
Abstract
Introduction
I
In addition to such chemical substances, lasers are being used as a coadjuvant tool in endodontic therapy. Laser applications in endodontics have been reported, including their use in pulp diagnosis, investigating dentinal hypersensitivity, pulp capping and pulpotomy, sterilization of root canals, root canal shaping, obturation, and apicoectomy. 6 It has been shown that new lasers with a wide range of characteristics – Nd:YAG, 810 nm diode, Er: YAG, and CO2) – are effective in smear layer elimination, antibacterial activity, and sealer adhesion. 7 The Er:YAG laser was found to be more effective for debris removal, producing a cleaner surface with a higher number of dentinal tubules than other laser treatments. 4,8 Nd:YAG laser-irradiated samples presented melted and recrystallized dentin and smear layer removal. 9 Both Nd:YAG and diode laser were found to be more effective when compared with a non-lased control group in advancing the bond strength of epoxy resin-based sealer to dentin. 10
In improving the quality of root canal obturation, lasers have the potential to enhance the adhesiveness of root canal sealer to dentin surface. 10 Haragushiku et al. 11 investigated the influence of different surface treatments on the adhesion of endodontic sealers. They stated that highest adhesion values were observed with AH Plus when the specimens were treated with Er:YAG laser and 17% EDTA plus Cetavlon (EDTAC). Moura-Netto et al. 12 reported that Nd:YAG laser irradiation caused significantly less leakage in the apical third than in the untreated group. The lower level of apical leakage could be the result of morphological changes on the apical intraradicular dentin surface caused by the Nd:YAG laser. Some authors have compared the dentin pretreatments that are performed with a laser and irrigating solution. They reported that citric acid irrigation revealed higher bond strength values when compared with Er:YAG laser pretreatment. 13
Selection of the adequate root canal filling material is another important element of endodontic therapy. 11 Epoxy resin sealers have been used because of their reduced solubility, 14 apical seal, 15 and microretension to root dentin. 16 AH Plus a hydrophobic epoxy resin-based root canal sealer penetrates deeper into these irregularities because of its high flow rate and longer setting time. 17 Moreover, recently, methacrylate resin endodontic sealers have been developed. 18 EndoREZ is a hydrophilic methacrylate resin sealer whose sealing properties have been used to penetrate dentin tubules, creating resin tags. 19
Developments in adhesive technology have consolidated the research to minimize apical and coronal marginal leakage by improving sealer adhesion to root canal walls, and thus decrease the tendency of root-filled teeth to fracture. 20 Therefore, the aim of this study was to evaluate the effects of two laser systems (Er:YAG and Nd:YAG) and chelating agent EDTA before obturation on the bond strengths of resin-based root canal sealers AH Plus and EndoREZ for human root canal dentin using the pushout test. This study was performed on the apical, middle, and coronal thirds of the roots, to obtain an adequate assessment.
Materials and Methods
Tooth selection
This study was approved by the Ethics Committee of the Dentistry Faculty of Ataturk University in Erzurum, Turkey. A total of 100 extracted human maxillary canines with a single canal were used in this study. Teeth with calcification, an immature root apex, or resorption were discarded. Before performing the experiment, the teeth were stored in distilled water at room temperature.
Preparation of specimens
The teeth were sectioned transversally at the cementoenamel junction using a water-cooled diamond disk (Diamond disk superflex 910S/220, North Bel, İtaly) to obtain roots with a minimal length of 14 mm. Each root canal was checked for patency using a size 10 K-file (FKG, Dentaire, La-Chaux-de-Fonds, Switzerland) until the file was seen at the apical foramen. Working length was determined to be 1 mm short of patency length. The teeth were prepared using a K-file up to size 60 at the working length. A step-back preparation with size 70 and 80 K-files, and for coronal preparation, size 2, 3, 4, and 5 Gates-Glidden drills, were used to complete the canal instrumentation. Root canals were irrigated with 3 mL 5% NaOCl at each change of instrument.
Surface treatments and obturation
After sample preparation, the roots were randomly divided into four main groups according to the dentin surface treatments. Each group had two subgroups according to root canal sealer used, and a total of 8 groups were obtained (n=12). The rest of the roots were seperated for scanning electron microscopy (SEM) analysis.
• Group I served as a control and was irrigated with 3 ml 5% NaOCl and 3 mL distilled water.
• Group II was irrigated with 15% EDTA solution 2 mm short of the apical foramen for 90 sec. Then, specimens were irrigated with 3 mL 5% NaOCl and 3 mL distilled water.
• Group III was irradiated with Er:YAG (Doctor Smile erbium and diode laser, Lambda Scientifica S.r.l, Vicenza, Italy) at a wavelength of 2940 nm, 240 mJ output, and 0.32 j/cm2 energy density. After the laser irradiation, roots were irrigated with 3 mL distilled water.
• Group IV was irradiated with an Nd:YAG laser (Deka Smarty A-10, Florence, Italy) at a wavelength of 1064 nm, 15 Hz repetition rate, 1.5 W output, and pulse energy of 100 mJ. After the laser irradiation, roots were irrigated with 3 mL distilled water.
Subgroups
1. Following irrigation, the roots were dried with sterile paper points (Aceonedent, Geonggi-Do, Korea) and obturated with AH Plus (Dentsply, De Trey GmbH, Konstanz, Germany) and gutta-percha.
2. Following irrigation, the roots were dried with one sterile paper point and obturated with EndoREZ (Ultradent, South Jordan, UT) and gutta-percha.
Er:YAG laser irradiation was performed with a sapphire tip 12 mm in length and 600 μm in diameter attached to the handpiece using apicocervical movements with spiral motion for 1 min (from the apical foramen to the canal entrance and back to the apical stop for 20 sec each). During laser irradiation, the specimens were irrigated with 20 mL distilled water. Nd:YAG laser irradiation procedure took place similarly to that for the Er:YAG groups, except for the lasing time. Irradiation was performed with a fiberoptic tip of 300 μm in diameter for 10 sec; then, irradiation was stopped for 15 sec for thermal rest. This procedure was repeated four times, giving a total exposure time of 40 sec. During laser irradiation, 2 cc/min water was applied through the canal orifices.
In all groups, the irrigation process was performed with 31 ga/27 mm Navi Tip sideport (Ultradent, South Jordan, UT) needles. The specimens were obturated immediately after the final irrigation. Root canal sealers were mixed according to the manufacturers' instructions. The sealer was applied to the canal with a Lentulo spiral (Kendo, Munich, Germany) attached to a low-speed handpiece to avoid bubble formation. After insertion of the size 60 gutta-percha cone, accessory cones were inserted with a stainless steel finger spreader (Mani Inc, Japan) according to the lateral compaction technique. In the EndoREZ groups, the cervical root thirds were photoactivated for 40 sec according to the manufacturers' instructions. In all groups, the excess cones were removed with a heated instrument and root canal entrances were sealed with a quick-setting temporary filling material. Then, specimens were immediately placed in conditions of 37°C and 100% humidity for a 1 week.
Applying the pushout test
To prepare the dentin disks, thee roots were fixed on acrylic plates and sectioned in a precision cutting machine (Precision Saw, Buehler, USA) at 275 rpm. Nine slices at 0.98±0.07 mm thick were obtained from each root (three slices per root third). The first slice of each third (a total of 288 slices) was selected for the pushout test. Slices were examined with a stereomicroscope (Novex, Arnhem, Holland) at 20× magnification, to determine the surface area of the obturation material of the slices. For the pushout test, two different parts were attached to the universal testing machine (Instron Corp, USA). One was a cylindrical plunger and the other was a plate with three holes. The cylindrical plungers performed according to the apical diameter of dentine disks (an apical third of 0.5 mm, a middle third of 0.7 mm, and a coronal third of 0.9 mm were used), whereas the performance of the holes was related to the coronal diameter of the dentin disks. The side with the smaller diameter of dentin disk faced upward and was aligned with the plunger, causing failure of the bond. The machine was set at a constant speed of 1 mm/min. The load was recorded when the obturation material was pushed and dislodged from the canal wall. The force needed to dislodge the obturation material was recorded in Newtons and transformed into megapascals by dividing the force by the bonded area. The bonded area of the obturation material was calculated using the following formulation, where h is the thickness of the dentin disk, r1 is the radius of the small end of the obturation, and r2 is the radius of the large end of the obturation:
The bond strength data obtained are shown in Tables 1 and 2; they were analyzed statistically using one way analysis of variance (ANOVA) and Tukey's post-hoc test (p<0.05).
Different letters in the same lines represent statistically significant differences.
Different letters in the same lines represent the statistically significant differences.
SEM analysis
To investigate the effects of dentin surface treatments, one specimen was randomly selected from each group. After washing with distilled water, specimens were dried with paper points. The specimens were stored in phosphate-buffered 3% glutaraldehyde solution for 24 h. They were sectioned along the long axis of the root with a diamond disk, and placed in ethanol solution for dehydration. Then, they were examined using a scanning electron microscope (EVO LS10, Zeiss, Oberkochen, Germany).
Results
The mean and standard deviation of pushout bond strength values are given in Tables 1 and 2. A statistically significant difference (p<0.05) was reported between the root canal sealers. AH Plus showed higher adhesion values than did EndoREZ. There was a significant difference among the dentine surface treatments (p<0.05). Er:YAG laser irradiation increased bond strength values compared with the control (NaOCl) group (p<0.05). However, no significant difference was obtained between Nd:YAG and the control (NaOCl) group or EDTA and the control (NaOCl) group (p>0.05). The apical and middle thirds of the specimens showed higher adhesion values when compared with the coronal third (p<0.05). In the apical and coronal thirds, AH Plus presented higher adhesion values than EndoREZ (p<0.05). However, in the middle thirds, there was no significant difference between root canal sealers (p>0.05). When the root canal was irradiated with the Er:YAG laser, AH Plus showed higher adhesion values than EndoREZ (p<0.05). There was no significant difference between the root canal sealers when using the other dentin surface treatments (p>0.05). In the AH Plus groups, there was a significant difference among the dentin surface treatments. The Er:YAG laser group presented better adhesion values than the other dentin surface treatments did (NaOCI, EDTA, Nd:YAG laser) (p<0.05). In the EndoREZ groups, the Nd:YAG laser group showed higher adhesion values than the Er:YAG laser group (p<0.05). No significant difference was found among the dentin surface treatments in the root canal thirds (p>0.05).
In the apical thirds for the AH Plus root canal sealer, the specimens treated with the Er:YAG laser presented higher adhesion values than did the control and Nd:YAG laser groups (p<0.05). For the EndoREZ root canal sealer, the specimens treated with the Nd:YAG laser showed higher adhesion values than did the control group (p<0.05).
In the middle thirds for AH Plus root canal sealer, the specimens treated with the Er:YAG laser presented higher adhesion values than did the control group (p<0.05). For the EndoREZ root canal sealer, the specimens treated with EDTA showed higher adhesion values than did the Er:YAG laser group (p<0.05).
In the coronal thirds for the AH Plus root canal sealer, the specimens treated with the Er:YAG laser presented higher adhesion values than did the other groups. For EndoREZ root canal sealer, there was no significant difference among the groups.
Based on SEM analysis shown in Fig. 1, the Er:YAG laser and EDTA solution used in this study had the capacity to expose the dentinal tubules and remove the smear layer. In the Nd:YAG and control (NaOCl) groups, the smear layer was not removed.
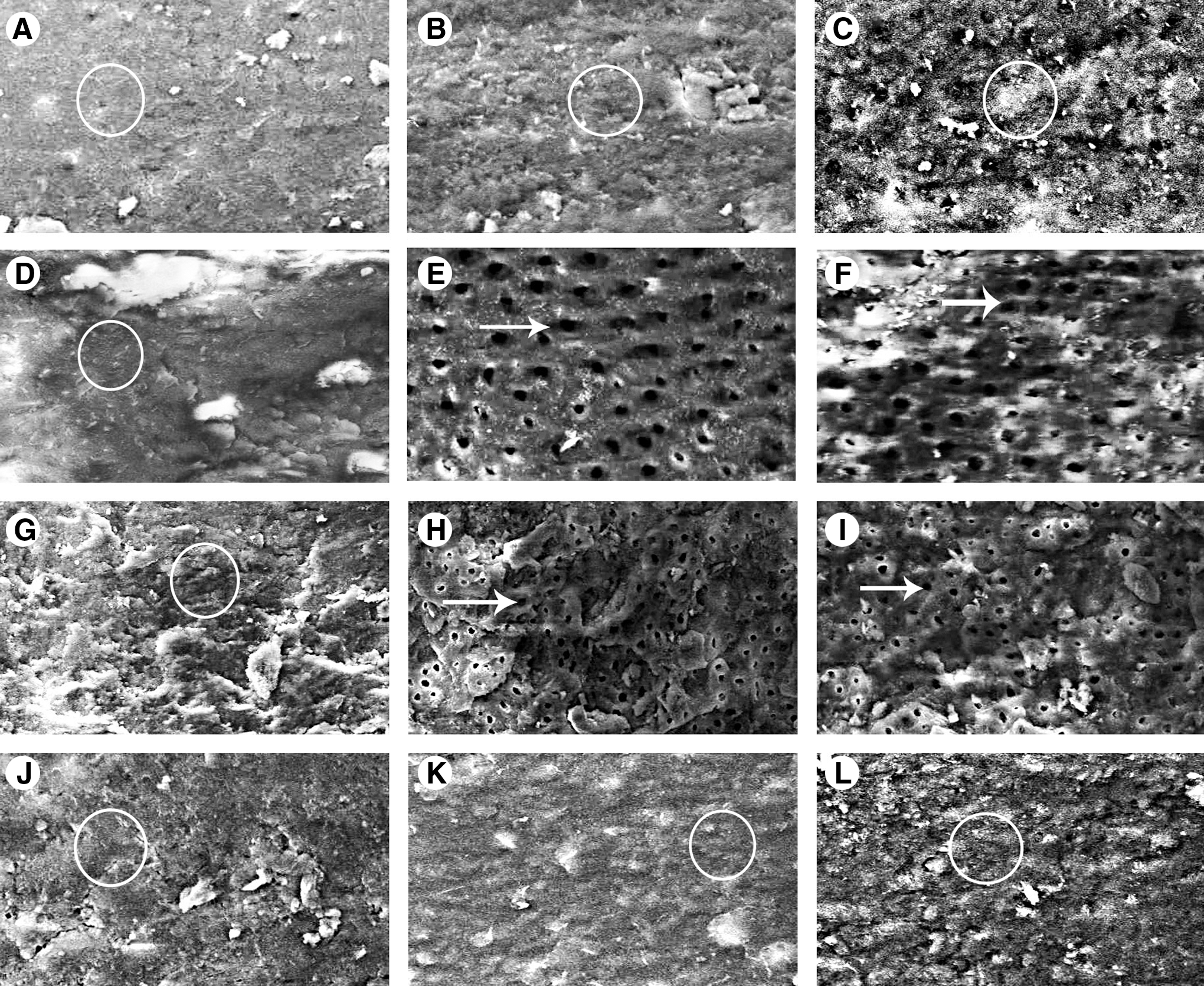
Scanning electron microscopic (SEM) images of
Discussion
Endodontic therapy is completed by hermetic sealing of the dentin structure after chemomechanical preparation. Obturation is performed with the association of a filling material and a root canal sealer. 21 Sealing ability is an important property of a root canal sealer; 22 therefore, an ideal root canal sealer must adhere both to the dentin and core material with no gaps, which is described as the adhesion process. 23 Sealer adhesion is related to root canal preparation, cleaning, and dentin surface treatment; the filling technique; and the type of sealer. 17 The adhesion capacity of root canal sealers to dentinal walls is anticipated as a result of high sealing property. This property should decrease marginal leakage in clinical cases. 23 The smear layer is a negative factor in root canal treatment that acts as a barrier between the sealing material and dentin, thereby inhibits the penetration of sealer tags into the dentinal tubules and reduces the adhesion of sealers. 2 Chemical substances such as EDTA, 1 citric acid, 24 and dental lasers such as the Er:YAG laser, 4,15 have been used to remove the smear layer. EDTA effects the tooth mineral matrix and helps to remove the smear layer during the biomechanic preparation of the root canal and increases penetration of root canal sealers into the dentinal tubules. 1 Er:YAG laser irradiation on the dentin surface removes the smear layer, exposes dentinal tubules, and creates a micromechanical retention surface. 15,25 Nd:YAG lasers are able to melt and resolidify the dentine walls, remove the smear layer, and reduce dentine permeability. 9 These effects on intracanal irradiation are similar to those of the diode laser and increase the sealing ability of endodontic therapy. 26 In the current study, to alter the surface conditions, to remove the smear layer and therefore to enhance the bond strength of resin-based root canal sealers, pretreatment with EDTA solution and Er: YAG and Nd: YAG lasers was presented.
Irradiation with the Er:YAG laser resulted in removal of the smear layer and morphological alteration of the dentinal tissue, as well as increase in the area of dentin with irregularities. 25,27 The presence of these irregularities on the surface of dentinal structure, which were formed by the surface treatments, could influence the mechanical adhesion. 13 In the present study, AH Plus root canal sealer presented higher adhesion values when irradiated with the Er:YAG laser compared with the other groups. In aggrement with the present results, Sousa-Neto et al. 27 reported that Er:YAG laser irradiation increased the bond strength values of epoxy resin-based root canal sealer. In our study, Er:YAG laser irradiation did not affect the adhesion values of EndoREZ root canal sealer significantly, compared with the control group. However, dentinal surface treatment with the Nd:YAG laser resulted in increased adhesion of the EndoREZ root canal sealer when compared with the other groups. The methacrylate-based root canal sealer EndoREZ requires opened dentinal tubules to improve its bonding to the dentinal walls. 28 Craters were observed in human dentine after irradiation with the Nd:YAG laser using SEM. 29 There has been no research on the relation with EndoREZ root canal sealer adhesion values performed in human dentin that was irradiated with Nd:YAG laser; therefore, this finding cannot be compared with previous results. Akisue et al. 13 compared the shear bond strength of resin-based root canal sealers with dentin pretreated with citric acid and Er:YAG laser. They obtained a mean bond strength of AH Plus 2. 12 MPa and EndoREZ 0.83 MPa when dentin was treated with Er:YAG laser. Our study reported a mean bond strength for AH Plus root canal sealer of 3. 34 MPa and for Endo REZ of 1.16 MPa when dentin was treated with Er:YAG laser. These results were comparable with previous studies. 30,31 Saleh et al. 23 found that smear layer removal with EDTA solution decreased the adhesion values of AH Plus and Apexit root canal sealers. The present study reported that pretreatment with EDTA solution did not enhance the bond strength values of resin-based root canal sealers compared with the control group. Generally comparing the dentin pretreatments, Er:YAG laser irradiation increased bond strength values compared with the control (NaOCl) group (p<0.05), but there was no significant difference between Nd:YAG and the control (NaOCl) group or EDTA and the control (NaOCl group (p>0.05)
Because of the temperature increase during the laser irradiation in the root canals, thermal damage to periodontal tissues was a major problem. 32 The application of water cooling during laser irradiation prevents the increase of temperature in the root canal, and decreases the possibility of thermal damages. 33 In previous studies, water coolant spray was used to avoid the harmfull effects of laser application. 4,34 In accordance with these studies, during laser irradiation, we used 2 cc/min of water coolant to prevent thermal damage to the dentinal structure. As a final rinse, 3 mL distilled water was used immediately after the surface treatments. As reported in previous studies, we aimed to prevent the formation of settled crystalline structures and to terminate the solvent effects of solutions. 35,36 During laser irradiation, another important concern is to use the appropiate laser tip to deliver energy through the root canal effectively. Previous studies found that conical fiber tips can be used safely and more effectively to remove smear layer than plain tips. 37,38 In the current study, we used a plain sapphire tip according to the laser device requirements; however, this can be considered a limitation of this study.
In this present study, the root canals were obturated with conventional gutta-percha and AH Plus and EndoREZ resin-based root canal sealers. Previous studies used only root canal sealer for obturation; however, this is not suggested clinically, because the sealer may dissolve over time, and this will produce leakage; therefore, thin layers of sealer are preferred. 39,40 For root canal filling, we used ∼1 mm thick dentin slices from each third to obtain reliable regional bond strength evaluation of the filling material to the dentinal wall. 41 To evaluate bond strength, the pushout test is an important tool. It is easy to align specimens for testing and it is less sensitive to small variations between the specimens than the tensile and shear strength tests. 42 Saleh et al. 23 evaluated the effect of dentin surface treatment on the adhesion of root canal sealer with tensile load application in the same direction as that of the dentinal tubules. Sousa-Neto et al. stated that with the pushout test, load application was perpendicular to the dentinal tubules that act as the actual forces that formed inside the root canal. 17 In this aspect, we preferred to use the pushout test to obtain more accurate results. Another advantage of the pushout test is that it allows the evaluation of the root canal sealers even though the bond strength is low. 42
AH Plus containing epoxy resin presented better penetration into the micro-irregularities, because of its long curing time, which increases of the mechanical locking between the resin and dentin, as well as its fluidity. This situation increases resistance against displacement, thereby possibly supporting higher bond strength. 27 The coronal photoactivation of the EndoREZ root canal sealer causes high polymerization stress that may induce the early displacement of the sealer. 43 In this study, AH Plus root canal sealer exhibited higher adhesion values than EndoREZ root canal sealer.
Babb et al. 44 showed that the variations in tubular density along the root canal are not an important factor altering the adhesion values of an endodontic sealer. In the present study, the specimens obturated with AH Plus root canal sealer did not show significant differences among the root canal thirds when subjected to different dentin surface treatments. Sly et al. 45 evaluated the adhesion of root canal obturation materials according to the root canal thirds. They reported that bond strength values did not differ among root canal thirds. However, because of the presence of greater collagen density in the apical region, higher adhesion values were expected there. 46 In the current study, a significant difference was detected in the apical region of the EndoREZ group when treated with the Nd:YAG laser. The apical region exhibited higher pushout strength values. Regardless of dentin pretreatments, AH Plus root canal sealer has shown higher adhesion values in the apical and middle thirds than in the coronal thirds; this may depend upon the higher ratio of collagen in the apical third. Epoxy resin-based root canal sealers react with amino groups that are exposed in collagen structure. As a result, the opened epoxide rings induce the formation of covalent bonds between the resin and dentine collagen. 31
Saleh et al. 23 concluded that removal of the smear layer may adversely affect the adhesion of the root canal sealer, and that root canal sealers require different dentin surface treatments for optimal adhesion. Furthermore, the researchers reported that the root canal sealers could not penetrate all of the exposed dentinal tubules after the removal of the smear layer, and that not all penetrating sealers showed high bond strength.
Bond strengths of different root canal filling materials were affected differently according to the irrigation solutions and laser systems. Based on this result, root canal obturation must be performed according to the interactions between the filling materials and dentin surface treatments.
Conclusions
Within the limitations of this in vitro study, Er:YAG laser irradiation can enhance the bond strength of AH Plus root canal sealer, whereas Nd:YAG laser irradiation can enhance the bond strength of EndoREZ root canal sealer. It can be concluded that AH Plus presented higher adhesion values than those reported for EndoREZ root canal sealer.
Footnotes
Author Disclosure Statement
No competing financial interests exist.