
Abstract
Introduction
D
Today, various materials are available for treating DH, such as tubule sealants, resin bonding agents, cements, desensitizing dentifrices, and lasers. 3,4 Among these methods, a desensitizing dentifrice is the easiest and the most common approach. 5 –7 Its ingredients have to attach and penetrate into the dentinal tubules and maintain the occluding effect for a long time. 8 A dentifrice containing 20% nano-carbonate apatite (n-CAP) was proved to form a thick protective layer on the dentinal surface. 9 This result was confirmed in other studies as well. 10,11 Carbonate apatite is similar to the inorganic component of the teeth, and it has excellent biocompatibility. 12 Furthermore, as the size of the particles is extremely small, this leads to attachment onto the tooth surface. 11
To treat DH successfully, the treatment ingredients must be resistant to the acid and mechanical challenges. 13 However, the primary mechanism of desensitizing agents is mechanical bonding rather than fusion. 14 –16 When the agents are exposed to acidic foods or tooth brushing, they are removed from the dentinal surface. Although the agents can relieve tooth sensitivity, the effect may not be long lasting. 3 Hence, the agents should be applied repeatedly. 13,16
Nd:YAG, Er:YAG, and CO2 lasers have been used for treatment of DH. 3,17 Laser treatment has low acid solubility and a long-term effect. 18,19 Among dental lasers, CO2 laser is known for not causing thermal damage, because of the high water absorption. 17,20 This laser is also characterized by its high hydroxyapatite absorption (low penetrating depth) and mechanical/acid resistance. 3,21 Therefore, it can apply in a noninvasive and long-lasting combined therapy with the n-CAP.
The combination of two different existing methods has been tried by many researchers. 14 –16, 22 –26 The combination of Nd:YAG and Gluma desensitizer had immediate and long-lasting effect in an in vivo study. 27 The combination of CO2 laser with fluoride gel was also more effective than laser alone in dentinal tubule occlusion. 14,25
Based on these findings, a new approach of combination of n-CAP dentifrice and laser was tried. The optimal irradiation conditions of combination therapy for achieving occlusion of dentinal tubules and development of acid resistance were determined based on the in vitro studies. 10,11 This study was then performed to identify whether the combination effect can be reproduced in an in situ model. The aim of this study was to evaluate the occluding effect and acid resistance of the combination of n-CAP dentifrice and CO2 laser by using an in situ model.
The null hypothesis was that the occluding effect and acid resistance effect of the combination treatment would be the same as that of the n-CAP dentifrice only.
Materials and Methods
Study design
The present study was a two-period crossover, single blind, randomized, four-treatment, split-mouth study. Ten healthy participants wore individual intraoral lower buccal appliances from 9:00 a.m. to 3:00 p.m. The oral appliances that were developed by Claydon et al. were modified for this study (Fig. 1). 28 It was designed for utilizing brushing times similar to an in vivo situation, and performing tooth brushing ex vivo. In a previous study, wires were used to fix specimens for analyzing. As this study was evaluated once during a period with a scanning electron microscope (SEM, S-4700 Hitachi Ltd., Tokyo, Japan), specimen replacement was not necessary. Putty instead of wires could also reduce the subject's discomfort. Four specimens were fitted in each appliance during the first period, and then the specimens were replaced in the appliance for the next period. The appliances were stored at 100% relative humidity after rinsing.
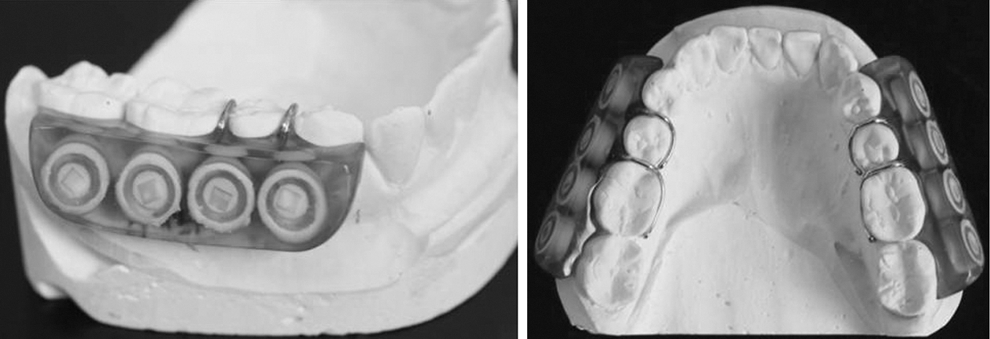
Intraoral appliance used in this study.
This study was performed for 8 days with 4 treatment days in each of the two periods of the study, and there was a 3-day washout period between the two periods. 29 Each period was divided into two parts for evaluation by using SEM; dentinal tubule occlusion on 2 days (days 1 and 2) and acid challenge on 2 days (days 3 and 4). At each evaluation, 20 specimens in a group were included in the SEM analysis.
The study was approved by the Ethics Committee of Yonsei Dental Hospital (Seoul, South Korea) (IRB No.2-2012-0044). The sample size was calculated according to the method used in previous study. 11 Between the n-CAP and the combined group, it was assumed that there would be a difference of 18 μm2 and a standard deviation of 20 for this difference using a one sided 5% significance test. Allowing for a dropout rate of 20% and 80% power, 9.54 subjects were needed. Therefore, 10 subjects were recruited.
All of the subjects were informed about this study, and informed consent was obtained. They were provided with an electric toothbrush (Oral-B professional, Braun, Germany) and n-CAP dentifrice to be used twice a day. They were instructed to brush the specimens by applying the same pressure (200g). The subjects were not allowed to consume any food and drink while wearing the appliances. The subjects brushed their teeth in their usual manner.
To collect teeth, a dental hygienist informed the patients who visited Yonsei Dental Hospital for tooth extraction about this study. Only teeth from patients who gave consent for the use of their extracted teeth were used.
Experimental group and acid challenge
There were four experimental groups: control, n-CAP, laser, and combined (Table 1). During the first period, participants wore the appliance, which fitted the specimens in the control group on the left side and those in the n-CAP group on the right side. During the second period, they wore the appliance, which fitted the specimens in the laser group on the left side and those in the combined group on the right side. Two specimens in each appliance were used for evaluating occlusion effect, and the other two specimens in the same appliance were used for evaluating acid resistance by SEM.
Twenty specimens from each group were used for evaluation of dentinal tubule occlusion by each treatment, and the other 20 specimens were used for the acid challenge.
n-CAP, nano-carbonate apatite.
The control group was not treated, and the n-CAP group was treated with the n-CAP dentifrice (Dentiguard sensitive®, Daewoong, Korea) for 17 sec on each occasion (two times a day) using an electric toothbrush ex vivo. The brushing time was determined from a previous study, in which the toothbrush made contact with the tooth for a maximum of 10 sec per day. 30 Based on this result, the time was calculated to assess the effect that would have been achieved had the patient used the dentifrice for 2 weeks. The laser group was irradiated with CO2 laser (Panalas CO5∑, Panasonic, Japan) using a 1A tip for 1 min with a power output of 3W (with low air cooling). The distance from the surface was 2–3 mm, and the energy density was 0.96 J/cm2. The laser beam was controlled in a zigzag manner with the beam directed vertically to the dentin surface. The combined group was first treated with n-CAP dentifrice and then irradiated twice on days 2 and 4. 25
On day 2, 20 specimens from each group were removed from the appliance to evaluate the dentinal tubule occlusion. The remaining 20 specimens were subjected to acid challenge by simple immersion in grape juice with pH 3.67 (Minute Made®, Coca-cola Co., Korea) for 3 min (ex vivo), and then rinsed. The acid challenge was performed on days 3 and 4 during the period, two times a day (11 a.m. and 3 p.m.). After acid challenge, the specimens were evaluated using SEM.
Specimen preparation
Recently extracted intact third molars, from patients >18 years of age, and of both genders, were used for obtaining the dentin samples. The teeth were stored in a freezer at −20°C until their use. The samples were cut up to the cemento–enamel junction using a diamond wheel disc. Root samples were embedded in a Teflon mold using an acrylic resin, and then ground with P600 to 1200 of silicon carbide papers (Allied high tech products, Rancho Dominguez, CA) using a polishing machine (RB 209 Minipol, R&B Inc, Korea) to expose the dentin surface. The dentin specimens of 2×2 mm2 in size were obtained from the same root to decrease the variation. After autoclaving, a total of 160 dentin specimens were embedded into an acrylic mold. They were fixed in the intraoral appliance with putty. Each specimen fixed in the appliance was etched with 6% citric acid for 90 sec to open dentinal tubules. After rinsing, all of the specimens were dried at room temperature.
Evaluation of dentin specimens
Twenty specimens of each group were evaluated at each step; after dentinal tubule occlusion and acid challenge using SEM. The method for analysis was the same as in our previous study. 11
Statistical analysis
One-way ANOVA and Tukey's post-hoc test (PASW statistics ver. 18.0, SPSS, Chicago, IL) were used. The paired t test was used to evaluate the occluding effect of the treatment before and after the acid challenge. A p value of<0.05 was considered statistically significant.
Results
The mean age of the subjects was 29.2±4.6 years (3 males and 7 females).
In all of the experimental groups, the area of open dentinal tubules was decreased significantly after treatment compared with that in the control group (p<0.0001, Table 2). However, the occluding effect in the experimental groups did not show statistically significant differences (p>0.05). The occluding effect in the combined group was 97%, which was the highest occluding effect; that in the laser and the n-CAP group were 89% and 77%, respectively (Table 2). A smooth surface and wide dentinal tubules were observed in the control group (Fig. 2A). The n-CAP group had tubules almost completely occluded by the n-CAP particles (Fig. 2B). This n-CAP layer was also observed in cross-sectional micrographs (Fig. 2b). The laser group had a melted surface and a thin layer (Fig. 2C and 2c). In the combined group, dentinal tubules were completely occluded by melted n-CAP particles (Fig. 2D). Also, re-crystallized n-CAP particles were found to have penetrated into tubules, and they were found to occlude the entrance of the dentinal tubules in cross-sectional micrographs (Fig. 2d).
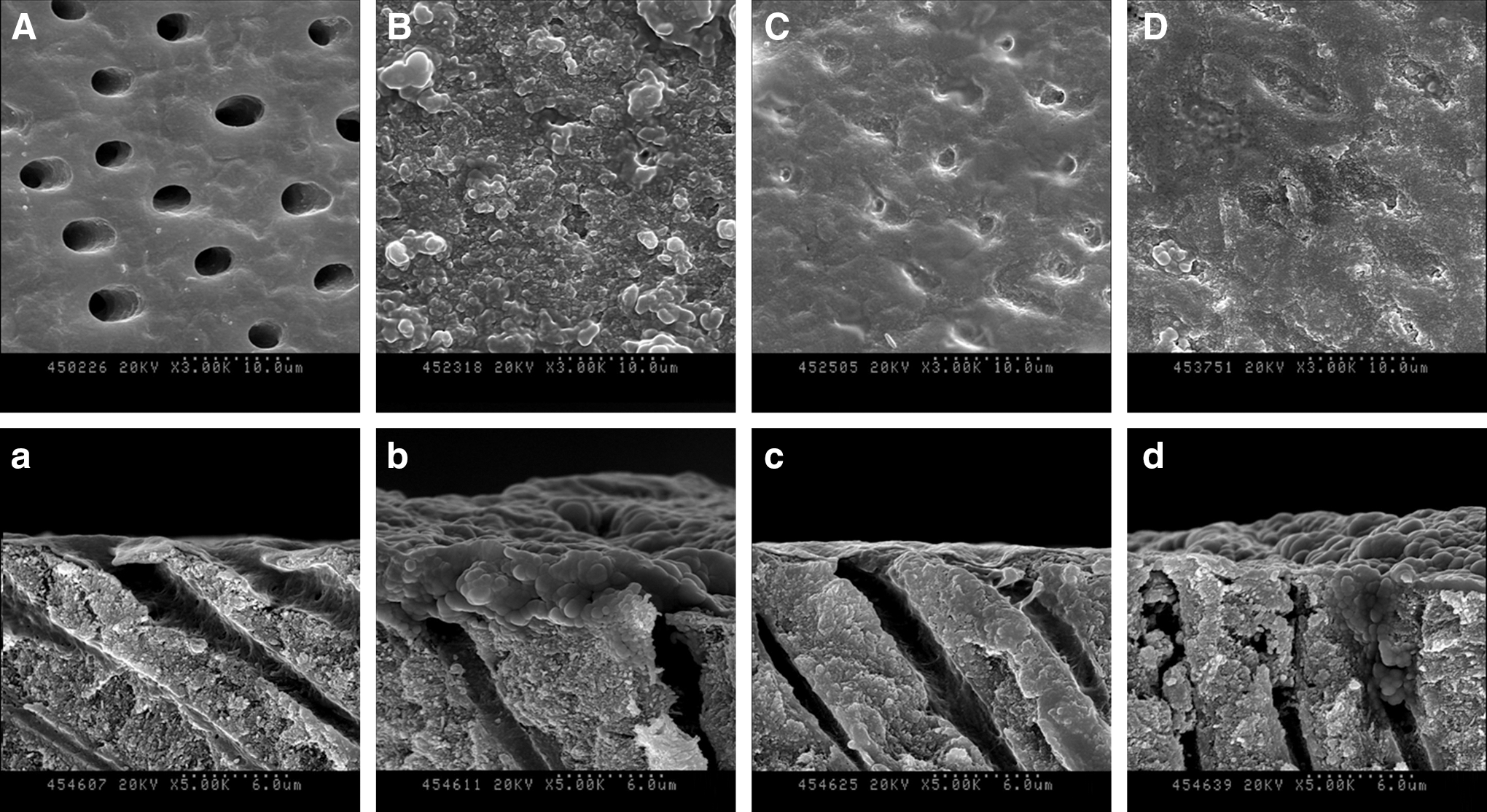
Scanning electron micrography (SEM) micrograph of specimen surfaces (
All values denote the mean (standard deviation).
Unit: μm2
In the same column, different superscript letters denote significant differences between groups by Tukey post-hoc test (α=0.05).
p values were determined by paired t test (α=0.05).
n-CAP, nano-carbonate apatite.
After 2 days of toothbrushing twice daily in the acidic environment caused by grape juice, the area of open dentinal tubules was significantly increased in the experimental groups (p<0.0001, the n-CAP and the laser group; p=0.020, the combined group, Table 2). The combined group showed the highest acid resistance among all of the experimental groups. The increase in the area of open dentinal tubules was only 1.51 μm2. On the other hand, in the n-CAP and the laser groups, the increase in open dentinal tubule area was 15.49 and 27.68 μm2, respectively (Table 2). In the n-CAP group, some n-CAP particles were found to occlude the dentinal tubules, but most of the dentinal tubules had re-opened (Fig. 3B). In cross-sectional image, the thick n-CAP layer was damaged by acid (Fig. 3b). Also, the lased dentin surface was exposed (Fig. 3C). In the combined group, however, fewer open tubules were observed than in other groups, and the dentinal tubules were occluded because of the remaining n-CAP on inner tubule walls (Fig. 3D and 3d).
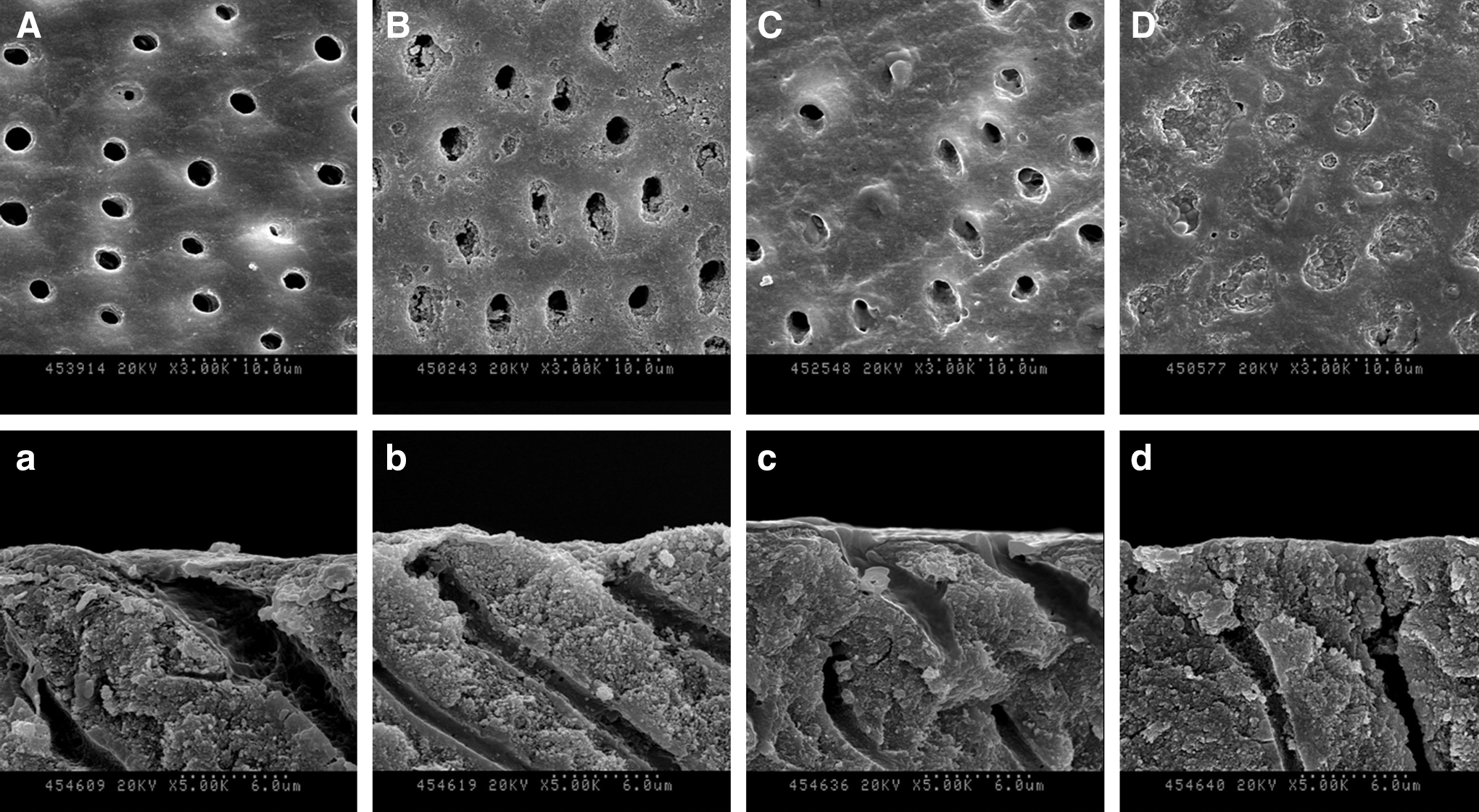
SEM micrographs of specimen surfaces (
Discussion
The null hypothesis was rejected pertaining to the acid resistance only. Although there was no significant difference in occluding effect of dentinal tubules between the n-CAP and the combined group, reopened dentinal tubule area in the combined group was significantly less than that in the n-CAP group after acid challenge.
This study assessed the occluding effect and acid resistance of the combined therapy by using an in situ model. In this study, the combined group showed higher dentinal tubule occlusion than did the control group. However, there was no significant difference in dentinal tubule occlusion among the treatment groups (p>0.05, Table 2). After acid challenge, the combined group showed a significantly lower reopened dentinal tubule area (1.51 μm2) than that in all of the other experimental groups (Table 2).
There are some reports suggesting that dentifrice abrasives have variable affinity for dentin surface, and that they cause unstable properties by mechanical stimulation and if acidic beverages are consumed. 31 –34 In this study, repetitive tooth brushing was performed to simulate an actual clinical situation. As a result, multiple n-CAP layers were found on the dentin surface (Fig. 2). However, the n-CAP layers were partially removed, and the dentinal tubules had reopened after acid challenge (p<0.0001, Fig. 3). Nevertheless, the n-CAP particles still remained on the intertubular dentin. It has been shown that the n-CAP particles can chemically attach to the tooth surface. 35 In a previous study, which evaluated the erosion and abrasion caused by a dentifrice, the dentifrice containing zinc-carbonate-hydroxyapatite exhibited the greatest abrasive property because of its soluble nature. 36 The other study reported that the use of a desensitizing dentifrice reduced the permeability of dentin. 37 Attenuated total reflection – Fourier transform infrared spectroscopy (ATR-FTIR) analysis also showed an increase in the intensity of the phosphate peak after using the desensitizing dentifrice. However, the dentin permeability was significantly increased and the intensity of the phosphate peak was decreased after acid challenge. These results were only caused by mechanical occlusion by the precipitation of insoluble calcium fluoride crystals within dentinal tubules. 11 Therefore, mechanical occlusion without fusion may have limitations in maintaining the occluding effect, because the ingredients can be removed by challenges in the oral cavity over time.
The desensitization effect of laser is decided by the type of laser, irradiation parameters, and evaluation method. CO2 laser and its parameters were chosen for use in combination with the n-CAP dentifrice based on the results of two previous studies. 10,11 The CO2 laser group did not show a molten-like appearance and orifices, which could have caused confusion in image analysis of the Er:YAG laser. 10 The CO2 laser has a lower penetration depth than the Nd:YAG laser, and hence it reduces the thermal damage. 3,38 The beam is absorbed by hydroxyapatite, and it also melted the tooth surface. The CO2 laser, therefore, showed the greatest occlusion effect in this study (p<0.0001, Table 2).
The laser group could not resist against the acid challenge. The area of opened dentinal tubules was greater in this group than that in the n-CAP group. This result was in accordance with our previous study. 11 Even though acid resistance is an important feature in the treatment of DH, as it prevents exposure of dentinal tubules, the use of a single laser does not resist an agitated acid challenge. It is known that the effects of lasers on the treatment of DH vary, depending upon the type of laser used and the irradiation parameters, and the superiority of lasers to topical desensitizing agents is marginal. 39,40 The recurrence rate of DH was found to vary with each laser; the recurrent rate of hypersensitivity of the He-Ne laser was from 7.4% to 66.0%, that of the GaAlAs laser was from 6.0% to 75.0%, that of the Nd:YAG laser was 34.0%, and that of the CO2 laser was up to 50.0%. 41 In this study, the effectiveness of laser irradiation only was lower than that of the n-CAP and the combined treatments.
The combined treatment with the n-CAP and laser has been conducted to enhance the treatment effect in vitro. 10,11 The previous study showed that the highest dentinal tubule occlusion and acid resistance were observed in the combined group. 11 The present study also proved that the combined group had the highest occlusion effect (97%) compared with the control group, and the least increase in the reopened tubule area after acid challenge in the in situ model. The formation of a thick layer caused by laser irradiation and repetitive tooth brushing during the treatment was also observed (Fig. 2D). Repetitive tooth brushing can help to increase the coherence between the n-CAP layers before and after laser irradiation. Consequently, a thick protective layer was formed on the dentin surface. The other advantage of this combined treatment was an increase in the acid resistance, by eliminating carbonate. 23 Therefore, the combined group showed the smallest increase in the area of open dentinal tubules after acid challenge.
As this was an in situ study, it could have some limitations.
First, it may not be possible to extrapolate the results of an in situ study to an actual clinical situation. However, in vivo studies cannot show the changes caused by treatment of open dentinal tubules, 42 and they could be time consuming. For this reason, many researchers have used an in situ model to study the dental phenomena or conditions. 42 According to in situ study, the experimentation period could be reduced, and control of the confounding factors could be achieved.
Second, we used a different solution from the previous study, which used acetic buffer solution to test acid resistance of the combined treatment. The reason for this was that although the intraoral appliance was immersed ex vivo, the subjects had to wear the appliance after rinsing; therefore, we changed the solution based on the other studies. 29,43 Although the type of solution used might have an influence on the results, this study showed similar results to those in an in vitro study.
Conclusions
This in situ study has shown that the combination of n-CAP desensitizing dentifrice with CO2 laser results in the same effectiveness in the dentinal occlusion effect as with the n-CAP only. This new approach, however, showed an acid-resistant property compared with the other approaches. These findings indicate that this combined therapy is a promising method for ensuring long-lasting effect of DH treatment in clinical practice.
Footnotes
Acknowledgments
This study was approved by the institutional review board committee of the College of Dentistry, Yonsei University. This work was supported by the Basic Science Research Program through the National Research Foundation of Korea (NRF), funded by the Ministry of Education, Science and Technology (R13-2003-013-05002-0).
Author Disclosure Statement
No competing financial interests exist.