
Abstract
Introduction
I
Several studies have reported some negative effects of tooth bleaching. 2,5 –7 However, the most common side effect in teeth with pulp vitality is tooth sensitivity. 3,8 –10 A definitive understanding of the tooth hypersensitivity issue has been far more elusive, and, as such, remains the most common adverse event associated with whitening of vital teeth. 11 This sensitivity can be caused by the formation of oxygen bubbles inside the dentinal tubules from the application of hydrogen peroxide (HP), and activation of the intrapulpal nerves. 12 To minimize this sensitivity, various methods have been proposed, such as laser therapy as an immediate auxiliary analgesic aid by the repolarization of the altered nerve membrane. 5,9,11 –14
Auxiliary power sources (halogen light, arc plasma, LED, LED-laser, and laser) are used in in-office tooth bleaching techniques to accelerate the redox reaction of the whitening gel, to increase ease of use, to improve comfort and safety, and to decrease the procedure time. 2,13,15 –19
Hybrid equipment with LED and low-level laser has emerged as a suggested method to improve the efficacy of bleaching and to help control tooth sensitivity. However, there are few clinical studies in the literature evaluating the efficacy of hybrid LED-laser in tooth bleaching. 1,5,6,20
Therefore, the aim of this study was to evaluate the efficacy of low intensity laser radiation present in a hybrid LED-laser source in the activation of 35% HP gel, and the control of dental sensitivity using the in-office bleaching technique.
Materials and Methods
Study design
The study was blind, randomized, and split mouth (upper and lower arches). The Ethics Committee of the Universidade Estadual de Ponta Grossa approved this research (protocol number 187442010).
Inclusion and exclusion criteria
The following were included: patients between 18 and 30 years of age, with good oral and general health, vital upper and lower teeth (first premolars, canines, and incisors) that are free of caries and restorations, good oral hygiene, who are nonsmokers and do not have painful symptoms. The initial color of these teeth was C2 or darker compared to the VITA Lumin scale (Vita Zahnfabrik, Bad Säckingen, Germany) and organized by order of value. 7,8,21
The following were excluded: patients who had undergone any type of prior bleaching procedure, pregnant or lactating women, patients with teeth showing staining (tetracycline or fluorosis), those who had had endodontic treatment, and those with parafunctional habits or who are using analgesic and/or anti-inflammatory drugs.
Sample size calculation
The sample size calculation was performed based on data from previously published studies. 1,5 Considering a test power of 80% for an average percentage of the population of 87% of the individuals who reported tooth sensitivity within 24 h of bleaching, we established a suggested proportion of 62% tooth sensitivity with the use of different light sources. These calculations were made using a statistical program (nQuery Advisor version 4.0 for Windows, Statistical Solutions; Saugus, MA, USA). 1,5 Therefore, the sample size required to detect differences was 15 volunteers per group. A total of 16 individuals per group were selected in order to offset any withdrawal of volunteers.
Study intervention
The hybrid source device (Whitening Lase II, DMC Equipamentos LTDA, São Carlos, SP, Brazil) used in this present study had six blue LED (425–480 nm) outputs with 300 mW of power each, and three infrared lasers (810 nm) with 200 mW of power each and 8 cm2 spot size. The irradiance LED-laser system was ∼300 mW/cm2 per tooth.
Upper and lower arches randomized in the LED and LED-laser groups, therefore resulting in n=16 for each group. The participant was blind to the treatments and the operator did not know which group that participant would be allocated to at the time of intervention. The groups received the following treatments.
GL (LED) was treated with 35% HP (Lase Peroxide Sensy 35%, DMC, São Carlos, SP, Brazil), and activated only by LED light.
GLL (LED-laser) was treated with 35% HP (Lase Peroxide Sensy 35%), and activated by LED-laser.
In both groups the light was activated three times; 1 min of activation, interspersed for 2 min with gel at rest; after the third application the gel was allowed to remain for 3 min and was then removed, totaling 10 min, 3 min of which included irradiation. The gel was then replaced, and the protocol was repeated twice more, totaling 30 min, same as above, 9 were irradiation. The bleaching treatments were performed during two sessions at intervals of 1 week between sessions and 2 weeks between treatments.
The teeth and soft tissues were air dried; the gums were protected with a gingival barrier (Lase Protect, DMC) and light cured for 30 sec with Whitening Lase II. Participants were instructed to brush their teeth regularly using fluoride toothpaste (Sorriso Fresh, Colgate-Palmolive, São Paulo, SP, Brazil).
Tooth sensitivity evaluation
Participants were instructed to register their tooth sensitivity at various times: during bleaching, immediately after finishing the bleaching, 12 h after, 12–24 h after, 24–48 h after, 1 month after, and 6 months after the completion of the procedures, using a five point verbal pain rating scale (VRS): 0=none, 1=mild, 2=moderate, 3=considerable, and 4=severe. 5 –7 The data were organized into two categories: the overall percentage of patients who reported tooth sensitivity at least once during treatment, regardless of the evaluation time, and the intensity of the overall sensitivity at each of the evaluation times.
Shade evaluation
The color evaluation was subjective and was recorded before and after each bleaching session, 1 month after, and 6 months after the bleaching treatment using the Vita Lumin color scale. Consequently, in each period, the change in color of the teeth in relation to their initial color was determined; color guides were organized from the highest value (B1) to the lowest value (C4), as shown in Table 1. 3,7 The measurement area of interest for the registration of color was the middle third of the labial surface of the central incisors. For calibration purposes, six patients who were not included in the sample participated in the training phase. Two examiners, who were blinded to the allocation of the session, evaluated the color of teeth at baseline (before the treatment), after cleaning of the teeth, before and after each treatment session, and at 1 and 6 months after the procedure, always in the same room with artificial lighting and the patient in the same position. 3,10
Light-to-dark ranking by manufacturer.
Statistical analysis
The agreement between the researchers was assessed using the weighted Kappa test. Tooth sensitivity and efficacy of bleaching were compared between groups at each period, using the Wilcoxon test. The parameters within the same group at different evaluation periods were analyzed using the Friedman test with the pairwise comparison made with the Wilcoxon test. The proportion of individuals who reported sensitivity after treatment were analyzed using the Cochran Q and McNemar tests. The level of significance was 5%.
Results
All the volunteers completed the study. The agreement (Kappa) between the examiners for the color variable was κ=0.889, which was considered to be excellent. Table 2 shows the number of patients who experienced sensitivity during treatment, regardless of the sessions. Over half of the patients experienced sensitivity during bleaching. Most volunteers from both groups experienced sensitivity within 24 h, but at the end of 48 h the percentage of individuals with sensitivity decreased significantly in both groups (p<0.05). The sensitivity was not significant at any assessed period when a comparison was made between the groups (p>0.05).
Regimen: two sessions at intervals of 1 week between sessions and 2 weeks between treatments.
Rows: similar uppercase letters, no statistically significant differences (p>0.05). McNemar test.
Columns: different lowercase letters, significant differences (p<0.05). Cochran's Q test and pair comparisons with McNemar test.
Figure 1 shows the sensitivity scores in percentages for the groups at the studied periods. Severe sensitivity was reported more often in the 12 h after bleaching. After 48 h, there was a reduction of the sensitivity scores with no pain (97%) or mild pain (3%) in both groups. Table 3 shows that there was no statistical difference between the groups at any time period (p>0.05). However, differences were observed when comparing different periods within the same group (p<0.05).
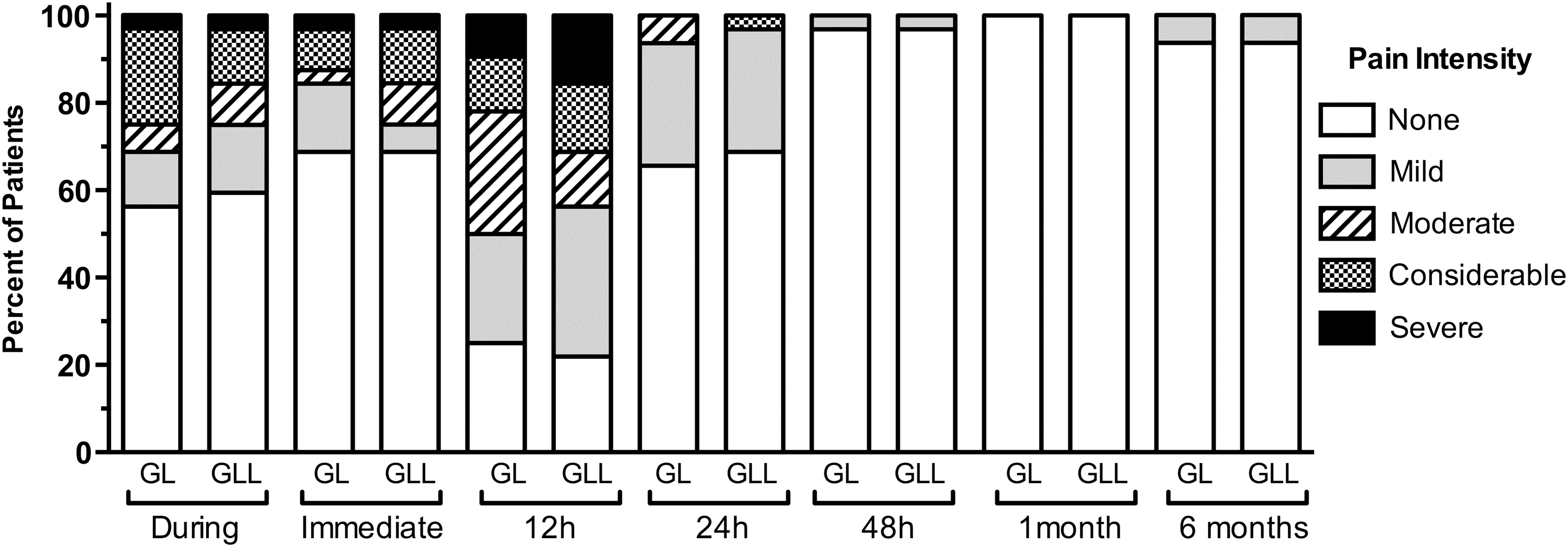
Percentage of subjects in GL (LED) and GLL (LED-laser) groups who reported no, mild, moderate, considerable, and severe pain at each time period.
Rows: similar uppercase letters, no statistically significant differences (p>0.05). Wilcoxon test.
Columns: different lowercase letters, significant differences (p<0.01). Friedman test and pair comparisons with Wilcoxon.
VRS, verbal pain rating scale.
Regarding color change (Table 4), there was no difference between the groups at any evaluated period (p>0.05). Nevertheless, the two techniques were effective for bleaching, with the difference between the initial time and 30 days after bleaching being statistically significant for both groups (p<0.01).
Rows: similar uppercase letters, no statistically significant differences (p>0.05), Wilcoxon test.
Columns: different lowercase letters, significant differences (p<0.01), Friedman test and pair comparisons with Wilcoxon.
Discussion
In this present study, when we evaluated the prevalence of tooth sensitivity, we observed that 94% of patients in each group reported pain within 12 h after receiving treatment. During treatment, the GL group (LED) had 63%, and the GLL group (LED-laser) had sensitivity at 56% of the evaluations. Different methods to reduce the sensitivity associated with bleaching have been used, including the reduction of concentration, time, and frequency of use of the gel, as well as treatment with fluoride, potassium nitrate, and lasers. 2,4,9,11,12,20
Few studies have evaluated hybrid light source systems with blue LED and low-intensity infrared laser in tooth bleaching, with the aim of verifying whether the combination of these elements could provide some advantages regarding the reduction of tooth sensitivity and color change compared with conventional treatments (LED). 1,5,6 Only one study in the literature has shown reduced tooth sensitivity when hybrid LED-laser sources and 35% HP were used, compared with the use of isolated 35% HP. 20 However, in this study, the authors used a shorter exposure time in the LED-laser group than in the isolated HP group, that is, the group with hybrid sources the contact time of the gel was 47% lower. This was probably the cause of reduced sensitivity to the LED-laser, as studies confirm that the longer contact time of the gel with the teeth is one of the causes of increased sensitivity caused by bleaching. 4,6
Studies show that phototherapy with low-intensity laser can offset the effects of cytotoxic substances released by HP, and assist in the decomposition and catalyzing of the same, accelerating its bleaching action. 2,14 The wavelengths of red and infrared light are absorbed into cells, increasing metabolism under stress conditions, and thus the photon energy is absorbed and converted by chemical reaction inside the cells. 14 Consequently, when properly used, low-power laser can reduce pulpal damage and promote post-bleaching pain relief. 14,16
In our study, we observed that the higher scores for tooth sensitivity were reported more frequently up to 12 h after bleaching for both groups, and that from 24 h on, there was a significant decrease in both groups, with no pain (97%) or mild pain (3%) being reported after 48 h. These findings differ from some studies, in which increased sensitivity was reported for >48 h when LED-laser sources associated with 35% HP were used, 7 but are in agreement with results from other studies, and confirm that tooth sensitivity caused by bleaching seems to be transient. 1,2,6,8
A possible reason why we did not find different results between the groups is probably because the therapeutic laser that is present in these hybrid sources does not come into direct contact with the target tissue. 13 One should also consider the barrier formed by the colored HP gel can minimize the density of the power in the target tissue and maximize light reflection, 6,16,17,19,22 significantly decreasing the absorption of laser by the tissue (dental pulp), which means that the therapeutic action of the laser is reduced. 13 The fact that the hybrid LED-laser source has three laser outputs, and that laser light is not collimated, means that the light may, therefore, not reach the target properly.
A point observed in the present study was the difficulty in evaluating the parameter of tooth sensitivity, given its subjectivity. To investigate the sensitivity caused by bleaching, we used the five point VRS, because apart from its simplicity, it provides good reproducibility in the study of tooth sensitivity, and has been applied to other studies that have analyzed sensitivity after tooth bleaching. 5 –7
The present study used a cross-over, split-mouth (upper and lower arches) clinical approach, which differed from other studies that used a maxillary hemi-arch split-mouth design. 3,8,10 The reason for this choice was the format of the delivery system of the tip of the LED-laser, which has a tip with six LED outlets and three infrared laser outlets arranged in one dental arch (superior or inferior), therefore making it impossible to assess in the same dental arch. It is generally believed there is a greater tendency for sensitivity to occur in teeth in the lower arch because of the lower thickness of dentin, and, consequently, faster and more intense penetration by the bleaching gel. 3,10 This was not demonstrated in the present study, which is in agreement with other studies in which there was no correlation between the thickness of the tooth and post-bleaching sensitivity, or between the upper and lower teeth. 4,6 It is worth mentioning that all the teeth of the volunteers included in this study responded positively to a pulp sensitivity test after 30 days and after a 6 month follow-up study.
Regarding the efficacy of tooth bleaching, this study evaluated the color change using a shade scale at different periods. 2,3,7,8 We observed a significant color change from baseline to 30 days and 6 months. This result was maintained for the periods of 30 days and 6 months for both groups. 5,6,8,21 The studies that used 35% HP bleaching (with or without light) reported changes in color of 5–8 shade guide units (SGUs) after the second bleaching treatments, 5,7,8 which is consistent with the results of this present study. The manufacturer of the LED-laser equipment suggests that the laser also has the function of activating the gel to improve the efficacy of bleaching, in addition to the function of desensitization. Our study demonstrated that the laser present in the hybrid sources was not more effective than the LED used alone, similar to the results of other studies. 1,5,6 This may have occurred because of the use of high concentrations of HP, as previous studies have shown that in these situations the use of light sources may be considered optional, because the number of free radicals produced by the chemical degradation of HP are sufficient to react with the pigments of the structure of the dentin, and any further increase in this number will not speed up the bleaching process. 8,9
It is important to state that the type of LED-laser models available, with different delivery systems and power light sources, coupled with the diversity of catalyzing agents, makes it difficult to make a comparison with other studies. 15,16,18,20,22 Nevertheless, it is important to emphasize the need for further research into the use of hybrid light sources in tooth bleaching. Therefore, further studies of the use of bleaching agents in lower concentrations coupled with hybrid sources, and the use of separate therapeutic laser treatment are required.
Conclusions
We concluded that the use of hybrid LED-laser sources, as a method of catalyzing high concentration (35% HP) bleaching agents, was not more effective than LED sources used alone, although the two methods were effective for bleaching. The laser element of this hybrid source was not able to prevent or even reduce tooth sensitivity caused by this bleaching technique.
Footnotes
Author Disclosure Statement
No competing financial interests exist.