas, clinical data must be correlated with radiological findings and histological evaluation. It is reported that computed tomography and magnetic resonance imaging are superior to plain radiography, when establishing the intraosseous extent of the tumor, cortical perforation, and soft tissue involvement. 21
There is no general agreement about the best management approach for impacted teeth associated with odontomas. Morning 22 reported that ∼75% of impacted teeth related to odontomas erupt after removal of the odontoma, indicating that careful evaluation should be made before extracting such an impacted tooth. However, impacted teeth are frequently reported to be removed together with odontomas. 23,24 Treatment options also include simple observation with periodic clinical and radiological checkup, to evaluate the development of these teeth. 25,26
A number of different techniques have been proposed for osteotomy: 27 –31 ultrasonic, CO2, high-speed rotary handpiece, piezosurgery, and the erbium laser. The laser technique has a number of advantages, including precision, conservative action with less bone destruction, lack of vibrations, decontamination, and reduction of postoperative edema. However, there are also some disadvantages, including lengthening the time required for surgery, and the fragility of the surgical tips, which can easily break leading to higher costs. In our cases treated by conventional surgery, the osteotomy was performed traditionally, using a high-speed rotary handpiece.
In our study, 25 cases were treated with the Er:YAG and Er,Cr:YSGG lasers. The good ability of these instruments to ablate bone effectively without producing thermal side effects to adjacent tissues, together with the significant bactericidal 11 and detoxification effects they produced, 32 led to a good treatment outcome, and were helpful in the healing course of the odontomas.
The VAS score did not show any statistically significant difference correlated to tumor localization (p=0.11), gender of the patient (p=0.51), or tumor type (p=0.55). No relationship was found between VAS score and age (p=0.86).
A statistically significant difference (p=0.016) in VAS score was observed between patients treated with traditional scalpel surgery (median score=4.00) and patients who had undergone laser surgery (median score=3.00).
Orthodontic therapy was applied in 10 cases, to guide the impacted tooth into a normal position after excision of the odontoma, applying traction to the unerupted tooth by means of a vestibular arch and a direct bonding system, to achieve an acceptable occlusion. In eight cases, either because of too close contact with the odontoma, or because the tooth could not be preserved during removal of the lesion by laser or scalpel, the tooth was extracted together with the lesion. In 20 cases, a space maintainer was needed to reposition the impacted tooth and facilitate its eruption; after 8–12 months, the tooth had reached the occlusal plane without the need for orthodontic traction.
The result was a satisfactory postoperative occlusion and good clinical outcome in all cases, including those receiving orthodontic therapy: cases in which the impacted permanent tooth was preserved, those in which a space maintainer was applied in expectation of the tooth's eruption, and also those in which extraction was necessary because of close contact with the hamartoma.
Conclusions
In conclusion, this study has validated an innovative technique, and it may be said that the protocol offers significant benefit to patients. It does not require any specialized staff, reduces costs by eliminating or reducing the use of analgesics, does not greatly increase treatment time compared with conventional treatment, and maintains an excellent clinical outcome.
Footnotes
Author Disclosure Statement
No competing financial interests exist.