
Abstract
Introduction
T
Resections are now made perpendicular to the long axis of the root, decreasing the number of exposed dentinal tubules and apical leakage. 3,4 Novel sonic and ultrasonic cutting tips have also improved treatment. Ultrasonic retrotips allow the cavity to be smaller, more central, and more precisely shaped. The risk of perforation is reduced, the long axis of the tooth is readily followed, and cavities made quickly and safely. However, some studies have shown the formation of cracks on the resected surface, 5,6 whereas others have not. 7,8 Specific laser wavelengths can also remove dental hard tissues. 9 –13 Hibst and Keller 9,10 report that with sufficient water cooling, cavities can be cut in enamel and dentin by an Er:YAG laser without causing thermal damage to the surrounding tissues, and studies have used this wavelength for apicoectomy. 11 –14
This study evaluated resected root surfaces for the presence of cracks after root-end cavity preparation using burs, zirconium nitride-coated ultrasonic retrotips, and an Er:YAG laser. The tested hypothesis was that there would be no significant difference between these very different surgical techniques.
Materials and Methods
Sixty extracted human maxillary anterior teeth that had been stored in distilled water were used. The teeth had been extracted following appropriate consent procedures, and were from hospital dental department collections. Crowns were removed at the cementoenamel junction. The root canals were prepared with ProTaper instruments (Dentsply/Maillefer, Ballaigues, Switzerland). Irrigation was copious, with 2.5% sodium hypochlorite solution and the use of an EDTA lubricant (MD-Chel Cream, META BIOMED, Chungbuk, Korea). The canals were dried with paper points and obturated by lateral condensation of gutta-percha (Diadent, ChoongchongBuk Do, Korea) with 2Seal canal sealer (VDW, Munich, Germany). The teeth were kept at 37°C and 100% humidity for 1 week to ensure set of materials.
Teeth were mounted in a jig. The apical 3 mm of 20 teeth were resected at an angle of 90 degrees to the long axis of the root with tungsten carbide fissure burs (HM 31L 010, Meisinger, Neuss, Germany), and their root-end cavities were cut with tungsten carbide round burs (HM 1 010, Meisinger) in a slow speed handpiece with water coolant (Group 1). The other 40 teeth were resected with an Er:YAG laser (Fidelis Plus III, Fotona, Ljublijana, Slovenia) set at wavelength 2.94 nm, 300 mJ, 25 Hz, with irrigation following the manufacturer's instructions. Root-end cavities for 20 teeth were made with the laser fitted with a 1 mm tip, wavelength 2.94 nm, 250 mJ, 15 Hz with irrigation (Group 2). Two laser tips were used to prepare this group. The 20 cavities for Group 3 were then cut with a zirconium nitride-coated ultrasonic retrotip (ProUltra Tip No. SURG 1, Dentsply/Maillefer, one tip for every 10 teeth) powered by an ultrasonic generator (EMS, Nyon, Switzerland) set to medium power with water cooling. All cavity preparation was by a single operator.
The cavities were checked with a periodontal probe (PCPUNC15, Hu-Friedy, Chicago, IL) to ensure a standard 3 mm cavity depth. Teeth were examined for the number and types of cracks on their resected surface before and after cavity preparation at×50 magnification with a stereomicroscope (Leica Imaging Systems Ltd, Cambridge, England). Methylene blue dye (2%) was applied for 2 min to the root surfaces to aid detection. The cracks were classified as complete, incomplete, and intradentinal, in a manner similar to that of Beling et al. 8 by two investigators who reached a consensus (Fig. 1).
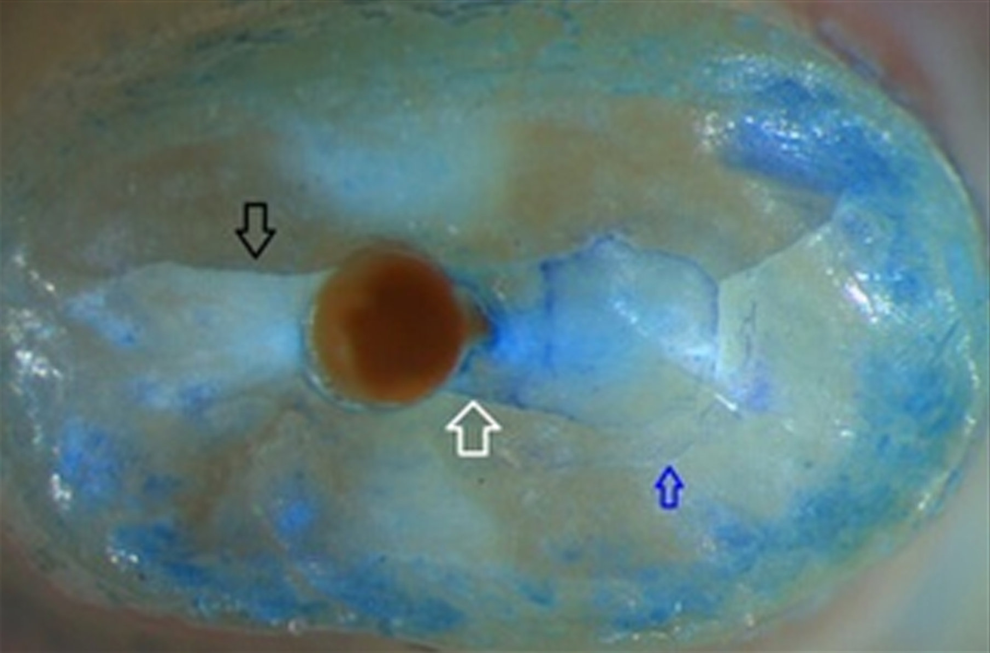
Explanation of crack types. Black arrow, complete crack; white arrow, incomplete crack; blue arrow, intradentinal crack.
Complete crack: extending from the canal space to the external root surface
Incomplete crack: extending from the canal space to a variable distance into the dentin, but ending short of the external root surface.
Intradentinal crack: confined to dentin and appearing to run in a facial-lingual direction mesial or distal to the canal.
Data were analyzed using the SPSS 11.5 program (SPSS Inc, Chicago, IL). Groups were compared using the Kruskal–Wallis and Mann–Whitney U tests. A p value≤0.05 was accepted as significant.
Results
The results are summarized in Tables 1 and 2. No statistically significant differences in crack number or type were detected between the more conventional and the laser groups after apical resections (p>0.05) or following cavity preparations (p>0.05).
Mann–Whitney U test was used in the analysis.
Kruskal–Wallis was used in the analysis.
Figures 2, 3, and 4 display representative images of the root ends after retropreparations for each groups.
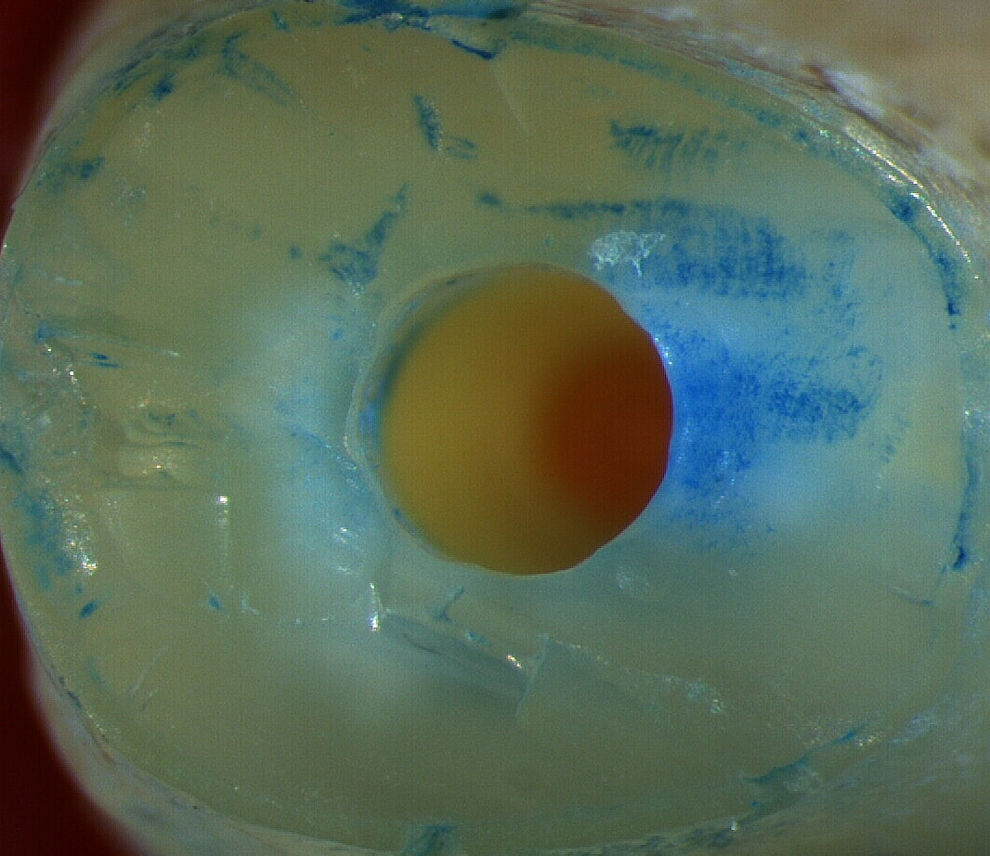
Root-end cavity after retropreparation with tungsten carbide round bur.
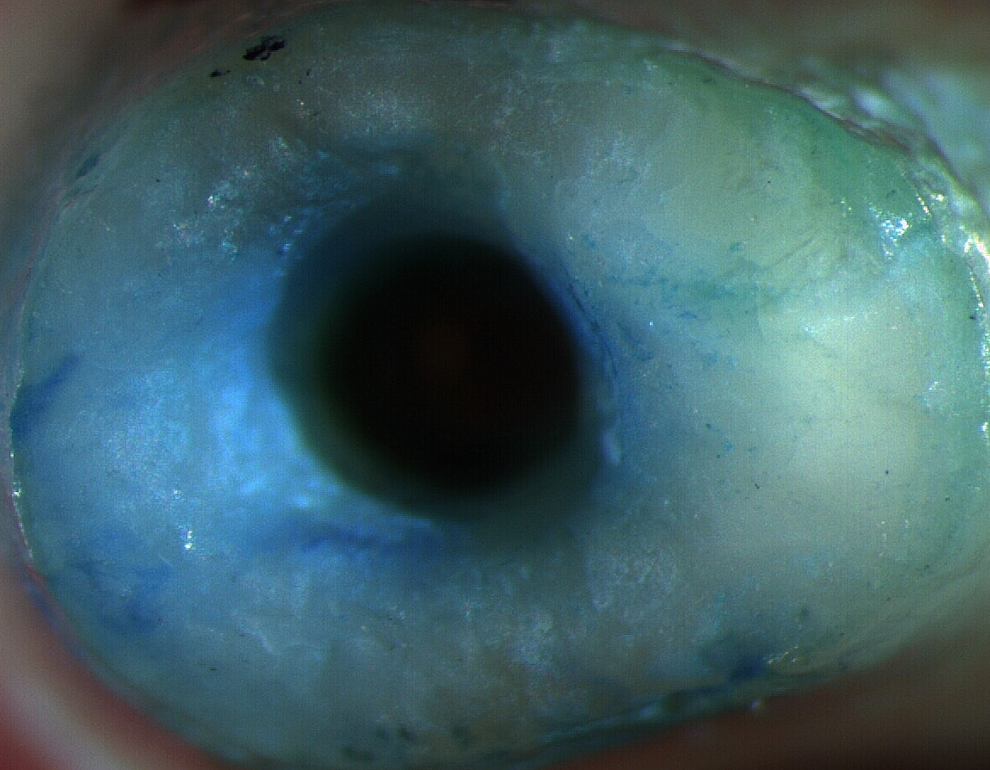
Root-end cavity after retropreparation with Er:YAG laser.
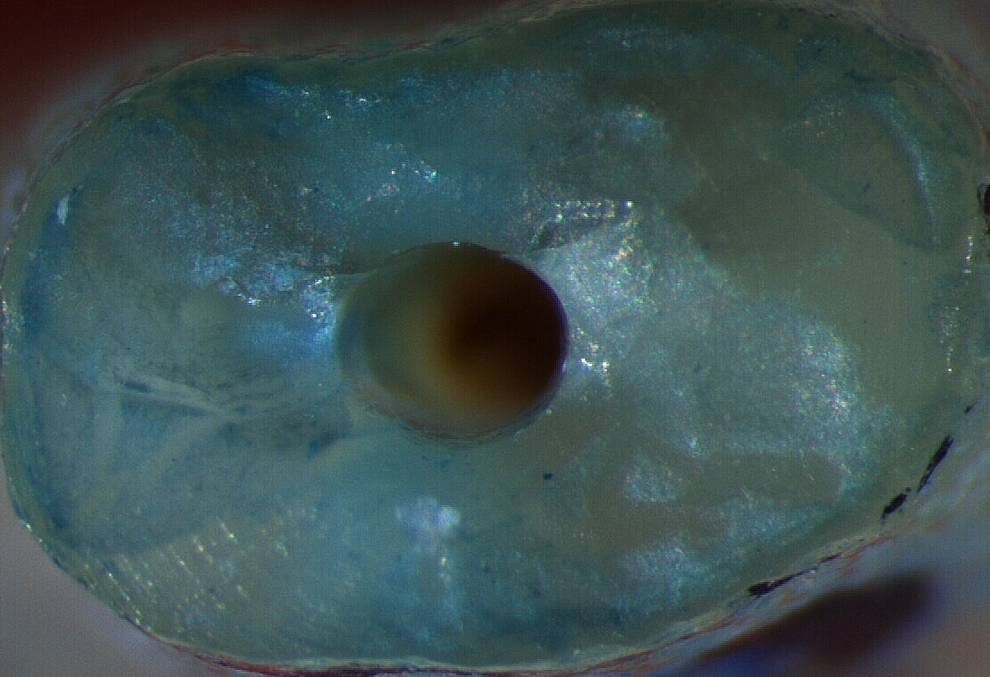
Root-end cavity after retropreparation with ultrasonic retrotip.
Discussion
The success rate of endodontic surgery has increased with the introduction of the dental operating microscope, ultrasonics, and improved root-end filling materials. 15 Results from this in vitro study agree with those of most studies about cracks formed by ultrasonic retrotips. 5 –7 Morgan and Marshall 16 found only 1 of 25 roots demonstrating evidence of a crack after ultrasonic preparation. Results from our study are comparable with those of Calzonetti et al. 17 and Gray et al., 18 who found no cracks in cadaver teeth after ultrasonic preparations. The current study has limitations, as it involved extracted teeth. In life, the periodontal ligament may act as an energy absorber during cavity preparation; 19 therefore, we supported the roots in a jig to simulate periodontium.
Navarre and Steiman 20 used zirconium nitride and stainless steel retrotips to examine crack formation in vitro, and discovered no cracks. Ishikawa et al. 21 found no statistically significant difference between zirconium nitride coated, diamond coated, and stainless steel ultrasonic tips for the number of microcracks in their in vitro study. For this reason, a zirconium nitride tip was used in this experiment.
Layton et al.. 6 and De Bruyne and De Moor 22 reported more crack formation at high frequency settings in in vitro models; however, Waplington et al. 7 found that power levels did not influence the number of cracks. Taschieri et al. 23 used full- and half-power levels in another in vitro study, and a significant difference was found; there were more cracks at full power. Bernardes et al. 24 did not detect any crack formation at medium power in their in vitro study. This suggests that ultrasonic generators should be set at medium power for root-end cavity preparation.
Many researchers have used teeth with filled root canals to represent in vivo conditions, 21,23,25 –28 but others have used unprepared teeth. 11,16,29,30 Beling et al. 8 reported that there was no significant difference between teeth filled with gutta-percha and unprepared teeth, but Onnink et al. 31 found a significant difference.
Hibst and Keller 9,10 reported that under sufficient water cooling, cavities could be made in enamel and dentin with an Er:YAG laser without causing thermal damage to the surrounding tissues. Scanning electron microscopic (SEM) studies by these authors showed that laser-resected surfaces presented an irregular but clean surface, with no smear layer and exposed dentinal tubules.
Wallace 32 evaluated the tendency for crack formation using the ErCr:YSGG laser for preparation of root-end cavities in vitro. Stereomicroscope views were taken from 36 extracted teeth after cavity preparation, and only one canal-related crack was found in unprepared teeth. Rahimi et al. 33 compared the number of cracks after ErCr:YSGG laser and ultrasonic root-end preparations of obturated teeth, recording only one crack in the ultrasonic group, and none in the laser group. The present study showed no significant difference between the laser and ultrasonic groups for number and type of cracks. Komori et al. 13 used the Er:YAG laser for the apicoectomy of 13 teeth for eight patients. Advantages such as absence of pain and vibration, the low risk of trauma to the surrounding tissues, and lack of risk of contamination of the surgical field were noted, with a 7 month clinical and radiological follow-up finding treatment successful. The current experiment used a similar laser in vitro, but for routine clinical use, the size of its handpiece and the angulation and diameter of its fiber tip need modification. Few studies have investigated the effect of piezosurgery on the integrity of root apices after cavity preparation. 34 Ultrasonic instruments are currently the preferred choice for root-end cavity preparation. 35 Laser resection and cavity preparation in this experiment appeared to be no more damaging than established techniques, and they offered the added benefit of disinfection of the root face and the root-end cavity. 36 Developments in laser tips made for surgery of this type will facilitate further research.
Conclusions
Under the conditions of this in vitro apicoectomy study, it appeared that the resection and root-end preparation method chosen had no significant effect on crack numbers or type.
Footnotes
Author Disclosure Statement
No competing financial interests exist.