
Abstract
Introduction
I
It is generally accepted that the LTW is primarily a photothermal process: laser light absorbed by tissue chromophores (water, hemoglobin, and melanin) is converted to heat, which induces a local temperature increase. As the laser energy is converted into heat, it induces molecular thermal changes. When a sufficient number of tissue molecules are altered, enough bonds are formed between the edges, conferring satisfactory tensile strength to the tissue fusion. The molecules and the types of molecular bonds involved in this process are still not well known. 4 In ideal conditions, the thermal damage should be limited to the immediate area of the weld site. Therefore, LTW critical parameters are the temperature rise and its tissue distribution; an uneven and/or an insufficient heating of the incision edges will not alter enough molecules, resulting in weak welds, whereas a too-high temperature will induce collateral thermal damage, impairing the wound healing. Consequently, the major limitations of the clinical application of LTW are poor tensile strength and collateral tissue heat damage. In addressing these issues, two main strategies have been developed. The first approach 5,6 consists of matching the optical penetration depth to the thickness of the tissue to be welded. As water is the most abundant constituent of almost all tissues and the principal natural chromophore, Beer's law and the water absorption coefficient allow for the calculation of the optical penetration depth for a given laser wavelength; therefore, the laser welding of a given tissue thickness necessitates the choice of a suitable wavelength. The advantage is the use of natural chromophores, without adding foreign substances. The second approach 7 –9 consists of enhancing the optical absorption of the target tissue by adding exogenous chromophores associated or not associated with exogenous proteins as a solder. The use of a wavelength-specific chromophore enables differential absorption between the stained and unstained tissue. The advantage is a selective absorption of laser radiation by the target, inducing a higher temperature at the welding site and less heat damage around it; meanwhile, lower laser irradiances may be used to achieve the required effect.
Extensive efforts have been expended over the past 50 years to bring LTW from the laboratory into clinical practice. By using many experimental models, different wavelengths, and various irradiation conditions, laser welding has been explored in many different tissue types: blood vessels, gastrointestinal tract, genitourinary organs, peripheral nerves, skin, and cornea. 3,10,11 To the best of our knowledge, there has not yet been any experimentation exploring the laser welding of the oral mucosa. The objectives of this preliminary study were: to assess the feasibility of the laser gingiva welding in an ex vivo animal model, to find the irradiation conditions yielding the best tensile strength, to compare the tensile strength between the laser welded and the sutured gingiva, and to evaluate the temperature rise and the extent of the thermal tissue damage.
Materials and Methods
Animal model and study design
According to previous studies, 12 the validated animal model of the human gingiva is the porcine gingiva. Lower jaws of 6-month-old pigs slaughtered 14 h prior to the experiments were obtained from a slaughter house. Taking into account previous studies, 13 the jaws were transported and stored at 4°C, and particular attention was given to their state of hydration throughout the experimental period, by spraying them with 0.9% saline solution.
From each jaw, we excised bilaterally a large full-thickness flap composed of the buccal gingiva and the corresponding oral mucosa between the canine and the retromolar region. This large flap was then divided in two samples, trimmed to conform to a 2 cm wide×3 cm long template. Therefore, four samples were harvested from each jaw on a total of 166 pieces. Excess tissue thickness was removed, leaving only the mucosa. The average thickness of the resulting samples was 1 mm; however, the thickness of each specimen varied between 0.5 and 2.5 mm. In the middle of each sample an incision of 2 cm length was performed.
The first group of 147 jaws provided 588 samples, which served to assess the irradiation conditions (468 samples) and the chromophore concentration (120 samples) yielding the best tensile strength of the welds. These experimental conditions were then used to study the tensile strength and the extent of the thermal injury in the laser welded gingiva. A second group of 16 jaws (64 samples) were used as follows: two symmetrically harvested samples served to compare the laser welded and the sutured gingiva tensile strength, the third sample served to evaluate histologically the thermal damage extent, and the fourth sample was kept intact, as a negative control (it was histologically prepared but has not been further used in this study). The third group of three jaws (12 samples) served to complete the temperature measurements by thermal camera; these samples were completely incised, so as to see the total incision depth by looking at the shorter side of the specimen.
LTW irradiation conditions and conventional suture
The laser gingiva welding was performed with a diode laser of 808±0.5 nm (Sapphire Portable Diode Laser®, Den-Mat Holdings, Santa Maria, USA). The laser beam was delivered by a 400 μm optic fiber in a quasicontact mode; the spot diameter was 406 μm. The emitted power measured by a power meter (UP19K-15S, Gentec-EO, Québec, Canada) represented 40% of the displayed power. Depending upon the operator, the exposure time needed to obtain an effective LTW was 60–130 sec for the whole incision length, corresponding to a laser scanning rate of 1 mm for 3–7 sec.
The chromophore used was indocyanine green (ICG) (TCI, Tokyo, Japan), of which peak absorption in aqueous solution matched that of the diode laser wavelength. Because the ICG absorption curve depends upon concentration and upon solvent, 14 and because effective welds were achieved with 808 nm diode laser and high-concentration ICG solution, 15,16 six ICG solutions in the same range of concentration, that is, 8% (106 mM), 9% (117 mM), 10% (130 mM), 11% (142 mM), 12% (157 mM), and 13% (168 mM), were used to assess the concentration yielding the best tensile strength of the gingiva welds. Before laser welding, a drop of ICG solution was applied over the incision by using a 28 gauge needle; then the excess was carefully wiped off. During the procedure, the tissue edges were firmly clamped together by forceps. In order to select the irradiation conditions yielding the best tensile strength, 13 irradiation conditions were tested for each chromophore concentration (Table 1). According to these results, we chose the irradiation conditions in which to perform the LTW, allowing an assessment of the tensile strength, the temperature rise, and the extent of the thermal tissue damage.
ICG, indocyanine green; CW, continuous wave.
The conventional sutures were achieved by a 5-0 silk surgical thread (Angiotech, Surgical Specialties Corp., PA) knotted three times. The incisions were closed by five interrupted full-thickness suture points made every 2 mm at a 2 mm distance from the edges.
Temperature measurements
The LTW performed on the 32 samples of the second group induced a temperature rise that was measured by two K-type thermocouples (HH806AWE, Omega, Manchester, UK), placed beneath the welding site and on the upper surface of the tissue flap, 1 cm distant from the welding site.
On the third group of 12 samples, the temperature evolution during LTW was followed up by a thermal camera (Thermovision 900, Agema, Infrared System AB, Danderyd, Sweden) detecting infrared signals in the 2–5.4 μm spectral band, and generating images by the version Erika 3.1 software. Each sample was placed at the focus distance, and was “viewed” by the camera all along its incision depth during the laser welding.
Tensile strength measurements
The mechanical force required to break off the tissue repairs performed either by laser welding or by suture was measured by using a digital force gauge (Sauter FH 10, Sauter GmbH, Balingen, Germany) mounted on a test stand (SLK Wheel Manual Test Stand, SunDoo Instruments Co., WenZhou, China). Normal tension was applied at the incision axis to all samples. The maximum tension needed to create a visible hole in a properly closed incision was recorded. This value was divided by the grip length (8 mm) multiplied by the thickness of the incised tissue, to arrive at a tensile strength in N/cm2. To avoid an increasing tensile strength caused by drying, the tissue samples were kept moist throughout the procedure, by spraying them with a 0.9% saline solution.
Histological study
Immediately after laser welding, the samples were placed in a 10% buffered formaldehyde solution for 2 weeks. Then, they were histologically processed according to the standard procedures for optical microscopy study. Finally, the 6 μm thick sections were stained with picrosirius red solution (Direct Red 80, Sigma-Aldrich, St. Louis, MO) as previously described. 17 This staining enhances the natural birefringence of the collagen fibres when placed in polarized light. The heat induces a loss of the collagen birefringence. The sharp demarcation separating birefringent and nonbirefringent zones examined under polarized light allows an accurate micrometric measurement of the altered tissue. Thus, the thermal damage extent was assessed by measuring the maximum distance (in μm) of the altered tissue at its upper surface, and then all along the repair at 77×magnification.
Statistics
Statistical analyses were performed with Prism 5® software (GraphPad Software, Inc., San Diego, CA). Paired t test was used to eliminate any interindividual bias (e.g., age, sex, postmortem interval). It compared the tensile strength between the laser welded and the sutured samples collected symmetrically in the same animal. One way analysis of variance (ANOVA) with Tukey's multiple comparison test were used to assess statistical significance, defined as p<0.05, of tensile strength and temperature differences among sample groups.
Results
LTW irradiation conditions
Among the 78 combinations of 13 irradiation conditions and six ICG concentrations, the strongest gingiva welds (25.09±4.89 N/cm2) were achieved with an output power of 4.5 W at 10 Hz, corresponding to a measured power density of 1391 W/cm2 and a fluence of 31.3 kJ/cm2 (Fig. 1). These irradiation conditions tested on six sample groups, one for each ICG concentration, indicated that the best tensile strength (p<0.05) was yielded by the 9% saline solution (117 mM) of ICG (Fig. 2). Consequently, all the following measurements were performed on laser welds obtained by using these parameters.
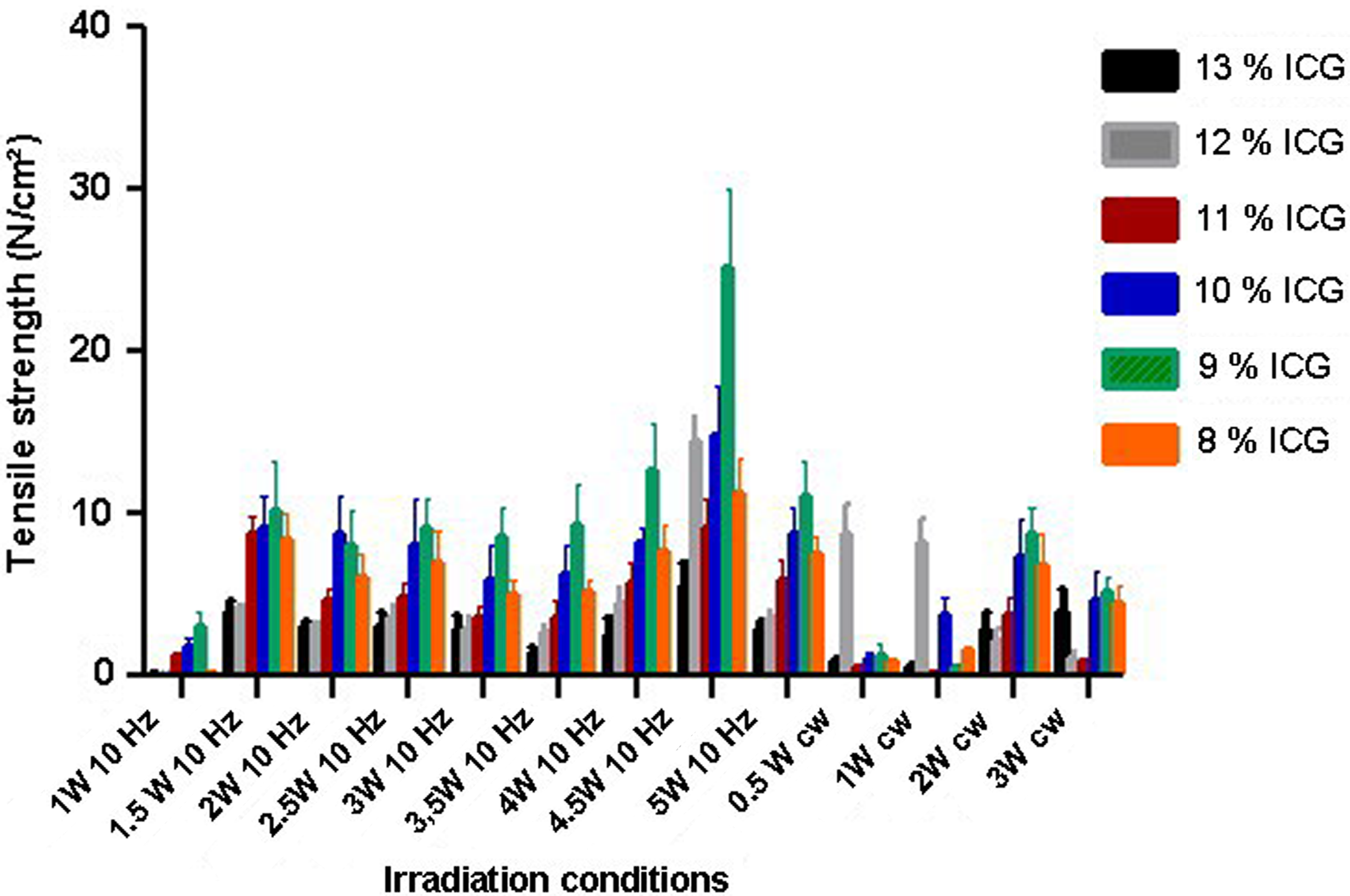
Means and SD of tensile strength values in function of irradiation conditions. The strongest gingiva welds (25.09±4.89 N/cm2) were achieved with an output power of 4.5 W at 10 Hz, corresponding to a measured power density of 1391 W/cm2 and a fluence of 31.30 kJ/cm2 ; The number of samples in each group is six.
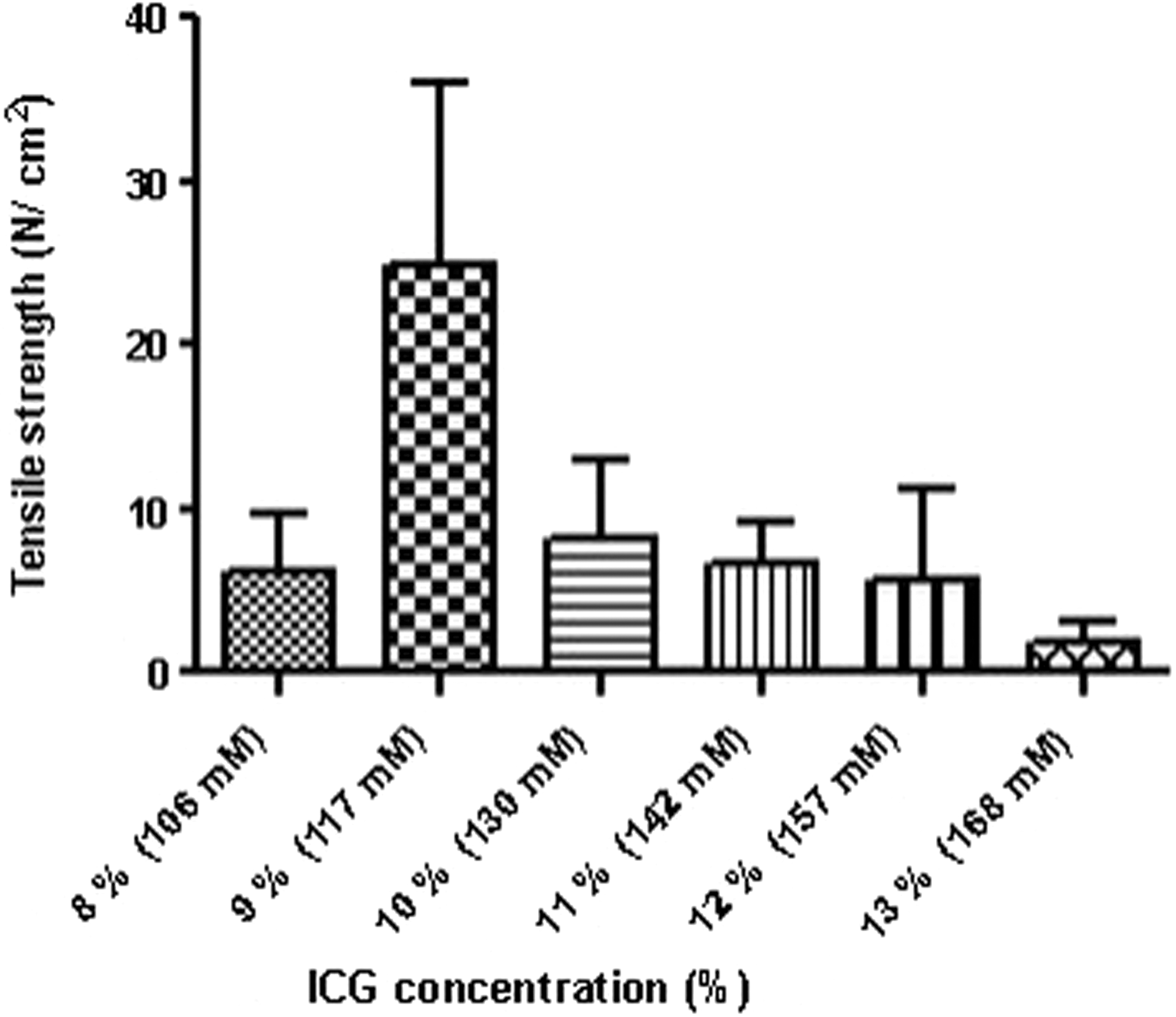
The influence of the indocyanine green (ICG) concentration on the tensile strength tested by one way analysis of variance (ANOVA). The 9% ICG solution yielded a significantly (p<0.05) higher laser tissue welding (LTW) tensile strength as compared with all the other assessed ICG concentrations used for the same irradiation conditions (4.5 W, 10 Hz, 1391 W/cm2, 31.3 kJ/cm2).
Tensile strength measurements
Considering the suture apposition strength, the paired t test indicated no statistically significant difference between the sutured and the laser welded gingiva (Fig. 3), even though the mean value was higher for the conventionally repaired incisions, that is, 32.95±12.59 N/cm2 compared with 25.36±12.36 N/cm2.

Means and SD of tensile strengths of the laser tissue welding (LTW) and the conventionally sutured oral mucosa (paired t test).
Temperature measurements
The temperature was initially measured by thermocouples. Beneath the welding site, the average temperature was 48°C±16.8°C, whereas at 1 cm distance from the uppermost welding point, the temperature averaged 26°C±2.5°C. Then, the temperature measurements were repeated by thermal camera. For this second series of measurements, the average temperature at the lowest point of the welding site was 42°C±8.9°C. Meanwhile, at the uppermost layers of the welded tissue, the temperature rose to 74°C±5.4°C. In the surrounding tissue, the mean temperature rose to 50°C±4.7°C (Table 2).
At the upper surface of the samples, the temperature was recorded for the welding site, for the tissue surrounding the welding site, and for the 1 cm distant tissue. At the lower surface (intrados) of the welding site, the temperature was measured by thermal camera and by thermocouple.
Histological study
Micrometric measures revealed at the upper surface of the welding site that the damaged zone had an average width of 333±107 μm. The typical funnel-shaped damaged zone had a depth of 680±132 μm, tapering to a thin band of altered tissue with an average width of 123±21 μm (Table 3). We did not use any correction factors to compensate for eventual linear tissue shrinkage following sample fixation. 18,19 Figure 4 shows the damaged zone.
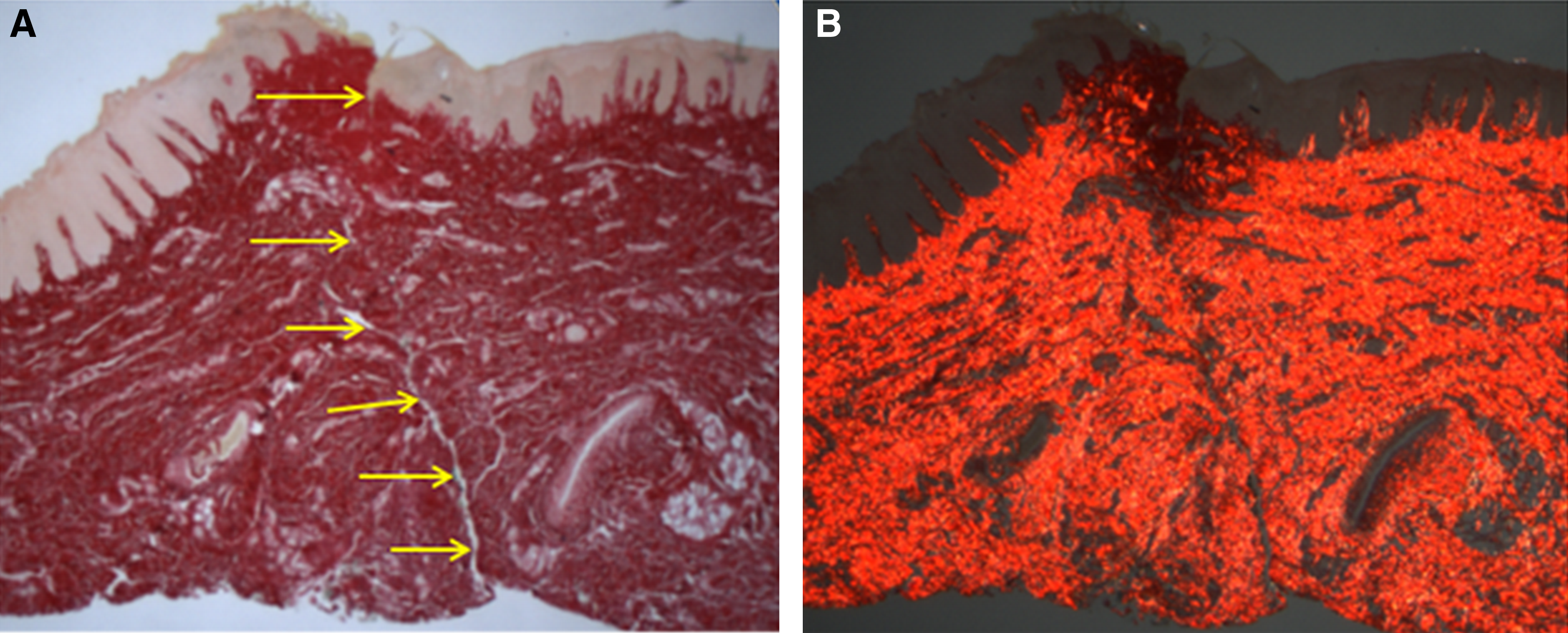
Laser welded porcine gingiva (arrows) stained by picrosirius red and examined by optical microscopy at×24 magnification, under normal light
The funnel-shaped damaged zone, having the largest width at the upper aspect of the flap, is tapering to a minimal width of damaged tissue, involving both edges beneath the funnel-shaped zone.
Discussion
Human masticatory mucosa thickness can vary between <0.7 mm, for the facial gingiva at canines in the maxilla, to >4 mm, for the gingiva in the tuberosity and retromolar regions. 20 Therefore, a suitable laser wavelength for LTW should vary between 1300 and 1800 nm. Taking into account the considerable intra- and interindividual variation in the thickness of oral mucosa, the use of a chromophore seems to be a more practical strategy. The drawback of this strategy is the use of a colored foreign substance in tissues of aesthetic importance.
ICG was tested in the late 1950s for use in human medicine. 21 Ever since, it has been widely used in various medical applications, 22 and few cases of side effects have been reported. Nevertheless, some concerns arose about toxic effects on retinal cells observed in studies conducted in vitro and in vivo, as well as following vitreoretinal surgery. 23 Studies into the possible toxic effects of ICG on oral mucosa cells in LTW conditions remain to be performed.
As a chromophore, ICG has been extensively used in LTW because of its absorption properties at the 808 nm diode laser wavelength. Because a higher chromophore concentration induces a lower tissue temperature rise, and, therefore, a poorer tensile strength, 24 ICG concentration is an important parameter in obtaining a satisfactory tensile strength. Oddly, ICG light absorption does not increase linearly with increasing concentration. 14 Also, the absorption spectrum changes when ICG is added to proteins. When bound with cell proteins, in tissues and cells the ICG absorption peak is shifted to 810 nm. 25 Further studies are needed to determine the absorption spectrum shifting of ICG-stained oral tissues in relation to the ICG concentration applied onto them.
Because the extent of the protein denaturation is linearly proportional to time and is an exponential function of temperature, 26 the temperature is the dominant parameter governing the LTW process. Thermocouples are the most common devices used for temperature measurements. Because their position relative to the laser spot is variable during the laser welding procedure, they may give falsely low or high readings depending upon their location. 27 Thermal cameras circumvent this problem. However, they have their own shortcomings, as a result of which the real temperature can be underestimated. 28
Experiments using a controlled-temperature system to achieve LTW have shown that the surface temperature necessary to ensure a convenient tensile strength varied from one tissue to another. In vivo LTW experiments on urinary bladder in rats using CO2 laser associated with an albumin solder have shown that the strongest tissue bond was formed at 55±2.5°C. 27 Ex vivo LTW experiments on porcine cornea using an 808 nm diode laser associated with ICG have shown the efficiency of a maximum temperature peak in the 59–66°C range, as calculated inside the stained wound. 16 An ex vivo study on porcine dura repair using a temperature-controlled CO2 laser reported a needed surface temperature of 70°C. 29 Aorta welds in rats performed in vivo by a 1.95 μm diode laser demonstrated that even though tissue fusion was achievable over a surface temperature range of 70–90°C, 100% success rates only occurred within the middle of this range, at 80°C. These results suggest that the temperature range yielding strong enough welds is relatively narrow compared with the broad range of temperatures for which apparent tissue fusion may occur. 30 Furthermore, the temperature at which denaturation occurs is not a constant, but increases approximately linearly with the logarithm of the heating rate. 31
When the temperature was simultaneously measured at the adventitial surface by thermal camera, and at the intimal surface by thermocouple during LTW performed ex vivo on human veins, a quasiconstant difference of 25–30°C was observed. 26 The thermal conductivity of the vein wall, decreasing with the tissue dehydration, was assumed to be responsible for the temperature differential. The temperature distribution in the welded tissue depends upon its optical properties (absorption, scattering and transmission of the light) and thermal conductivity. These characteristics are changing during welding, because of protein denaturation and tissue dehydration. Furthermore, the protein denaturation is related to dehydration: the denaturation temperature increases exponentially with the water loss, whereas the denaturation rate increases linearly with the protein dehydration. 32 Additionally, the state of tissue hydration plays a crucial role in tissue bonding. 33
Proper incision closure avoids gaps between tissue edges, representing potential sites of fluid leakage and/or infection. Therefore, the sutured incision strength was defined as the “suture apposition strength” rather than the much higher tensile strength needed to break the surgical thread. 34
In our experiments, the tensile strength values were scattered over a wide range, for both the laser welded and the sutured samples. Previous studies attributed the poor reproducibility of the repair strength to (1) the air gaps trapped between the bonding faces, 33 depending upon the dimensions and the shape of the contact area between edges, as well as the accurate apposition and the pressure applied on the edges; and (2) the tissue buckling caused by the dehydration during the laser welding. 35 Furthermore, the hydrated state of the tissue influences the strength of its repair, because at any temperature dehydration is responsible for an increased tensile strength of the tissue bonds. 33
Collagen birefringence changes are induced by temperature increase at which other morphologic changes are hard to detect. 36 A considerable reduction in birefringence is induced by heating the collagen above a threshold temperature of ∼70°C. 36,37
Previous studies reported a total destruction of the epithelium across a width of ∼1.5 mm when an 808 nm diode laser was used at 1.8 kW/cm2 power density for ex vivo biopsies in pig oral mucosa. 38 On the other side, in vivo studies have shown that the healing of the incisions performed in the palatal mucosa of rats either by scalpel or by an 808 nm diode laser (at a 4 W output power delivered in a continuous mode by a 400 μm fiber, for ∼6 sec) was complete at 14 days, with no difference between the two techniques. 39 In clinical conditions, an 808 nm diode laser has being used 40 with an average output power of 2.5 W delivered in a continuous wave mode by a 320 μm fiber in order to measure the thermal damage in oral mucosa biopsies performed for histopathological diagnoses. The width of the thermally injured tissue ranged from 260.7 to 321.4 μm, with a mean value of 282.8 μm. By using a chromophore, our study suggests that a lower power density could be enough to obtain the laser welding of the gingiva and, meanwhile, to provide safer conditions for healing.
Conclusions
Our results demonstrated that the use of an 808 nm diode laser with an output power of 4.5 W at 10 Hz associated with a 9% ICG solution was able to perform welds of satisfactory tensile strength with limited thermal tissue damage. These findings lay the groundwork for future in vitro and in vivo studies, as well as for clinical trials using LTW as a promising procedure in oral surgery. However, further studies are required to improve the reproducibility of the experimental results and to support the safety of this closure technique, particularly to assess ICG toxicity for oral mucosa cells.
Footnotes
Acknowledgments
The authors thank the following persons for their contributions to this article: all the team of Alazard & Roux Slaughter House for their efforts in preparing with care the porcine jaws, Dr Stéphane Pichon for help in preparing the ICG solutions, and Vincent Delacour for preparation of histological slides.
Author Disclosure Statement
No competing financial interests exist.