
Abstract
Introduction
S
Fractional lasers, which induce small, focal zones of tissue injury, are effective for treating various cutaneous diseases that require a large treatment area and high pulse energy; these lasers are well tolerated by patients, with fewer side effects than conventional laser therapies. In contrast to conventional ablative laser modalities that create a confluent, uniform patch of epidermal or dermal injury, fractional lasers induce a microscopic zone of tissue injury, stimulating collagen remodeling and deposition. 6 Currently, the non-ablative 1,550-nm erbium-glass fractional photothermolysis system (FPS) is one of the most popular fractional lasers in use clinically, and because the stratum corneum remains intact after FPS treatment and the epidermal barrier function is preserved, the severity and duration of side effects as well as the down time are significantly reduced. 6 –9 The ablative 10,600-nm carbon dioxide fractional laser system (CO2 FS) is also a frequently used device that is coming to the forefront. The action mechanism of the CO2 FS laser includes tissue ablation, immediate collagen shrinkage, and dermal collagen remodeling, which causes matrix metalloproteinases to eliminate the fragmented collagenous matrix and promote new collagen synthesis. 6,10 CO2 FS is gaining popularity because of its higher energy delivery and better outcomes with fewer treatment sessions.
To the best of our knowledge, comparative studies evaluating clinical outcomes and adverse events of FPS and CO2 FS therapy for various types of scars in a large group of Asian patients are rare, and our purpose was to compare the clinical outcome of each laser device for scars in Asian skin. Therefore, we evaluated the efficacy and safety of treatments using FPS and CO2 FS to improve the cosmetic outcomes of scars.
Materials and Methods
Patients
We conducted a retrospective study to compare the efficacy and safety of treatments with FPS and CO2 FS for various types of scars in East Asian people. One hundred patients with various types of scars who visited the Department of Dermatology at Yonsei University Health System from March 2010 to February 2011 were enrolled in the present study (29 males, 71 females, mean age 27.4 years, range 3–63 years, Fitzpatrick skin type III-IV). An informed consent was obtained from every individual prior to initiation, and the study was performed according to the ethical guidelines of the 1975 Declaration of Helsinki. The duration of scars varied widely among patients, from 3 weeks to 55 years (mean 73.7 months), and the number of treatments performed ranged from 1 to 12 sessions (Table 1). The types of scars included surgical scars, post-traumatic scars, burn scars, acne scars, and scars after cutaneous diseases. Scars were additionally classified as depressed or atrophic scars, hypertrophic scars, combined scars, and acne scars. Exclusion criteria were: history of keloid scarring, isotretinoin use, pregnancy, use of immunosuppressants, and previous concomitant treatments, including skin resurfacing procedures and chemical reconstruction of skin scars (CROSS) using trichloroacetic acid. Patients who had FPS or CO2 FS treatments within the previous 6 months were also excluded.
Laser treatment
The proper laser device and treatment parameters were chosen individually, based on the characteristics of patient scars. Patients were treated with either the non-ablative 1550 nm erbium-glass FPS using a Mosaic™ laser (Lutronic Corporation, Goyang, Korea), or the ablative 10,600-nm CO2 FS using a Mosaic eCO2 ™ laser (Lutronic Corporation, Goyang, Korea). If necessary, a combination therapy of FPS and CO2 FS was also conducted. The treatment intervals were 1.5–2 months, based on the scar characteristics, and the end-point of treatment was decided individually, considering the clinical outcomes and degree of patient satisfaction. For local anesthesia, the lesion was cleansed with a mild cleanser and 70% alcohol, and topical EMLA cream (eutectic mixture of 2.5% lidocaine HCl and 2.5% prilocaine; AstraZeneca AB, Södertälje, Sweden) was applied under occlusion 1 h prior to laser therapy.
For FPS, the laser was applied at a pulse energy setting of 25–32 mJ fluence, 200 spots/cm2 density, and static and/or dynamic operating modes; for CO2 FS, the laser was applied at 100–150 mJ fluence, 100–120 spots/cm2 density, and static and/or dynamic operating modes. After treatment, the treated areas were cooled with ice packs for 5–10 min for protection. To promote post-laser therapy wound healing, the patients were instructed to use a moisturizer several times a day for 1 week after treatment.
Objective and subjective evaluations
Objective evaluation
Photographs were taken using identical camera settings, lighting conditions, and patient positioning at baseline, before every treatment, and 3 months after the last treatment. Two blinded physicians evaluated the scars by comparing the clinical photography in a nonchronological order, taken before and after the treatment. We used a quintile grading scale for evaluations: grade 0, no improvement; grade 1, <25%=minimal improvement; grade 2, 26–50%=moderate improvement; grade 3, 51–75%=marked improvement; and grade 4, >75%=near-total improvement.
Subjective evaluation
Patients were surveyed 3 months after the last treatment to determine their overall levels of satisfaction with the treatment results using the following response choices: very satisfied, satisfied, moderately satisfied, slightly satisfied, and dissatisfied. The patients also reported any side effects of treatments including erythema, bleeding, oozing, edema, post-therapy dyschromias, scaling, crusting, and scarring.
Statistical analysis
We compared and analyzed the clinical assessment scores by dermatologists and the overall patient satisfaction levels associated with FPS and CO2 FS treatment using one way ANOVA, two sample t test, and correlations with Statistical Package for the Social Sciences version 18.0 (SPSS Inc., Chicago, IL). Differences were considered statistically significant when the p value was <0.05.
Results
Among the 100 patients, 42 patients had scars caused by trauma, 36 had postoperative scars, 10 had burn scars, 5 had acne scars, and 7 had scars induced by other cutaneous diseases such as herpes zoster, chicken pox, or Stevens–Johnson syndrome. Some patients had multiple scar lesions, and, therefore, the total number of scars was 106. Classification of the scars according to their characteristics was performed, and the 106 scars were classified into depressed or atrophic scars, hypertrophic scars, combined scars, and acne scars. Fifty-one patients (48%) had combined scars, and 34 patients (32%) had depressed or atrophic scars (Fig. 1). For improvement of scar lesions, 36 patients with 36 (34%) scars were treated with FPS, 18 patients with 20 scars (18.8%) were treated with CO2 FS, and 46 patients with 50 (47.2%) scars were treated with a combination treatment of FPS plus CO2 FS. The proper laser device and treatment parameters were chosen individually, based on the characteristics of the scars of each patient (Table 2). The end-point of treatment was also decided individually, according to the clinical outcomes and degree of patient satisfaction.
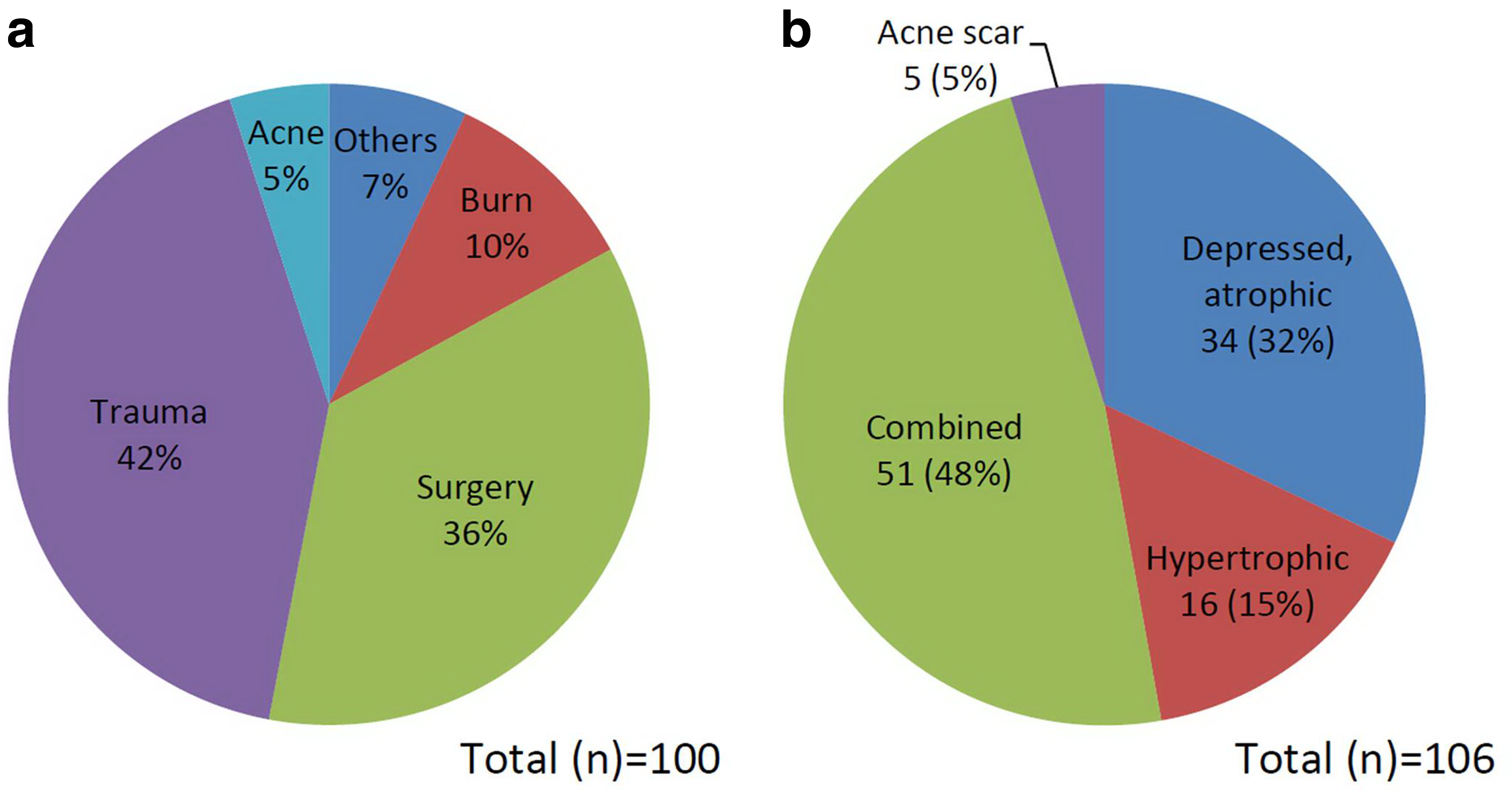
Scar classifications.
FPS, photothermolysis systems; CO2 FS, carbon dioxide fractional laser system.
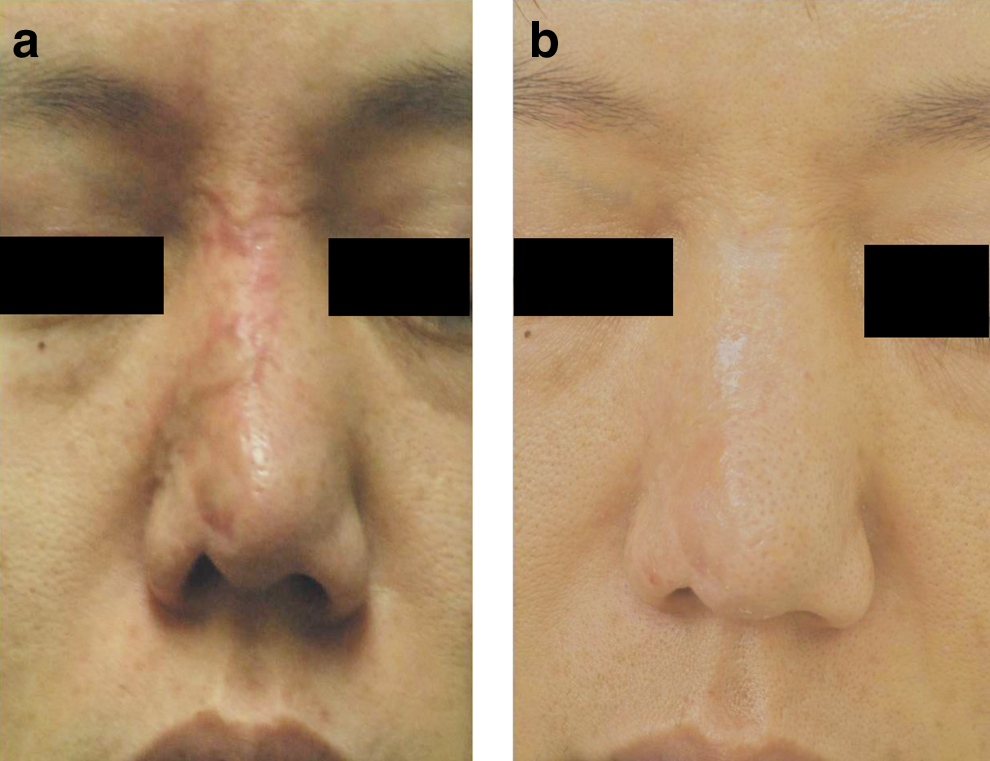
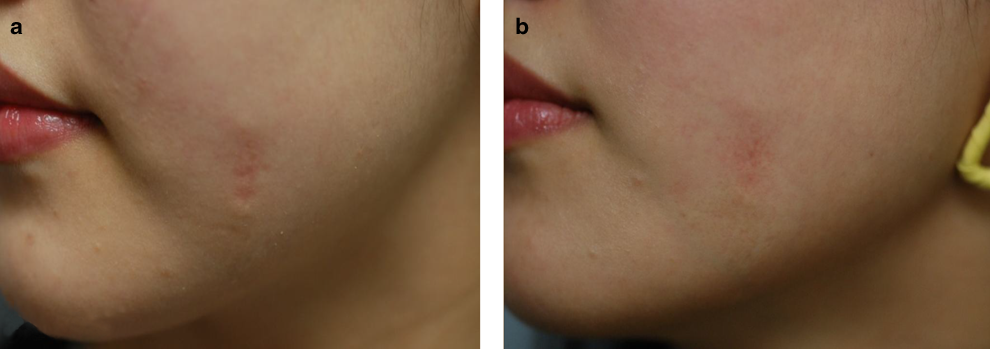
Follow-up 3 months after the last laser treatment resulted in 27 (25.5%) of the 100 patients showing moderate improvement, 61 (57.5%) patients showing marked improvement, and 12 (11.3%) patients showing near-total improvement (Figs. 2 and 3). The mean grades of clinical improvement based on assessment of the clinical photography were 2.64±0.76 for FPS, 2.60±0.68 for CO2 FS, and 2.94±0.83 for FPS+CO2 FS. The mean values did not show significant differences among laser devices (p=0.249). The mean grades of clinical improvement according to scar type were 2.72±1.02 for depressed or atrophic scars, 2.25±0.91 for hypertrophic scars, 2.27±0.98 for combined scars, and 2.31±0.95 for acne scars. The results did not differ significantly among scar types (p=0.344). The mean grade of improvement also did not differ between males and females (p=0.919) and did not show any correlations with patient age (p=0.857). When patients were divided into two groups based on time since scar development—patients who received treatment within 3 years of scar development (n=73) and patients who received treatment after 3 years of scar development (n=27)—the mean grade of improvement differed significantly between these two groups, 2.84±0.69 for the former group and 2.51±0.82 for the latter (p=0.042). The number of treatments did not significantly influence the grade of clinical improvement (p=0.251) (Table 3).
FPS, photothermolysis systems; CO2 FS, carbon dioxide fractional laser system.
Surveys evaluating the degree of patient satisfaction revealed that 37 (34.9%) patients were moderately satisfied 3 months after the last treatment, 37 (34.9%) were satisfied, and 10 (9.5%) were very satisfied. Only one (0.9%) patient was dissatisfied with the outcome, among the 100 patients. Degree of patient satisfaction did not differ between males and females (p=0.793), and also did not show any correlation with age (p=0.874). Most participants reported that post-treatment erythema, edema, crusting, and scaling resolved within 1 week. Eleven patients experienced post-treatment hyperpigmentation, and six patients reported post-treatment erythema that lasted for >1 week, but spontaneous resolution occurred within 3 weeks in all cases. Other possible adverse events, including post-therapy blister formation, scarring, and secondary bacterial or viral infection, were not observed.
Discussion
The concept of FP was introduced in 2004 by Manstein and colleagues. 6 FP produces arrays of microscopic thermal wounds called microscopic treatment zones (MTZs) in the skin at a depth of 300–400 μm into the dermis without giving injury to the surrounding tissue. Therefore, in spite of the depth of injury in the mid-dermis, the intact dermal tissue next to the MTZ rapidly heals around the columns of thermal damage, and stimulates progressive collagen remodeling. 6 The original concept of FP was non-ablative, using near-infrared energy, sparing the epidermis, and, therefore, ideally provided rapid healing time and fewer side effects such as erythema or edema. However, despite the advances of reduced down time of nonablative FP, the requirement of multiple treatment sessions to receive an acceptable outcome resulted in the development of the more aggressive ablative FP, in which the MTZs included the epidermis. The greater degree of cutaneous injury induced by ablative FP was shown to provide a greater and prolonged effect on inducing new collagen generation and remodeling of dermal collagen. 11 –13 Currently, nonablative and ablative FP devices have been validated to be used in various cutaneous conditions, including wrinkles, photoaging, pigment abnormalities, scars, and others. 14 –17
In this study, we reviewed 100 patients with various types of scars who received FP laser treatments for the purpose of clinically improving scars. Laser devices and number of treatment sessions differed among individuals according to their scar characteristics. Although the combination therapy of FPS+CO2 FS resulted in highest improvements, the mean grade of improvement did not show statistically significant differences among FPS, CO2 FS, and FPS+CO2 FS. This reflects the fact that not only the laser device, but also the duration of the scar or scar characteristics and number of treatment sessions are also important factors that can affect the clinical outcome of scar treatment. Furthermore, although depressed or atrophic scars showed the greatest improvements, the mean grade of improvement did not differ significantly among scar characteristics. Therefore, it can be suggested that various factors such as scar characteristics, scar duration, number of treatment sessions, laser modalities, and technique complexly contribute to the improvement of scars. Nevertheless, treating the scar with repetitive sessions did not correlate with better treatment outcomes, suggesting that scar characteristics, treatment response, and patient satisfaction should be considered together to decide the end-point of treatment. These results show that it is difficult to simply predict the outcome of scar treatment, because the process is very complex with various contributable factors.
Our results suggest that early treatment after scar formation may lead to better improvement after laser therapy, as patients who received treatment within 3 years of scar development showed significantly greater improvements than did patients who received treatment >3 years after scar formation. It is known that scar remodeling and clinical improvement continues to occur over 2–3 years after scar formation, and because of the ability of remodeling and regeneration of the cutaneous tissue during this period, laser treatment can facilitate and help this process. Therefore, although the appropriate window for laser treatment after scar formation is yet unknown, early initiation of treatment is now preferred. 18,19
Scar treatment with FPS and CO2 FS was a safe and tolerable procedure with minimal side effects and acceptable clinical improvements. However, our results do not constitute a conclusive comparison of the two fractional laser systems, because of the limited sample size, variations in scar characteristics and scar durations, and the different number of treatment sessions among patients. As our study includes various different types of scars with different causes, it is difficult to objectively compare the treatment results, because every scar may show a different healing course after laser treatments due to the diverse nature of each scar. The different parameters used for each device are another limitation in this study, because to accurately compare treatment outcomes, the penetration depth and width of the laser column should be controlled. Selection bias is also a possibility, as the type of laser device was chosen upon the initial physician's assessment, and less severe types of scars might have received non-ablative procedures. However, we made efforts to objectively select the laser device according to the characteristics of the scar, such as depression, atrophy, and hypertrophy, and not the severity of the scar. Additionally, we could not completely eliminate the possibility of subject bias, as the participants experienced different post-treatment responses with FPS and CO2 FS. A prospective, randomized study with unified conditions of scars and treatment sessions with controlled parameters would be required to compare the efficacy and safety of the two laser systems more accurately and objectively.
Conclusions
In conclusion, the present study demonstrated the efficacy and safety of laser treatments on various types of scars using FPS and CO2 FS in East Asian patients. As a result, FPS and CO2 FS can both be safe and effective options to consider for scar treatment, and the two devices can also be used together safely. However, it can be suggested that the proper laser device and proper initiation time for scar treatment should be decided considering various factors such as type of scar, duration of scar, anatomical site, and patient demand. We also suggest that early treatment of scars is safe and effective, and although the proper time to initiate laser treatment after scar formation remains unknown, early treatment of scars may result in better improvements.
Footnotes
Author Disclosure Statement
No competing financial interests exist.