
Abstract
Introduction
P
Resin-modified glass ionomer materials (RMGI) are modified by hydroxyethyl methacrylate incorporation into the glass ionomer to improve the mechanical properties and to make it activated by light. 5 –7 Vitremer (3M ESPE) requires setting reactions based on acid base neutralization and free radical methacrylate polymerization. A third setting reaction is necessary to ensure that the remaining monomer not affected by irradiation continues to polymerize. 6
Resin-based dental materials have camphorquinone as the photoinitiator with a maximum light absorption of 468 nm. 8 Quartz-tungsten halogen (QTH) lamps have been used to activate resin-based dental materials; however, the improvement of light-emitting diode (LED) technology has made LED activation more common. This light source presents a remarkable improvement, because it is an inexpensive and durable activation source and its advancement is comparable to the advancement of computer technology. 9 Nevertheless, there is limited information regarding LED activation for RMGI. 7,10
Argon-ion lasers (ALs) have been used as a light activation source of resin-based dental materials since the early 1980s. 12,13 Camphorquinone is activated by irradiation with an AL, which has an emission band at 488 nm. 14 The use of an AL for bonding orthodontic brackets, 12,13 composite resin (CR) activation, 11,14 –16 and sealant curing 17,18 has been demonstrated.
The AL irradiation itself provides a reduced depth of caries lesions in sound enamel. 19 When it is associated with topical fluoride, it increases the microhardness of enamel 20,21 and decreases the depth of caries in enamel. 4 In addition, Nammour et al. 22 have reported a higher fluoride retention (4×) for enamel irradiated with a low dose AL (10.7 J/cm2).
Research involving demineralization around restorative materials activated by an AL after bur-prepared cavities has not been described in the literature. AL activation of a fluoride-releasing material such as RMGI could decrease the enamel mineral loss around dental restorations. Moreover, pH cycle experiments simulate oral cariogenic conditions and are conducted to provide information regarding enamel demineralization of restorative materials and adhesives used in cavity preparation techniques. 4,23
The objective of this study was to evaluate the inhibition of enamel demineralization around restorative materials after QTH, LED, or AL activation according to the Knoop microhardness (KHN) profile of the enamel and the indirect degree of conversion in the superficial and deep areas of restorative materials.
The null hypotheses tested were as follows: (1) the superficial enamel KHN values around the two restorative materials cured by different light-curing devices are not different; (2) the cross-sectional enamel KHN values around the two restorative materials cured by different light-curing devices are not different; and (3) there is no difference between restorative materials in terms of the KHN values.
Materials and Methods
Ethics statement
This study protocol was approved by the Guarulhos University Research Ethics Committee (CEP-UnG, process No 104/2009).
Experimental design
The experimental units consisted of 36 dental blocks (n=6 per group). Eighteen unerupted human third molars were stored in 0.1% thymol solution at 4°C. Thirty-six dental blocks of 4×4×2 mm were sectioned with double-faced diamond disks (no. 7020; KG Sorensen, Barueri, SP, Brazil) used at low speed (Kavo, Joinville, SC, Brazil) and under water irrigation.
Cavity preparation and restoration
Cavity preparations of ∼1.6×1.6×1.6 mm were made with no 2292 diamond burs (KG Sorensen, Barueri, SP, Brazil) under a water spray. The teeth were distributed into two groups according to the restorative material used: RMGI (n=18) and CR (n=18). Each group was divided into three subgroups according to the activation source: QTH, AL, and LED (n=6 for each subgroup). The groups were as follows: G1, RMGI activated by QTH (24 J/cm2); G2, RMGI activated by AL (24.2 J/cm2); G3, RMGI activated by LED (24 J/cm2); G4, CR activated by QTH (24 J/cm2); G5, CR activated by AL (24.2 J/cm2); and G6, RMGI activated by LED (24 J/cm2).
All cavities were prepared and restored by the same trained operator. Table 1 lists the composition, lot number, and application instructions of the selected materials. A commercial RMGI (Vitremer, 3M ESPE, St. Paul, MN; A3) was tested in this study. RMGI was mixed according to manufacturer's instructions at a 1:1 ratio and inserted in a single increment with a Centrix Syringe (Centrix Inc., Shelton, CT) 30 sec after Vitremer Primer (3M ESPE) application, dried for 5 sec, and light activated for 20 sec. G1, G2, and G3 were activated according to each activation source. After RMGI insertion, Vitremer Finishing Gloss was applied and light activated for 20 sec with an LED (RadiiCal Plus, SDI Limited, Bayswater, Victoria, Australia).
bis-GMA, bisphenol glycidyl methacrylate; Bis-EMA, bisphenol A polyethylene glycol diether dimethacrylate; UDMA, urethane dimethacrylate; DMA, dimethacrylates; HEMA, 2-hydroxyethyl methacrylate; TEGMA, triethylene glycol dimethacrylate; QTH, quartz-tungsten-halogen.
A two step etch-and-rinse adhesive system (Adper Single Bond 2, 3M ESPE) was used according to the manufacturer's instructions (G1, G2, and G3). Enamel surfaces were etched with 37% phosphoric acid for 15 sec, rinsed with water, and dried with a stream of air. After application of the adhesive system with disposable microbrush tips, excess solvent was evaporated with a gentle stream of air for 5 sec and the adhesive was light-cured for 10 sec. Light activation of adhesive was performed with an LED (1,200 mW/cm2; RadiiCal Plus, SDI Limited, Bayswater, Victoria, Australia) for all groups. The intensity was monitored with a radiometer (Cure Rite, Dentsply Caulk, Milford, DE). After the bonding procedure, a nano-filled CR (Filtek Z350, OA3, 3M ESPE) was selected. The CR was inserted in a single increment and activated by each respective light source. Restored enamel blocks were placed in 100% relative humidity at 37°C for 24 h and then polished using the Sof-lex (3M ESPE) disk system for 15 sec with each disk.
An 11 mm diameter light tip was placed in an Optilux 501 halogen curing unit (Demetron/Kerr, Danbury, CT), and its power density was measured by a radiometer, which confirmed 600 mW/cm2 (±58 mW/cm2) of irradiance. An LED source with a power density of 1200 mW/cm2 (RadiiCal Plus, SDI Limited, Bayswater, Victoria, Australia) and an 8 mm diameter light tip were used. The AL (Accucure 3000, LaserMed, Salt Lake City, UT) used could have a power output of 100, 150, 200, or 250 mW; the power selected was 200 mW for a 39 sec contact. The energy (J) was calculated by multiplying the intensity (mW) by the exposure time (sec). The AL used in this study emitted light at 488 nm and produced a spot of 6.3 mm in diameter, which was measured according to the knife-edge method to produce a power density of 620 mW/cm2.
All groups received the same energy density to a fixed area (fluence, J/cm2), which was calculated by multiplying the power density by the exposure time.
Quantitative evaluation of the restorative material at the surface (0 mm) was performed by five central indentations of 100 μm at the restorative material surface. By means of a microhardness tester (PanTec, Panambra, São Paulo, Brazil) a 25 g load was applied for 20 sec. The restorative material evaluation was performed 24 h after photoactivation. The response variable was microhardness in KHN units.
The specimens were thermocycled 1000 times in between distilled water baths held at 5°C and 55°C for 24 h. The dwell time was 60 sec, and the transfer time was 5 sec (MSCT-3e, Elquip, São Carlos, Brazil).
The restored enamel blocks were covered by wax, with the exception of the restoration area and 1 mm around it. The restored enamel blocks were submitted to pH challenge to induce caries-like lesions. To produce caries-like enamel lesions, a demineralization/remineralization model, developed by Featherstone, was modified to simulate high caries risk.
Each restored block was placed in 15 mL of demineralization solution at 37°C (2.0 mM calcium, 2.0 mM phosphate-buffered solution, and 74 mM acetate, pH 4.3). The pH cycling regimen was performed for 7 days with five daily cycles for 6 h in demineralizing solution at 37°C. The remineralization solution contained calcium and phosphate at a known degree of saturation (50 mM KCl, 1.5 mM Ca, 0.9 mM PO4, and 20 mM Tris, pH 7.0), which was changed daily. The enamel blocks were washed with distilled water before immersion in the remineralization solution for 18 h. During the 6th and 7th days of the cycle, the restored enamel blocks were kept only in the remineralization solution according to the protocol described by Rodrigues et al. 4 .
Quantitative evaluation according to the KHN profile of the caries-like enamel lesions was performed by four indentations located 100 μm from the restored cavity in each enamel block around the restoration margins in the upper, bottom, left, and right sides (Fig. 1). By means of a microhardness tester, a 25 g load was applied for 5 sec. The mean of four KHN values obtained from each specimen was used for evaluation.
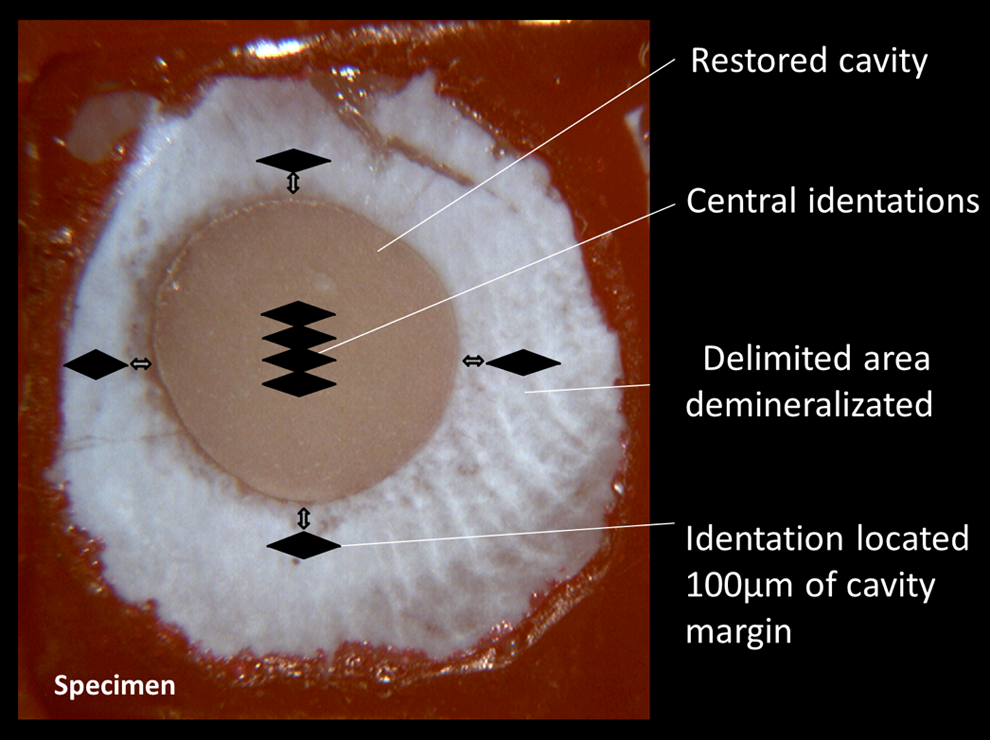
Schematic representation of superficial enamel microhardness and identation location on the restorative materials.
The specimens were longitudinally sectioned in their central area with double-faced diamond disks (no. 7020; KG Sorensen, Barueri, SP, Brazil) used at low speed (Kavo, Joinville, SC, Brazil) and under water irrigation.
The cut surface was exposed for acrylic resin inclusion and flattened. Enamel surfaces were wet-polished with 400-, 600-, and 1200-grit silicon carbide paper (Carburundum Abrasivos Ltda., Vinhedo, Brazil) using a polishing machine (PL02 RB LAB Com. Técnica Ltda, São Paulo, Brazil). Afterwards, the specimens were polished with diamond pastes (6, 3, 1, and 0.5 μm; Arotec SA Ind e Com., Cotia, São Paulo, Brazil) on cloths, under mineral oil lubrication.
Quantitative evaluation of the restorative material at a depth of 1.6 mm was performed by four central indentations at 100 μm from the restorative material surface on the floor of the cavity preparation. By means of a microhardness tester, a 25 g load was applied for 20 sec (Fig. 1). The mean of four KHN values obtained from each specimen was used for evaluation.
Demineralization of the restored enamel blocks was assessed with a microhardness tester (Pan Tec, Panambra, São Paulo, Brazil). One lane of seven indentations was made at 100 μm from the enamel–restoration interface. The indentations were made with a Knoop indenter using a 25 g load applied for 5 sec at the following depths: 30, 60, 90, 120, 150, 180, and 210 μm from the outer enamel surface and 100 μm from the enamel–restoration interface (Fig. 2). The mean of seven KHN values obtained from each specimen was used for evaluation.

Schematic representation of Knoop evaluation location in cross-sectional enamel evaluation 100 μm distant from the bonded interface, at the following depths: 30, 60, 90, 120, 150, 180, and 210 μm from the enamel surface (original magnification 40×).
Statistical analysis
The factors under study for each restorative material were depth (at two levels) and photoactivation source (at three levels) in a 2×3 factorial design.
The factors under study for superficial enamel evaluation were material (at two levels) and photoactivation source (at three levels) in a 2×3 factorial design.
The factors under study for cross-sectional enamel evaluation were material (at two levels), photoactivation source (at three levels), and depth (at 7 levels: 30, 60, 90, 120, 150, 180, and 210 μm) in a 3×2×7 factorial design.
The mean KHN values were evaluated by two way analysis of variance (ANOVA) and Tukey tests (p<0.05) for superficial enamel evaluation and material evaluation. The software employed was SANEST (EPAMIG, MG, Brazil). The mean KHN values were evaluated by three way ANOVA and Tukey tests (p<0.05) for subsuperficial enamel evaluation. The mean KHN values were compared by a Tukey post-hoc test (α=0.05).
Results
For restorative material evaluation of CR, ANOVA showed statistically significant differences for the depth factor (p=0.002). However, the photoactivation source factor and interactions between factors were not statistically significant (p>0.05). Table 2 shows the KHN values and the Tukey test results for the two depths; the KHN values of CR at the surface (0 mm) were greater than at a depth of 1.6 mm.
Means followed by different upper case letter at column indicate statistical differences (p<0.05).
QTH, quartz-tungsten-halogen; AL, argon laser; LED, light emitting diode.
For restorative material evaluation of RMGI, ANOVA showed statistically significant differences for the depth factor (p<0.05), and the KHN values were higher at a depth of 1.6 mm than at the surface (0 mm). The photoactivation source factor and interactions between factors were not statistically significant (p>0.05). Table 3 shows the KHN values and the Tukey test results for the depth factor for the restorative material evaluation of RMGI.
Means followed by different upper case letter at column indicate statistical differences (p<0.05).
QTH, quartz-tungsten-halogen; AL, argon laser; LED, light emitting diode.
For superficial enamel caries evaluation, ANOVA showed statistically significant differences for the material factor (p<0.05), and the KHN values were greater for RMGI than for CR. The photoactivation source factor and interactions between factors were not statistically significant for superficial enamel evaluation. Table 4 shows the KHN values and the Tukey's results for the material and photoactivation source factors for superficial enamel evaluation.
Means followed by different upper case letter at column indicate statistical differences (p<0.05
RMGI, resin-modified glass ionomer material; CR, composite resin; QTH, quartz-tungsten-halogen; AL, argon laser; LED, light emitting diode.
Data were submitted to three way ANOVA (α=0.05), considering the 2×3×7 factorial model to observe the factors and their interactions for subsuperficial enamel evaluation. ANOVA showed statistically significant differences for the material (p<0.05) and photoactivation source (p<0.05) factors. The KHN values were higher for RMGI than for CR. Among the various photoactivation sources, the mean KHN values were the highest with LED activation. The depth factor, as well as double and triple interactions between factors, were not statistically significant for subsuperficial enamel evaluation (p>0.05). Table 5 shows the KHN values and the Tukey test results for the material and photoactivation source factors for cross-sectional enamel evaluation.
Means followed by different upper case letter at column and lower case letter at row indicate statistical differences (p<0.05)
RMGI, resin-modified glass ionomer material; CR, composite resin; QTH, quartz-tungsten-halogen; AL, argon laser; LED, light emitting diode.
Discussion
According to the results of the present study, the first null hypothesis (that superficial enamel KHN values around the two restorative materials cured by different light-curing devices were not different) was accepted. The second null hypothesis (that cross-sectional enamel microhardness around the two restorative materials cured by different light-curing devices was not different) was rejected. The third null hypothesis (that there was no difference between restorative materials in terms of KHN values) was rejected.
In the present study, there were no differences in the material KHN results at 0 or 1.6 mm in terms of the photoactivation source with both materials. In addition, the fluency of 24 J/cm2 was standardized for all groups, which was enough for proper polymerization of the dental materials evaluated. It has been demonstrated that at an irradiance >10 J/cm2, there is a tendency for the degree of conversion to stabilize for CRs. 24,25 Furthermore, factors that could influence the transmission of light, such as the thickness of the restorative material and the distance of the light tip to the restoration surface, were standardized. 26
Within the RMGI layer activated by light, the setting by an acid base reaction and by a polymerization reaction occur simultaneously. 6,27 The acid base reaction and polymerization compete with and inhibit one another early during the RMGI reaction. 27 As evaluated in the present study, Kakaboura et al. 28 have affirmed that the RMGI surface, which is directly photoactivated, has a rapid polymer network formation and a strongly reduced salt formation rate.
Cefaly et al. 7 did not find statistically significant differences of microhardness values at the surface (0 mm) among LED and QTH for RGMI activation, and these results are similar to our findings. It has been demonstrated that the differences at the top and bottom are material dependent. 29 For RMGI, the KHN values were lower at the surface (0 mm), and the opposite was true at a depth of 1.6 mm. The initial KHN values (0 mm) were measured at 24 h after photoactivation. The pH cycling experiment was performed for 7 days, and the samples were longitudinally sectioned in their central area. The cut surface was evaluated by the KHN profile after this period. The third redox-mediated reaction allowed the increase of KHN values observed at a depth of 1.6 mm. 10 It has been demonstrated that the RMGI evaluated in this study presents a significant increase in KHN values at 7 days after activaction. 30 Moreover, even on unexposed regions of the RMGI material, the slow rate of chemically initiated polymerization allows the development of the acid base reaction. 28
On the other hand, CR polymerization varies according to depth. The restoration surface directly irradiated received the total amount of energy. Reflection, scattering, and absorption promote lower irradiance at greater depths, 8 thus explaining the KHN results at a depth of 1.6 mm (Table 2). As shown in Table 4, the CR fillings presented more enamel demineralization than the RMGI materials; 3,4 this result is related to the fluoride release in the RMGI material, which has a preventive effect. 3,21 The fluoride release reduced demineralization on the enamel around the restoration and along the cavity wall.
The preventive characteristic of AL irradiation has been demonstrated after fissure pit and fissure sealant activation. Das et al. 18 have reported a 47% decrease of caries depth with the use of an AL, compared with an LED as the activation source. In addition to AL activation, low-fluence enamel irradiation has shown favorable results in terms of decreased enamel demineralization. 19,31 However, the results of the present study did not show an influence of the activation source around the restorative materials. The association of a fluoride solution and AL irradiation presents a synergistic effect with a significant decrease of caries lesion depth compared with solely laser irradiation, 32 although the RMGI results were also not influenced by the activation.
Because of marginal gap formation, 33 polymerization contraction is an important factor. 24 The contraction depends upon the total power density and the combination of power density and exposure time. 33 Marginal gaps and microspaces can lead to demineralization of the cavity wall after pH cycling. In addition, the higher shrinkage stress during polymerization can lead to an increased risk of adhesive failures. 24,34
On the other hand, LED activation achieved higher KHN values along the cavity wall. In addition to the fact that fast polymerization causes shorter polymer chain lengths, 35 Asmussen and Peutzfeldt found smaller contraction with fast polymerization. 33 This fact can lead to decreased marginal gaps and microspaces as well as decreased demineralization of the cavity wall after pH cycling, in accordance with the results found in the present study. The contraction of CR depends upon the intensity and also the combination of intensity and exposure time used to deliver the energy.
Conclusions
In conclusion, AL activation had no additional benefits in preventing enamel demineralization for CR or RMGI restorations. In addition, the photoactivation source did not influence superficial enamel demineralization around the dental restoration, but LED had a more positive effect on subsurface enamel demineralization of the restorative materials evaluated. Finally, there was less development of enamel demineralization around RMGI restorations than around CR restorations.
Footnotes
Author Disclosure Statement
This work was supported by FAPESP (São Paulo Research Foundation, grant no. 2009/02240-3).