
Abstract
Introduction
I
Low-level laser therapy (LLLT) has been the subject of several studies investigating tissue repair optimization. 8 A better understanding of the cellular and molecular mechanisms involved in photobiomodulation has provided new perspectives with regard to the use of this technology. 9 The most accepted hypothesis is that red and near-infrared LLLT interacts with the mitochondria, more specifically with the respiratory chain enzyme cytochrome c oxidase in the partially reduced state, which is the terminal enzyme of the respiratory electron transport chain. 10 Increased electron transfer promotes adenosine triphosphate (ATP) production, and even small changes in ATP levels can induce changes in cellular metabolism. 10 In addition to an energy source, ATP is also an intercellular signaling molecule, 11 and this concept enables the understanding of the universality of the phenomena elicited by LLLT. 11 LLLT also regulates the redox potential to produce a more oxidized state. This modulation affects transcription factors and increases DNA synthesis, which improves cell proliferation. 9
The beneficial action of
Only a few studies have evaluated LLLT in bone subjected to IR. 21,22 Da Cunha et al. 21 investigated the effects of LLLT (780 nm, 40 mW, 4 J/cm2, 100 sec, 0.04 cm2 beam area, four points, seven sessions with 48 h intervals) on rat femurs, and histological analysis showed enhanced marrow cellularity, higher numbers of osteocytes and Haversian canals, and a significant increase in osteoblast activity. A radiographic analysis showed higher bone density in LLLT groups 1 day prior to radiotherapy and 4 weeks after radiotherapy. This study revealed a positive effect of LLLT on rat bone exposed to IR. In another study, Freire et al. 22 evaluated the preventive effect of LLLT in rats femur undergoing IR. The surgical defect and the LLLT sessions (780 nm, 40 mW, 4 J/cm2, 100 sec, 0.04 cm2 beam area, four points around the surgical wound, seven sessions with 48 h intervals) were performed prior to IR. The authors reported an increment of osteocytes and Haversian canals in LLLT groups.
The hypothesis of the present study is that LLLT can benefit the repair process of IR radiated bone. Digital histomorphometry analysis was used to quantify the area of newly formed bone in the initial repair period. The aim of the present study was to evaluate the LLLT stimuli in the newly formed bone area in surgical defects of rat tibiae undergoing IR.
Materials and Methods
This study was approved by the Committee on Research Ethics of the Universidade Federal de São Paulo – UNIFESP (approval No 0525/06).
We used 72 healthy, young adult male albino Wistar rats (Rattus norvegicus) between 90 and 105 days of age, weighing from 300 to 340 g. The rats were obtained from and maintained during the experiment at the Centro de Desenvolvimento de Modelo Experimental (CEDEME) of Universidade Federal de São Paulo - UNIFESP. The animals were under controlled temperature conditions, light–dark periods of 12 h, and unrestricted access to water and food.
The animals were distributed into four groups of 18 each: Group I, sham control; Group II, LLLT; Group III, irradiated with IR; and Group IV, irradiated with IR and LLLT (Fig. 1). Only one tibia per animal was used.
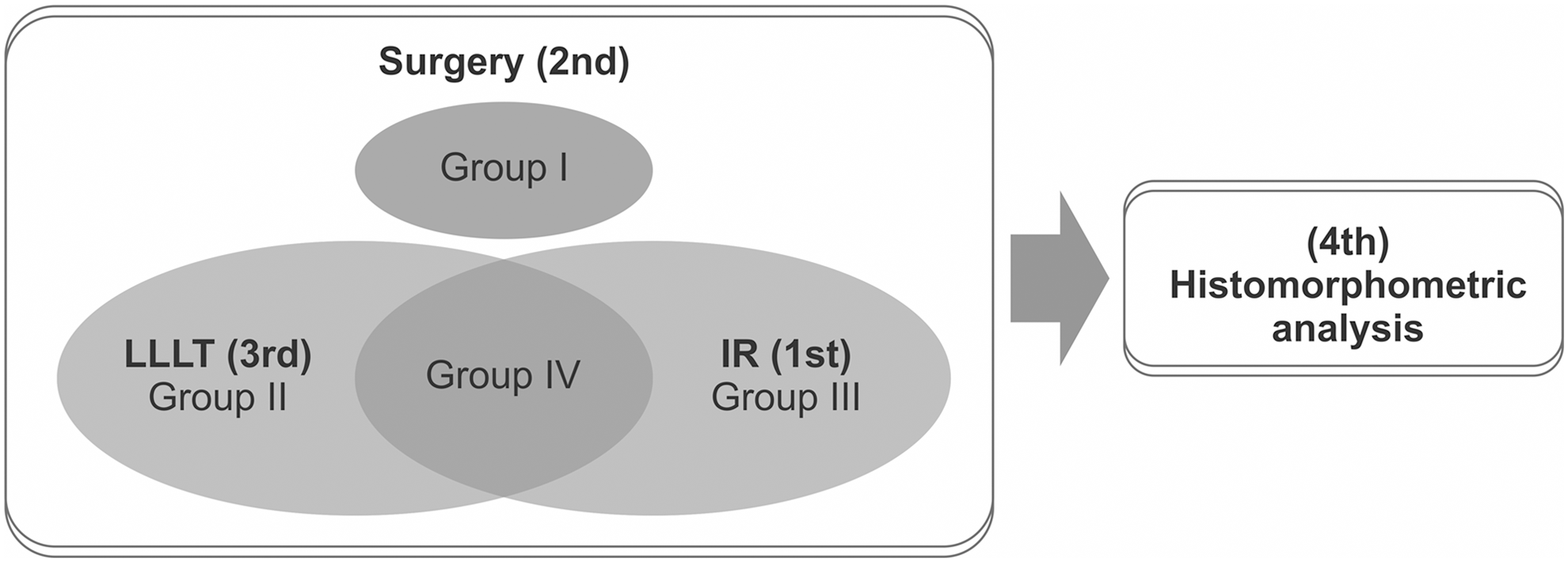
The design of the experiment. LLLT, low-level laser therapy; IR, ionizing radiation; Group I (control); Group II (LLLT); Group III (IR); Group IV (IR and LLLT).
IR procedure
Anesthesia was induced by intraperitoneal injection of ketamine (70 mg/kg) and xylazine (10 mg/kg). The animals in Groups III and IV were lined up on a perforated acrylic plate and immobilized with nylon straps attached to their front limb and lower part of the hindlimb. A simulation was performed prior to IR (Acuity C, Varian Medical Systems, Inc., Palo Alto, CA) to ensure that all tibiae were within the radiation field (26×16 cm) and received the IR dose uniformly. The tibiae were exposed to a single fraction of 30 Gy 21 –25 of gamma radiation with a dose rate of 1.10 Gy/min and a skin source distance of 80 cm for ∼27 min in a cobalt-60 unit (CGR, MeV model Alcyon II cobalt unit, France) (Fig. 2a).
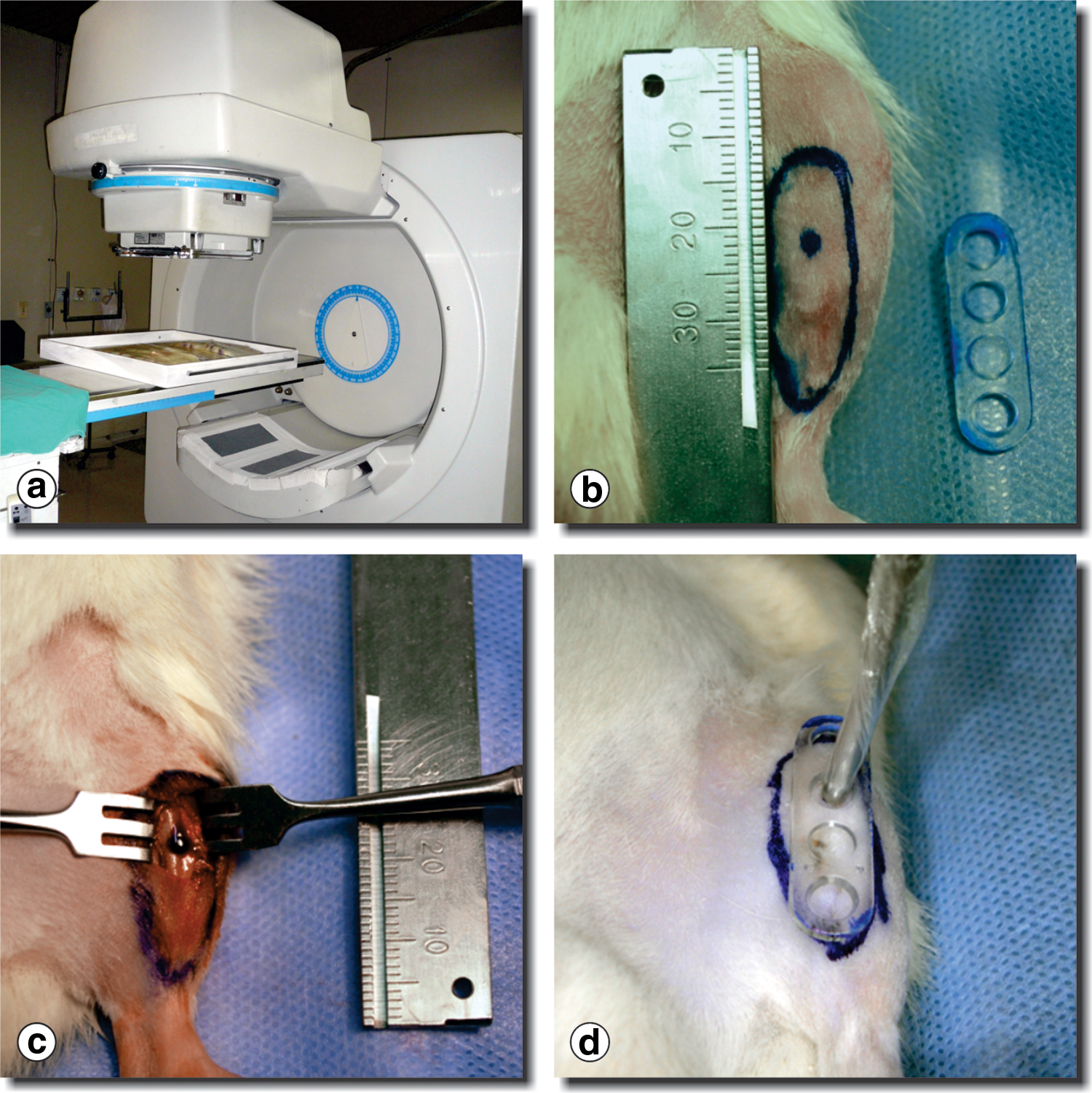
Sequence of procedures performed.
Surgical procedure
All animals were operated on under anesthesia with ketamine (70 mg/kg) and xylazine (10 mg/kg). Groups III and IV underwent surgery 28 days after IR. 26 Hair was removed from the hindlimb with an electrical clipper, using 2% chlorhexidine for antisepsis.
To ensure that LLLT would be applied in the same location as the bone defect, a plastic guide was positioned over the animals' skin before surgery, with the top edge on the tibia patella and the hole indicating the location on the tibia that would be drilled (Fig. 2b). The medial surface of the tibia was exposed through a rostrocaudal incision measuring ∼1 cm in length. A noncritical sized bone defect measuring 2.5 mm in diameter 12,13,15,17 was made in the diaphysis portion until reach the medullary cavity, using a spherical diamond drill (KG Sorensen, SP, Brazil) powered by an electric motor (Driller, SP, Brazil) coupled to a handpiece at ∼1600 rpm (Fig. 2c). The surgery was performed under constant irrigation with sterile saline. The suture was secured using a 4.0 nylon monofilament. Oral analgesic (ibuprofen, ∼15 mg/kg/day, Aché, Guarulhos, SP, Brazil) and intramuscular antibiotic (benzathine benzylpenicillin, 600,000 U, 20,000 UI/kg, IM, Eurofarma, SP, Brazil) were administered after surgery.
LLLT procedure
Three LLLT sessions were performed, the first just after surgery, the second 48 h after surgery, and the third 96 h after surgery. LLLT was applied to the animals in Groups II and IV. Groups I and III underwent the same procedures with the power switched off. The plastic guide was used to standardize the position of LLLT irradiation (Fig. 2d). For the LLLT sessions, the animals received half the anesthetic dose.
The laser irradiation consisted of a continuous operation, performed perpendicular to the tissue, transcutaneous, at only one point. Table 1 summarizes the laser parameters. The laser equipment (DMC, São Carlos, Brazil) was calibrated before irradiation session with power meters (Coherent, Inc., Santa Clara, CA).
Euthanasia
The animals were euthanized by exposure to 70% carbon dioxide at a rate of 20% chamber volume/min. Six animals from each group were euthanized on days 7, 14, and 21 after surgery. 27
Histological processing
The operated lower legs were dissected and the tibiae were fixed for ∼24 h in 10% buffered formalin and then in alcohol. Next, the tibiae were decalcified in 10% ethylenediaminetetraacetic acid for ∼24–36 h.
Once decalcified, the tibiae were incised at the proximal and distal regions 2 mm from the bone defect. After histological processing (Leica Microsystems GmbH, Wetzlar, Germany), the samples were embedded in paraffin for the preparation of histological sections on a semiautomated microtome (Leica Biosystems Nussloch GmbH, Nussloch, Germany). Four longitudinal sections were obtained from each tibia at a thickness of ∼3 μm. The samples were further processed with a modified Masson's trichrome stain.
Digital image analysis
Image acquisition
All the images were taken by the same pathologist, who was unaware of the treatment conditions, using a trinocular microscope with plan-achromatic objectives coupled to a camera (Olympus, Center Valley, PA) and a computer. Optical microscopy (Olympus, Center Valley, PA) at 2× magnification was used to identify the site with the highest incidence of newly formed bone at the bone perforation. From this point, four consecutive, clockwise images were acquired at 200× magnification (Fig. 3a).

Sequence of images of the measurement process of new bone formation using digital image analysis.
Selection of newly formed bone areas
The tagged image file format (TIFF) images were transferred to Adobe® Photoshop® (Adobe Systems Incorporated, San Jose, CA). The areas of new bone formation were delineated by the Magic Wand tool (Fig. 3b). In the Select option, the Inverse function was selected to keep the area of interest; using the Eraser tool, the image corresponding to the remaining bone surgery infiltrate, consistent with granulation tissue (or in more advanced stages, medullary bone tissue) was erased. Again, in the Select option, the Deselect function was used to keep only the image of areas of newly formed bone (Fig. 3c).
Measurement of newly formed bone areas
The selected areas were measured using Image Tool, version 3.0 (Department of Dental Diagnostic Science at the University of Texas Health Science Center, San Antonio, TX). A specific calibration was performed and the result was expressed in μm2. The image was then converted to gray scale (Fig. 3d,e). Using the Analysis tool and the Find object function, the bar of the threshold was manually adjusted and the areas that did not correspond to the newly formed bone, which we call “negative areas,” were automatically defined and numbered in red (Fig. 3f–i). Next, the Deselect all option was selected, and only the negative areas were manually selected (Fig. 3i). Using the Analyze function, the software measured the negative areas selected in μm2 (Fig. 3j).
Calculation of newly formed bone areas
All measurements were exported to Microsoft Office Excel 2007. The sum of the negative areas was subtracted from the total image area (area=77,571.77). The result corresponded to the area of newly formed bone.
Statistical analysis
The Power and Sample Size tools in Minitab 15 (Minitab Inc., State College, PA) were used to determine if the sample size was representative. Intraclass correlation (ICC) was used to measure the reliability between the two histological readings. The Kruskal–Wallis test was used to compare the mean areas of bone formation among the four groups on days 7, 14, and 21. The Mann–Whitney U test compared the independent samples in pairs to identify which groups were significantly different. The statistical result of each comparison was corrected using the Bonferroni correction. The confidence interval (CI=95%) measured the reliability of an estimated range of values. SPSS software version 16 (IBM Corporation, Armonk, NY) was used to analyze the data. The rejection level was set at p≤0.05.
Results
The sample power was 78.35% (0.7835). ICC showed statistical significance (p<0.001) between the two evaluations for all groups and at all periods. When comparing the four groups at each period, all groups showed a statistical increase in the mean area of newly formed bone on day 21 (p<0.006). The mean area of newly formed bone was significantly lower in the group with IR (p<0.006) than in all the other groups. On days 14 and 21, the mean area of newly formed bone was similar in Groups I, II, and IV (Fig. 4).
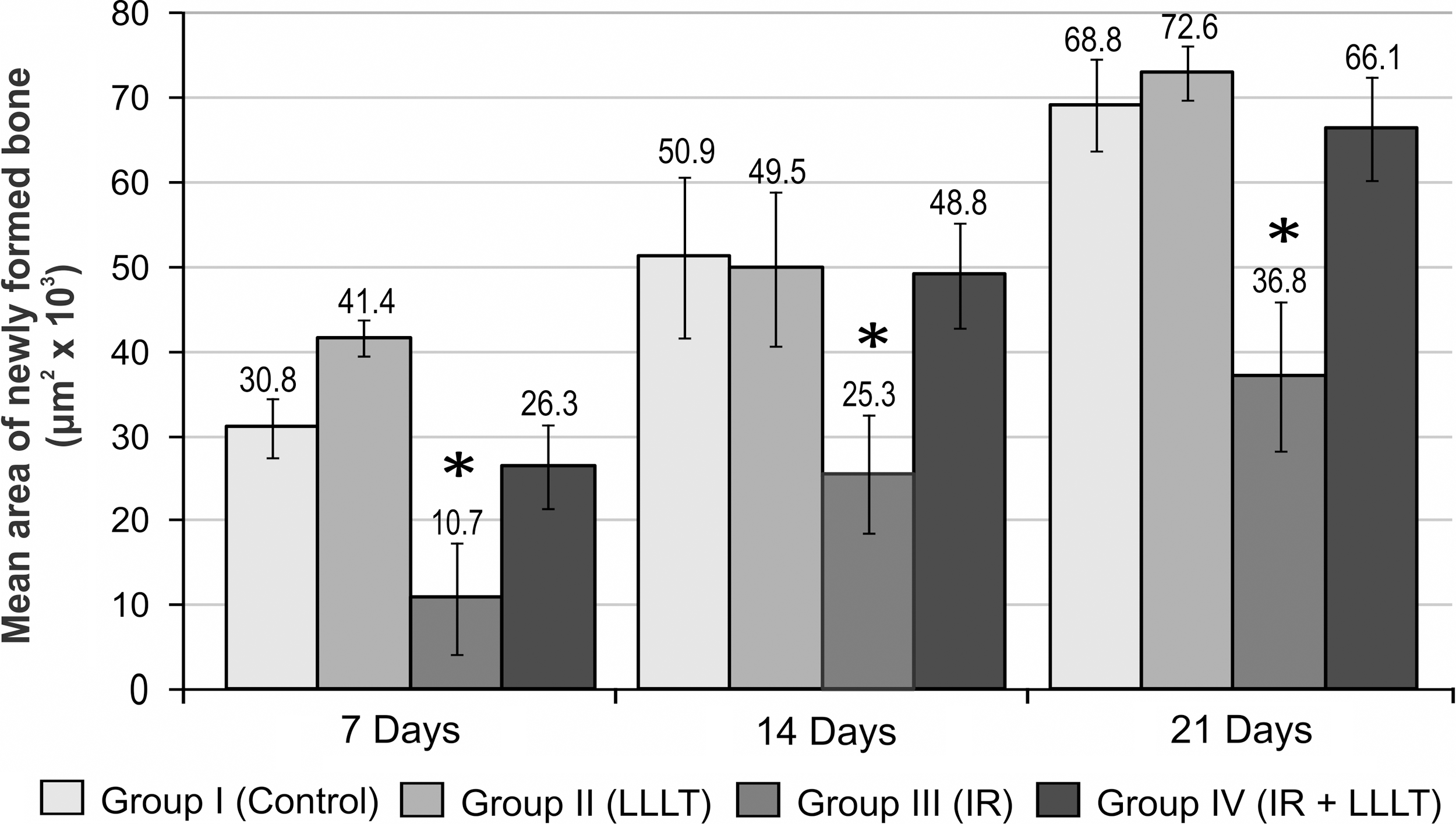
Comparison of the mean area of the newly formed bone (μm2) between the four groups on days 7, 14, and 21. Kruskal–Wallis test.
Figure 5 summarizes our findings on comparison of the groups in pairs, with their respective control groups on days 7, 14, and 21.
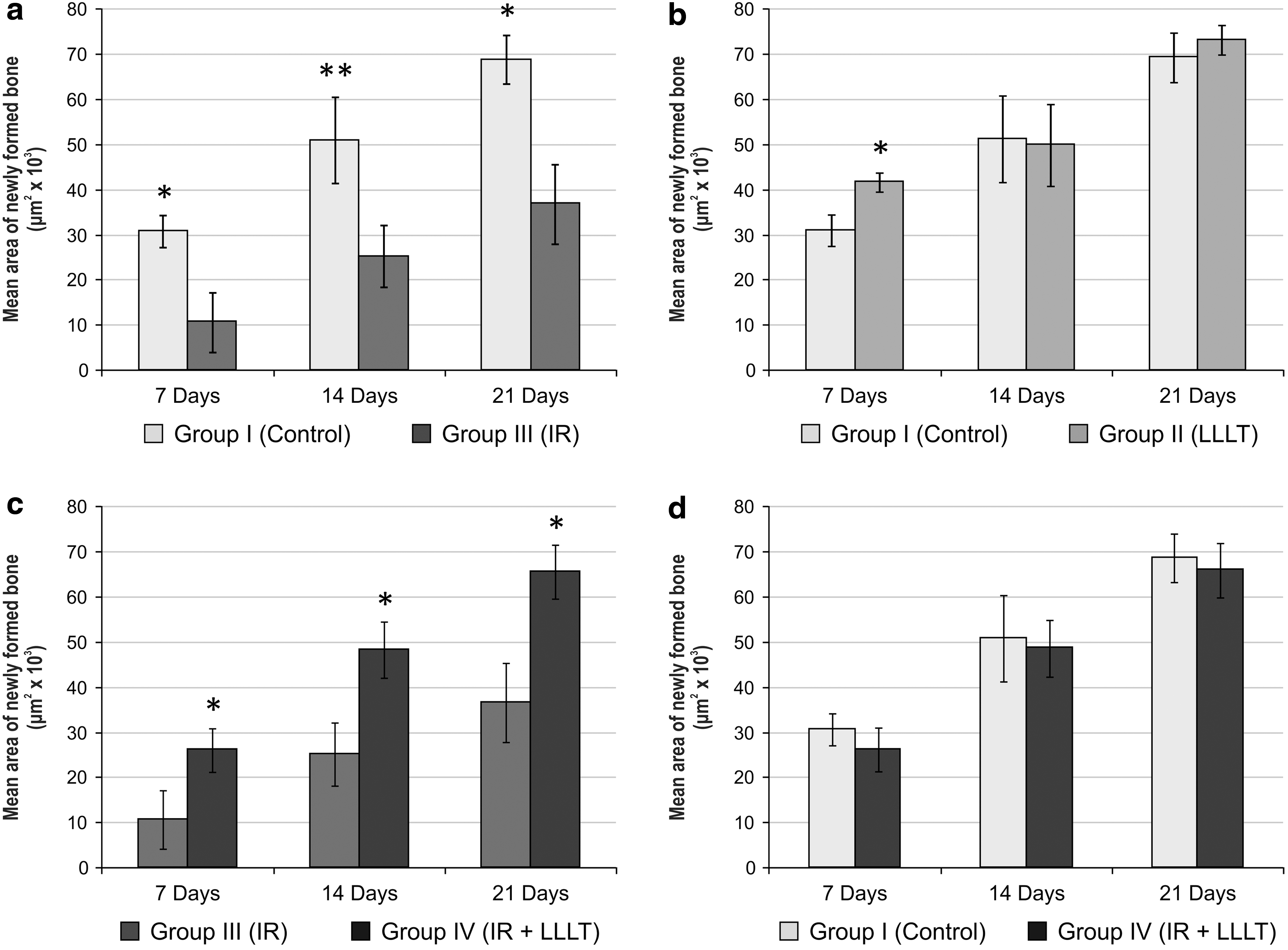
The analysis on day 7 revealed that, in Group III, the repair process was compatible with fibrovascular regeneration, whereas Groups I, II, and IV exhibited newly formed bone tissue (Fig. 6). On day 14, Group I presented a larger area of new bone formation than Group II; however, Group II showed a markedly advanced stage of repair characterized by bone reabsorption and the maturation of medullary tissue (Fig. 6). For this reason, the mean area of newly formed bone in Group II was smaller on day 14, but not significantly different than that in Group I (Fig. 5b). On day 21, in most cases, Groups I and II presented complete marrow repair. Bone repair was at an advanced stage in Group IV, and slower repair was still noted in Group III (Fig. 6).

Photomicrographs of the four groups on days 7, 14, and 21 at 200× magnification with optical microscopy. Masson's Trichrome staining. The “A” arrow indicates osteoid. The “B” arrow indicates marrow repair. The “C” arrow indicates a less organized bone. The “D” arrow indicates bone in a more advanced stage of maturity and with an organized structure. LLLT, low-level laser therapy; IR, ionizing radiation.
Discussion
Technological advances in RT equipment and procedures such as intensity modulated irradiation therapy and three-dimensional conformal therapy significantly decrease the incidence of ORN but do not completely eliminate the risk of developing radiation-induced bone atrophy. 7,28 The presence of bone with optimal repair potential is an important factor in the prognosis of functional and esthetic rehabilitation of patients after cancer treatment. 7 The present study demonstrated the positive effect of LLLT during the initial phase of the repair process in the tibiae of rats exposed to high doses of IR. We observed a more pronounced amount of newly formed bone, very similar to that in the control group. Although the beneficial action of LLLT on bone subjected to IR has been corroborated by similar studies, 21,22 more detailed studies with different parameters are necessary to obtain a deeper understanding of this approach prior to its use in clinical trials.
Recommended LLLT doses in the literature vary widely because of the large number of adjustable parameters on the equipment, the lack of standardized research protocols, and many beam measurement and dose calculation errors. 29 In the present study, the 2 J deposited energy, in accordance with previous studies with similar energy, 13,19 was effective in terms of bone repair, particularly observed in Group II (LLLT) (Fig. 5b). The wavelength (808 nm) employed corresponded to near infrared, which achieves deep tissue penetration. It is noteworthy that the benefits for bone repair are not only defined by the direct interaction of bone tissue cells with LLLT, but the laser action enables an improvement in vascularization to enhance the supply of circulating cells, nutrition, and oxygen. 12,16,17 Use of the LLLT protocol on 3 alternate days has been described in several studies, 15,17,20,21 and the dose employed here resulted in a significant increase in the mean area of new bone formation at Group IV (IR and LLLT) (Fig. 5d). Silva Júnior et al. 20 in their comparative study, observed there was a significant increase in new bone formation in the group exposed to three sessions a week of irradiation compared with the control group, but there was no increase in the group irradiated over 12 sessions. The author concluded that LLLT yielded the best results when applied during the proliferative and earlier stages of differentiation of immature precursors, but not during the later stages, in agreement with the literature. 12 –18
In the present study, the IR dose was considered appropriate because all animals tolerated this protocol and there was a significant difference in the mean area of newly formed bone between Groups I (Control) and III (IR) at all time points (Fig. 5). Compared with other groups, we observed a smaller mean area of newly formed bone and a delay in the repair process in Group III on all days analyzed (Fig. 4). These results are consistent with the findings in the literature, 23 –25 revealing significant bone changes using a single IR dose of 30 Gy in rats. The date of surgery at 28 days after IR was based on a study by Kiyohara et al., 26 who irradiated Wistar rat femurs with a single 30 Gy dose and evaluated the samples using histomorphometry and binarized radiographs at 0, 1, 2, 3, and 4 weeks. At the end of the study, the effects of IR were well settled and more pronounced than in the initial periods.
There was a significant increase in the area of newly formed bone in Group IV (IR and LLLT
An outstanding result was that we did not observe a statistically significant difference in the newly formed bone repair mean area between Groups I (Control) and IV (IR and LLLT) (Fig. 5). This result demonstrates the photobiostimulation effect of LLLT on bone undergoing IR. One hypothesis of this action is that the pathological state of the tissue may have determined the optimal conditions for LLLT performance. 10,30 The literature reveals that cellular pH and cells' reduction potential have an important influence on the response to irradiation; the laser effect is greater at lower pH, and the potential is reduced. 10
For a future approach, with additional immunohistochemical analysis, further studies should assess angiogenesis, osteoblast activity, the growth factors involved in the repair process, and the osteoblast/osteoclast recruitment ratio. In addition, high-resolution scanning electron microscopy should be considered in upcoming analysis. 31 We are aware that the sample size of this study was small, and that the defects were not critical; however, the results were statistically representative and allowed comparison of the groups with their respective controls for the same conditions and parameters. With regard to the differences of embryonic origins between long bones and irregular bones of the face, their repair process is very similar. The use of animal models is often an essential step in evaluating the development of new materials, techniques, or technologies applied to bone repair. 32
It is well known that IR causes dose-dependent structural changes on bone tissue. 6,7 With further understanding about potential benefits of LLLT, it would be possible to prevent radiation-induced complications or to improve the treatment outcomes when performing curettage of necrotic bone, resections, and patient rehabilitation procedures, where there is a need to stimulate the bone repair process.
Conclusions
In conclusion, this experiment has revealed that LLLT increased the newly formed bone area at the initial phase of the tibia repair process in rats exposed to IR. More detailed studies under the same parameters will be developed in order to determine which conditions have influenced these results.
Footnotes
Acknowledgments
This study received support from the Research Support Foundation of the State of São Paulo - FAPESP/ - research process: 10/51626-9. We thank Dr. Luciana Almeida-Lopes, coordinating professor of Nupen – Research and Education Center for Photo Therapy in Health Sciences, for scientific support, and Jimmy Adans, Francisco Gustavo da Silveira Sousa Junior, and Ricardo Iannuzzi for manuscript preparation. We also thank Renaldo Mansini, Jr. of DMC Equipamentos Ltda., São Carlos, Brazil, for support with the laser equipment.
Author Disclosure Statement
No competing financial interests exist.