
Abstract
Introduction
T
These morphological changes promote a reduction of collagen type I (thick fibers) and a change of aggregation and collagen alignment in the injured tendons, slowing the repair process and also making injured Achilles tendon susceptible to total ruptures. 5 –7
Low-level laser therapy (LLLT) has been used to accelerate the repair of Achilles injuries and tendinopathies, once LLLT generates synthesis of nucleic acid and cellular divisions in fibroblasts, while also increasing the quantity of mRNA pro-collagen types I and III, and improving the alignment of collagen fibers, facilitating and optimizing the Achilles tendon repair process. 7 –10
The widespread use of different types of LLLT is associated with a variability of effects. There are some studies reporting accelerated tendon repair; 11 modulation in pain, strength, and function; 12 increases in the organization of collagen fibers; and consequent improvements in tendon regeneration 10 as a result of LLLT application to Achilles tendon injuries.
Although there are numerous studies reporting promising results with near-infrared LLLT in relation to the proliferation and alignment of collagen, 10 –12 there are also a wide variety of parameters used (mean power and fluence), and there is still a lack of data determining how to achieve the best results with LLLT. Therefore, the aim of the present study was to assess the effects of LLLT, with a wavelength of 780 nm (near infrared), a mean power of 70 mW, and fluence (ΔE) of 17.5 J/cm2, on the repair process of partially injured Achilles tendons in rats.
Materials and Methods
This study was approved by the Ethics Committee of the Universidade Federal de São Paulo - protocol number 0074/2011.
Sixty-five male 12-week-old Wistar rats (Rattus norvegicus: var. albinus, Rodentia, Mammalia), weighing between 270 and 300 g, were used. The animals were kept in cages of standard polypropylene, in a light/dark cycle of 12 h, with temperatures of ∼20°C and humidity of 65%. They received water and rat chow ad libitum.
Achilles tendon injury procedure
Sixty animals were randomly anesthetized with an intraperitoneal injection of ketamine hydrochloride (100 mg/kg) and xylazine hydrochloride (50 mg/kg). The five remaining animals were not given anesthesia.
After anesthesia, manual trichotomy of the areas corresponding to the Achilles tendon of the right hindpaw was performed. The animal was positioned at the injury equipment (Fig. 1). The right hindpaw was placed on the equipment base, and mild traction was exerted through ankle dorsiflexion until the dorsal region of the paw rested against the base of the equipment (Fig. 2A). Finally, a weight of 186 g was released from a height of 20 cm onto the Achilles tendon of each animal, corresponding to a potential energy of 364.9 mJ at the time of trauma. 6,7
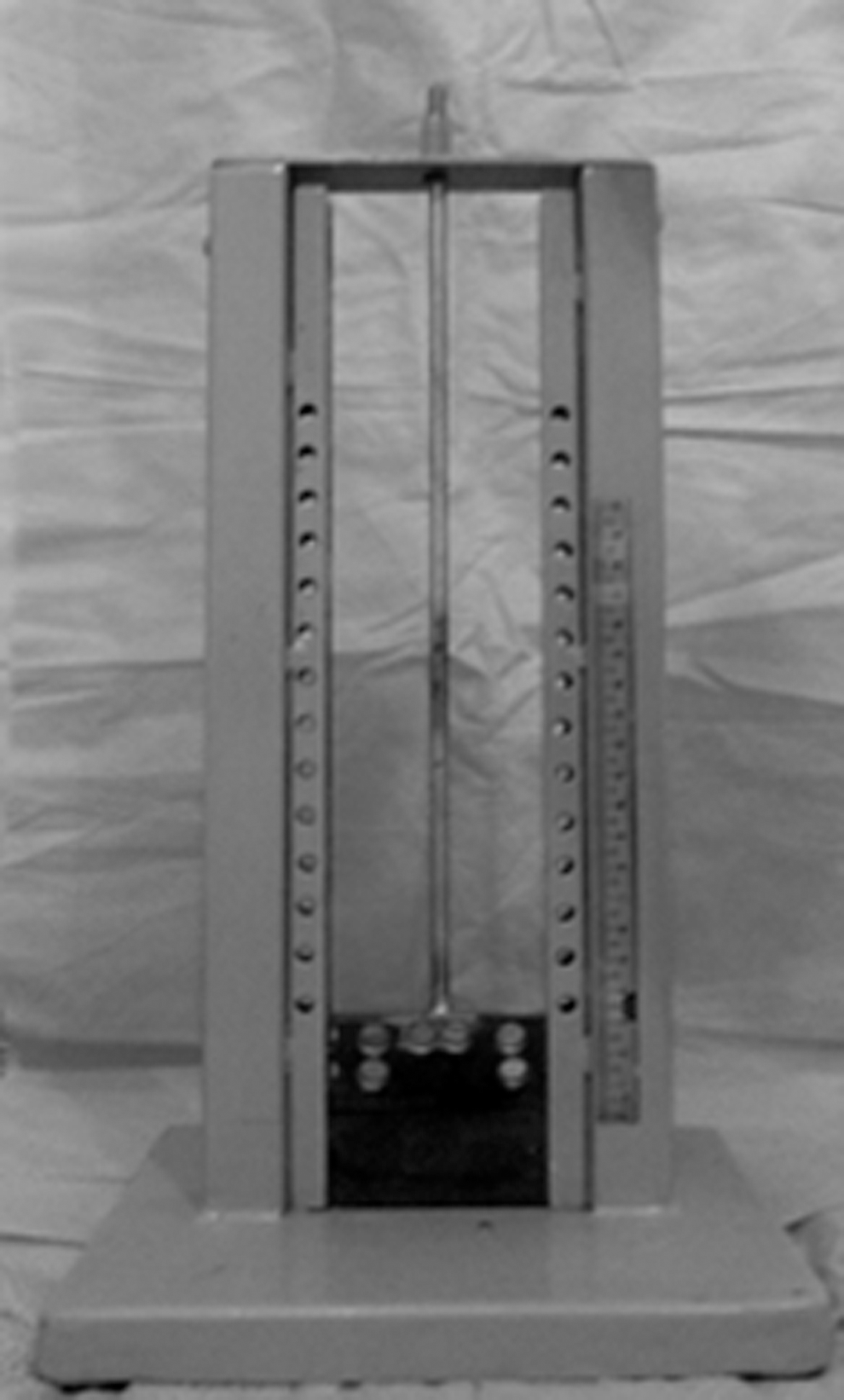
Equipment used to partially injure the Achilles tendons.

Photographs of the (
Distribution of the groups
After the Achilles tendons of the 60 animals were partially injured, they were randomly distributed into seven groups: • Sham 1: 10 injured tendons that were submitted to simulated LLLT for 1 day • LASER 1: 10 injured tendons that were submitted to LLLT application for 1 day • Sham 3: 10 injured tendons that were submitted to simulated LLLT for 3 days • LASER 3: 10 injured tendons that were submitted to LLLT application for 3 days • Sham 7: 10 injured tendons that were submitted to simulated LLLT for 7 days • LASER 7: 10 injured tendons that were submitted to LLLT application for 7 days • The other 5 animals (10 tendons) were placed in the control group, on which no procedures were performed
Laser treatment
The LLLT equipment was used with the semiconductor active medium AsGaAl (MMOptics), λ=780 nm (near-infrared), a beam area of 0.04 cm2, and a mean power of 70 mW.
The laser was applied once a day to central portion of the Achilles tendon of the injured animals. The laser treatment started 1 min after induced injury, and was applied with ΔE=17.5 J/cm2 for 10 sec using a total final energy of 0.7 J. The contact technique and continuous emission were used in all irradiations (Fig. 2B). The animals were treated for 1 day (LASER 1), 3 consecutive days (LASER 3), or 7 consecutive days (LASER 7). 6,7,13
The animals in the sham groups (1, 3, and 7) only received simulated LLLT application, with the device turned off. However, contact was maintained between the equipment and the injured area for the same time as during the active treatment.
Euthanasia
The animals in groups LASER 1/Sham 1, LASER 3/Sham 3, and LASER 7/Sham 7 were euthanized (anesthetic overdose) 24 h, 4 days, and 8 days after the induced injury, respectively. The animals in the control group were euthanized on the last day of the experiment (8th day).
Processing of the samples
After the animals were euthanized, the tendons of the two hindpaws were removed from the animals in the control group, as well as the 60 tendons (right hindpaw) of the animals belonging to the other groups (Fig. 2C).
The tendons were removed surgically, and immediately after this procedure, the tendons were washed in saline solution (0.9%) and then fixed for 12 h in paraformaldehyde 4% in Millonig 0.1M buffer (pH 7.2–7.4).
After fixation, the tendons were washed in water and dehydrated in increasing solutions of ethyl alcohol (from 70% to 100%) for 45 min in each one. Next, they were diaphonized in xylene (two baths of 45 min each), and included in paraffin, positioned in such a way as to obtain longitudinal slices. The slices were made with a microtome, with thicknesses of 7 μm, to analyze the birefringence (tissue alignment), and of 5 μm for the picrosirius red technique.
Each slide was prepared with two slices of each tendon for staining with picrosirius red and birefringence. This process was repeated three times. Therefore, three nonconsecutive slides were obtained for each analysis from each animal studied.
All slices were de-waxed, hydrated, and submitted to the methods listed subsequently.
Birefringence
Analysis of the alignment of collagen fibers was performed using birefringence, as described by Vidal. 2 The slides of each group were immersed in distilled water (refractive index n=1.333) for 30 min, covered with a slip and analyzed by a microscope with polarized light and a 10×/0.22 lens, a 0.9 condenser, a Sénarmont λ/4 compensator, and monochromatic light (λ=546 nm), obtained through a Leica interference filter.
Three measurements were obtained with the tendon axis at a 45 degree inclination in relation to the polarizer and analyzer, calculating the arithmetic mean of the tendon alignment in each sample. Finally, the results of the measurements, in degrees, were transformed into nanometers (nm) by multiplying them by 3.03. 7,14,15
Picrosirius red
Ten random areas (of each tendon) were analyzed under polarized light, stained in 0.1% sirius red solution, in saturated picric acid. Five areas were from the proximal region, and the other five were from the distal region.
The images were obtained using a CoolSNAP™ Pro cf camera, coupled with a Nikon Eclipse-E800 microscope. The measurements were made at 100× magnification (objective 10×), with the assistance of Image-ProPlus, version 4.5.
The analysis identified the different colors (polarization in green, type III collagen fibers; and polarization in red and yellow, type I collagen fibers), 16 and quantified the area corresponding to each color. The areas of each polarization were summed by slide, and the percentages of each type of polarization, in relation to the total area, were calculated and analyzed. The results were expressed as a mean percentage of the two different types of collagen fibers.
Statistical analysis
The Statistical Package for Social Sciences (SPSS version 15.0) was used for statistical analysis, with the level of significance set at 5% (p≤0.05). The Shapiro–Wilk and Levene tests were used to assess the distribution and homogeneity of the data, respectively. The parametric data were reported in mean and standard deviation values, and tested by ANOVA of one factor and (post-hoc) Tukey's test or the Games–Howell test, when there was no homogeneity of the variances. The nonparametric data were reported in median and interquartile range values, and were assessed by the Kruskal–Wallis test and (post-hoc) the Mann–Whitney test and Bonferroni adjustment.
Results
Table 1 presents the data of the control, LASER, and Sham groups. For collagen alignment, statistically significant differences (p<0.05) were only found in the comparison between the control group with Sham 1 and Sham 3 groups, which exhibited the most disorganized collagen fibers. The other groups (Sham 7, LASER 1, LASER 3, and LASER 7) did not reveal any significant differences (p>0.05) in comparison with the control group, that is, they exhibited a collagen fiber alignment similar to normal. In terms of collagen type (I and III), significant differences (p<0.05) were found when comparing the control group with Sham 3, LASER 1, LASER 3, and LASER 7 groups. These experimental groups exhibited higher percentages of collagen type I, and lower percentages of collagen type III.
The intergroup analysis (Sham 1, 3, and 7 vs. LASER 1, 3, and 7) for collagen alignment (Fig. 3) in relation to the number of applications (1, 3, and 7) did not reveal significant differences (p>0.05).
Photomicrography of collagen fibers alignment (birefringence) at 10×:
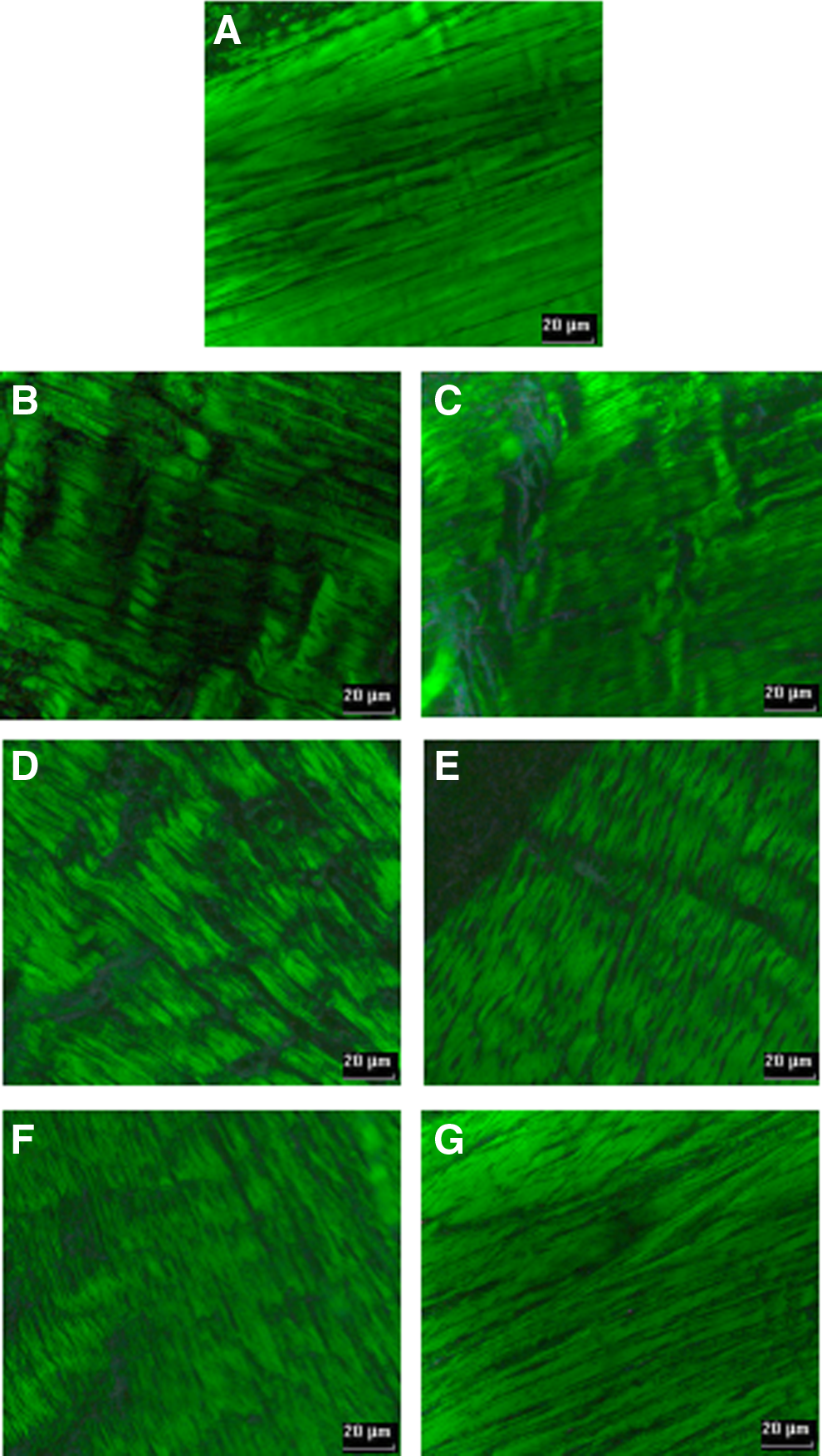
The same analysis for collagen composition (Fig. 4) only showed significant differences (p<0.05) when comparing the following groups: LASER 3 versus Sham 3 and LASER 7 versus Sham 7. The LASER groups exhibited a higher percentage of collagen type I and a lower percentage of collagen type III.

Photomicrography of the collagen types (I and III) in objective 10×:
Discussion
LLLT has been widely used in clinical practice, with promising results in Achilles tendon repair because the long period that it takes the tendon to heal. 7 Therefore, the present study investigated the effect of near-infrared LLLT on the realignment and proliferation of collagen fibers in partially injured Achilles tendons in rats.
Although different reports exist in relation to the etiology of these injuries and their interaction with LLLT, there is still a lack of information regarding the repair process and the best parameters and application techniques in these situations. 17,18 Consequently, different experimental models have been elaborated to better understand the laser–tissue interaction. The Achilles tendon injury used in this study has been used in a number of studies 6,7,18,19 aiming to assess the effects of certain types of LLLT on the alignment of collagen fibers, as well as the stimulation and proliferation of collagen.
There are also studies that have shown, by means of ultrasonography, that this type of trauma promotes a partial injury in the central portion of the Achilles tendon in rats, with<10% variation. For this reason, this method can be used and reproduced in studies that aim to understand the injury and repair processes of Achilles tendinopathies. 9
As seen in the abovementioned reports and in the results of this study, the method of direct trauma was effective in promoting the misalignment of collagen fibers and changing the composition of the collagen (types I and III) of injured Achilles tendons. Misalignment of collagen fibers in injured tendons causes functional disabilities and a reduction in tensile strength, leaving the tendon more susceptible to complete ruptures. 6,10,11 The realignment of tendon fibers in all of the groups in the present study was assessed. Birefringence was chosen, because the literature contains many reports of its excellent effectiveness in relation to this purpose. 6,7,10,11,18
Exactly how LLLT realigns the collagen fibers of injured tendons is not widely known. However, the LLLT used in the present study may have caused an increased proliferation of fibroblasts, stimulating growth factor release and increasing the deposition of collagen in the injured area. 11 It may also have stimulated the extracellular matrix and changes in fibrillar collagen structures, as the electromagnetic energy offered by LLLT, with an elevated mean power interacting with collagen molecules, generates structural changes and fiber realignment. 10,20
Bjordal et al. 21 reported that some wavelengths (632, 820–830, and 904 nm) tended to stimulate the fibroblastic metabolism more efficiently. However, the near-infrared wavelength of 780 nm also showed positive results in increasing fibroblast cell proliferation. 11 These wavelengths are within the range (760–840 nm) of those that are less absorbed by superficial chromophores, resulting in greater tissue penetration 8 and, consequently, facilitating the mechanisms through which LLLT promotes collagen realignment.
The literature contains different reports showing the efficiency of LLLT for this purpose. Neves et al. 18 demonstrated the collagen realignment of Achilles tendons submitted to the same method of injury as in this study, and treated with LLLT. However, contrary to the present study, the best results were obtained with a treatment time of 5 days (one application per day). Oliveira et al. 7 and Wood et al. 6 also reported collagen realignment under LLLT application for 1,3,5, and 7 consecutive days (one application per day). The results confirmed that five applications attained the best alignment parameters, when compared with the normal alignment situation.
This study corroborates the results of those studies. Similar results were obtained in all of the treated groups in relation to near-normal levels of collagen realignment, even using different parameters and doses. However, contrary to the abovementioned studies, the best collagen alignment results were obtained after 7 consecutive days of treatment. In these studies, 6,7,18 a wavelength of 830 nm was used, which is higher than that used in the present study.
Although this study reported near-normal levels of collagen realignment, perhaps the same levels of realignment would have been achieved, with fewer applications, if the wavelength had been increased. It is probable that the wavelength is a significant factor in obtaining satisfactory levels of collagen realignment in injured tendons.
The change in composition of collagen fibers in injured Achilles tendons is also considered a complicating factor in their repair process. Therefore, the present study also assessed the presence of collagen types I and III. A reduction of type I (thick fibers) and a consequent increase of type III (thin fibers) could result in chronic pain, and even complete rupture of the tendon. 6,8 For this purpose, the picrosirius red staining process was used, as it has been reported as an efficient method for this type of analysis. 6,11,18
Although the mechanisms of the tendon repair (type of collagen) with LLLT have not yet been fully clarified, it seems to increase the quantity of mRNA procollagen types I and III. 8,9 The LLLT used in this study could have stimulated fibroblastic activity and proliferation. There are reports in the literature stating that a wavelength of 780 nm promotes this phenomenon efficiently, which increases the collagen synthesis. 11
Furthermore, near-infrared LLLT (780 nm) can modulate inflammatory processes, 22,23 including in Achilles tendons injuries. 24 Perhaps the early modulation of pro-inflammatory mediator release and, consequently, tissue degradation and pain control, may also have facilitated the proliferation of collagen type I. This modulation at the tissue healing process may have occurred because of rapid passage of the inflammatory phase to the proliferative phase, 25 as damage to tendons treated with LLLT was contained early.
Other factors that may have stimulated the increase of synthesis of collagen type I was the elevated mean power and ΔE used, which in turn sent electromagnetic signals (produced by the LLLT) to the extracellular matrix, increasing collagen type I and reducing type III, and improving the tensile strength of tendons. 11,18
There are studies corroborating these hypotheses, showing increases in the quantity of collagen type I in tendons submitted to the same method of injury as that used in this study, treated with elevated wavelengths and frequency of applications (one application per day for 5 consecutive days). However, and differently from this study, no difference was found in the quantity of collagen type III with the proposed treatment, 6 possibly because a low mean power was used.
On the other hand, some studies treated Achilles tendons with mean power that varied (40, 60, 80, and 100 mW) and showed elevated quantities of collagen type I when the mean power was 80 mW, and increased quantities of collagen type III when the mean power was 60, 80, and 100 mW. 18
This study presented increases of collagen type I, and, different from the previous studies, also showed a reduction of collagen type III with the LLLT parameters used. Therefore, the mean power, ΔE, and λ seem to be the most relevant factors in the stimulation of collagen proliferation, particularly type I, and the mean power of 70 mW perhaps is more appropriate than the mean power used in the aforementioned studies, to enhance repair of the Achilles tendon. 6,18
Although the present study demonstrates a satisfactory interaction between LLLT and the injured Achilles tendon, including stimulation of the repair process (tissue alignment and collagen proliferation), further studies of this interaction are required, using different injury methods and other parameters of LLLT.
Conclusions
LLLT stimulated the healing process of injured Achilles tendons, and is an adequate tool to enhance and optimize their repair.
Footnotes
Acknowledgments
The authors thank the São Paulo Research Foundation (FAPESP) for supporting this study (2011/00979-1).
Author Disclosure Statement
No competing financial interests exist.