
Abstract
Introduction
T
The dose of ionizing radiation, amount of salivary tissue exposed, and patient's individual response are the main factors influencing glandular alterations. 4 –6 Damage becomes irreversible after cumulative doses ranging from 26 to 39 Gy, and the salivary flow rate (SFR) can decrease by 10% from the one presented before radiation. 7,8 Despite being stable, as they do not have high mitotic rates, acinar cells respond quickly to radiation. 9,10 The mechanisms that lead to tissue destruction and salivary gland radiosensitivity have not been totally understood so far. Salivary gland alterations start with the damage to the cell membrane, with loss of response to the autonomic controls, and progression to edema, degeneration, and acinar cell apoptosis. Acute effects start 24 h after therapy starts, and stabilize within 72 h. Late effects are the consequence of fibrosis and acinar atrophy, 11,12 which occur as a result of mesenchymal alterations, including changes in the extra cellular matrix, specifically in the lamilin and in collagen IV. 13,14
Low-level laser therapy (LLLT) is a simple low-cost tool that can be used as an adjuvant to conventional treatments, or alone and electively in some diseases. 15 –18 Its effects are based on the modulation of several metabolic, biochemical, and photophysical processes that transform laser light into useful energy for the cell. LLLT's effect on xerostomia has been investigated in clinical and pre-clinical studies. 16,17,19,20 Simões et al. 16 have demonstrated that LLLT increased the SFR and the levels of salivary proteins in Wistar rats. In patients irradiated in the head and neck region, Lopes et al. 19 and Simões et al. 20 have shown that LLLT decreased xerostomia and increased stimulated SFR.
The objective of the present pilot study was to clinically assess LLLT's effect on radiotherapy-induced hyposalivation and xerostomia. In addition, the influence of this therapeutic modality on the quality of life related to oral health (QLROH) was also assessed.
Patients and Methods
Fifty-one patients treated with radiotherapy in the head and neck region were assessed consecutively; these patients came from Rio Grande do Sul State Radiotherapy Services, Brazil (São Lucas Hospital - Pontifical Catholic University of Rio Grande do Sul, Santa Casa Hospital Complex, Bruno Born Hospital, Tacchini Hospital and Charity Hospital). From these, 23 individuals between 37 and 69 years of age were selected, all with a history of head and neck malignancy, treated with ionizing radiation, through fractioned teletherapy, with dosimetry ranging from 45 to 70 Gy. They were all irradiated in cervicofacial region, and both parotids and submandibular glands were involved in radiation therapy portals (uni- or bilaterally).
Patients needed to have been followed up for at least 6 months after radiotherapy (with no relapses or metastasis), with a present Karnofsky 21 performance scale ≥60, present xerostomia, and hyposalivation (unstimulated salivary flow rate <0.1 mL/min and, under stimulation, <0.7 mL/min). The individuals were randomly distributed into a laser group (n=12) and a control group (n=11). All the patients received instructions regarding oral hygiene and mucosal hydration (through frequent ingestion of water), and were advised to avoid spicy and citric foods consumption, as well as alcoholic beverages and tobacco. The study flow chart is shown in Fig. 1.
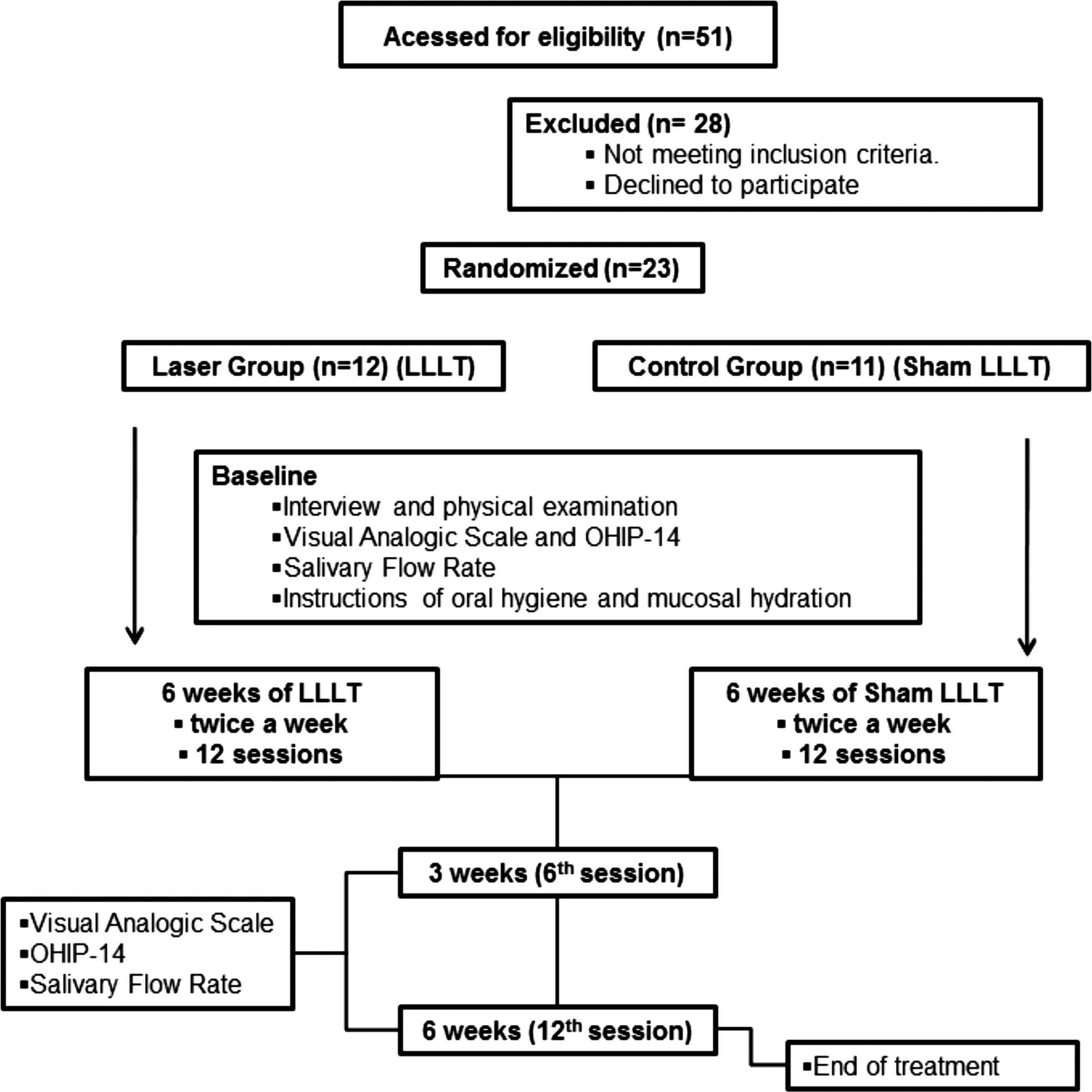
Flow chart representing the stages of the study.
This study was approved by the Ethics Committee of the Pontifical Catholic University of Rio Grande do Sul (Protocol 10513712.7.0000.5336). All the patients signed the Informed Consent Form.
Xerostomia and SFR
A Visual Analog Scale (VAS) developed by Pai et al., 22 consisting of eight items related to xerostomia and quantified by 10 cm long horizontal lines, was used for xerostomia assessment.
Stimulated and unstimulated whole SFR were determined. Samples were collected in the morning, between 8:00 and 11:00 a.m., in previously weighed polypropylene vials. Patients were advised not to ingest food or drink, not to use cosmetics or drugs on the lips, and not to smoke or undergo physical stress 1 h before the procedure. For unstimulated saliva sampling, patients were advised to keep their lips slightly open, allowing saliva to run passively into a vial for 15 min. For stimulated salivary sampling, a 1.0 cm long and 0.5 cm diameter latex cylinder held by dental floss was used. Stimulation was performed for 5 min, and at each minute the content collected was deposited into the vial. The content of both samplings was weighed on a precision scale and transformed into mL/min. 23,24
Xerostomia and SFR were assessed at baseline after the 6th session, and at the end of the 12th treatment session.
QLROH
The QLROH was assessed through the Oral Health Impact Profile (OHIP-14) questionnaire, Portuguese language version. 25 This tool was used at baseline, after the 6th session and after the 12th treatment session.
LLLT
A GaAlAs diode laser was used (Thera Lase® DMC Equipamentos Ltda., São Carlos, SP, Brazil). Laser irradiation was performed in continuous wave mode. The following parameters were used: 830 nm (infrared) wavelength, 100 mW output power, 3.57 W/cm2 power density, 71 J/cm2 dose per point, 2 J energy per point, application time 20 sec per point, and 28 J dose per session. The area of the spot tip of this tool is 0.028 cm2. Patients underwent two LLLT weekly sessions for 6 weeks, for a total of 12 sessions. The laser was calibrated before each session of LLLT; the laser device had a system of calibration coupled to the equipment. Furthermore, after calibration, we used a power meter to check the output power.
LLLT was performed on the major salivary glands punctually. Three points were applied to each parotid gland, two to each submandibular gland, and two to each sublingual gland. 19 A total of 14 points were applied per session. The tip of the tool remained in contact with and perpendicular to the patients' skin during the applications on the parotid and submandibular glands. On the points meant for the sublingual glands, the tip was placed perpendicular to and in contact with the floor of the mouth.
The same number of sessions and application protocol were used with the control group as with the laser group; however, the tool had a plastic tip with a rubber interior that blocked radiation emission, which was confirmed by means of a power meter before the applications in the control group.
Statistical analysis
Stimulated and unstimulated SFR, as well as the scores from the QLROH (OHIP-14), were compared between the groups by the Mann–Whitney test. In each group, in order to compare the SFR and the quality of life scores obtained at baseline, after the 6th and 12th sessions of LLLT, the Friedman test was used, complemented by its multiple comparison test. The VAS scores were assessed by using the repeated measures analysis of variance (ANOVA) complemented by the Tukey multiple comparison test. Values of p≤0.05 were considered significant.
Results
Characterization of the sample
The demographic characteristics of the sample, TNM classification of tumors, the treatments for the malignancies, systemic alterations, and drugs used during the study are shown in Table 1. The time between radiotherapy and the beginning of the study was ∼46 months in the control group and 40 months in the laser group. Tobacco and alcohol had been used by 73.91% and 52.17% of the patients in the sample, respectively, until the moment the malignant neoplasia was diagnosed. At the time they were included in the study, all patients had already discontinued the use of those substances.
Xerostomia and SFR
Xerostomia scores, which were assessed by VAS, presented no significant difference between the groups at baseline, after the 6th session, or at the end of the treatment (12th session). However, both in the laser group and in the control group, there was a significant decrease in xerostomia at the end of the 12th session of the treatment if compared with the assessment conducted in baseline (Table 2).
Means followed by different letters in the column differ significantly through analysis of variance (ANOVA) test, using repeated measurements design, complemented by Tukey multiple comparison test, with 5% significance level.
The stimulated and unstimulated SFR did not differ significantly between the groups at baseline, after the 6th session, or at the end of the treatment (12th session). When comparing the SFR of each group at different experimental times, a significant increase in unstimulated SFR was observed at the end of the treatment in the control group (Table 3).
Comparison between groups: Mann–Whitney test.
Comparison between times of the study: mean ranks followed by different letters in the column differ significantly in the Friedman nonparametric test, complemented by his multiple comparison test, at a 5% significance level.
QLROH
The QLROH, assessed through OHIP-14, did not differ significantly between the groups at baseline, after the 6th session, or at the end of the treatment (12th session). Both in the laser group and in the control group, there was a significant decrease in the OHIP-14 scores at the end of the treatment when compared with the assessment conducted at baseline (Table 4).
Mann–Whitney test significant at p≤0.05.
Comparison between groups.
Superscript capital letters show the comparison between times of the study within each group.
Discussion
The present pilot study has investigated LLLT's effect on hyposalivation and xerostomia in patients with head and neck malignancies treated with radiotherapy. All the selected patients presented important salivary dysfunction as a consequence of radiotherapy. Although the literature show, in pre-clinical and clinical studies, the benefits of LLLT in salivary flow increase, 16,19,20,26 –30 there is not any study investigating its effects on patients who have already undergone radiotherapy treatment, and present hyposalivation and xerostomia as sequelae.
Low-level laser radiation is a nonionizing and noninvasive form of radiation, well tolerated by the tissues and with no mutagenic effects. LLLT's effects on salivary glands have not been completely understood so far. Studies have shown an increase in the number of duct epithelial cell mitoses, and stimulation to protein synthesis in submandibular glands of rats. 26,31 As a result of mitochondria stimulation, increase in adenosine triphosphate (ATP) levels, increase in glucose consumption by the cells, and the intracellular calcium level, LLLT can promote cell proliferation and increase in the antiapoptotic protein expression, as well as increase blood microcirculation in the salivary glands. 19,29,32,33 However, the present study has not confirmed the hypothesis that LLLT could stimulate residual gland function in patients who have had head and neck radiotherapy. No significant difference was observed between laser and control groups regarding the SFR and OHIP-14 scores and VAS. When using LLLT in head and neck irradiated patients, Cowen et al., 34 Lopes et al., 19 Simões et al., 20 and Oton-Leite et al. 30 observed a decrease in xerostomia and an increase in the SFR, suggesting lasertherapy as an adjuvant in the treatment of salivary alterations as a consequence of radiotherapy. However, in those studies, LLLT was applied concurrently to radiotherapy, that is, when irreversible morphological alterations such as acinar atrophy and fibrosis had not been produced in the major salivary glands yet. In contrast, in the present pilot study, patients had ended radiotherapy for at least 6 months; therefore, the negative results obtained with regard to LLLT can be attributed to late alterations caused by ionizing radiation in the glandular structure. All patients had received ionizing radiation doses ranging from 45 to 70 Gy, which several authors 35 –37 consider irreversible for glandular function restoration.
At the end of the treatment, however, there was a decrease in xerostomia, and improvement in the QLROH in both groups. It is important to highlight that all patients were advised, early in the experiment, about the importance of oral mucosa hydration, dental hygiene care, and frequent stimulus of the salivary glands. Those recommendations were reinforced at each of the 12 sessions regardless of the group the patient was in. The assistance to the individuals, given during the 6 weeks of the study, was the determining factor for the improvement of xerostomia and QLROH, showing the need for a follow-up for the head and neck irradiated patients, in order to manage the sequelae caused by radiotherapy. Decrease in xerostomia was not followed by a clinically significant increase in the amount of saliva. Dawes 38 and Jensen et al. 39 suggest that xerostomia does not necessarily present correlation with the SFR. Bhide et al. 40 mention that the difference between patient perception and salivary flow could be affected by external factors.
Although there was no difference in the SFR between the laser and control groups, a significant increase in the unstimulated SFR was observed in the control group at the end of the experiment, in relation to the baseline assessment. With regard to the stimulated whole saliva, the values obtained at the end of the study did not differ from the baseline values in either group. The result of the unstimulated SFR in the control group, despite being statistically significant, did not have any clinical significance once the values were much below what is considered normal. The median of the unstimulated SFR in that group was 0.028 mL/min at the end of the study, whereas the normal value is 0.1 mL/min. During randomization, the laser group had two patients with bilateral neck dissection and excision of both submandibular glands, whereas the control group did not have patients in such condition. Taking into consideration that the submandibular glands supply two thirds of unstimulated whole saliva, that factor might have justified the difference in unstimulated SFR in the control group.
The lack of an LLLT therapeutic protocol made these study methodological definitions difficult. In the literature, the power, power density, wavelength, and all other parameters differ considerably in the studies that used LLLT for xerostomia treatment. 19,20 We have opted for using the infrared wavelength because of the depth of the glandular parenchyma to be irradiated. 17 The frequency of the sessions in the other studies ranged from once a week 20 to daily. 19 In the present study, the sessions took place twice a week for 6 weeks, with the objective of keeping a steady cell response and maintaining the patients' adherence to therapy. Furthermore, as some authors mention that LLLT can stimulate not only the healthy cells but also the tumor cells, 41 –43 during LLLT applications, the areas close to the already-treated tumor lesions were avoided.
As xerostomia has serious consequences to the patients' quality of life, we have opted for assessing the QLROH, using the OHIP-14. Nowadays, several tools are available for that purpose, although not a single one could be considered a gold standard. 44 Taking into account the decrease in the OHIP-14 scores along the 6-week study, the relationship between xerostomia relief perception and improvement in the quality of life of the individuals in the research is evident.
Saliva plays an important role in the oral and general homeostasis, once salivary dysfunctions predispose individuals to several complications. Radiotherapy performed in the head and neck region is one of the main causes of salivary disorders, interfering negatively with the patients' quality of life. Some studies have evidenced the LLLT benefits to the gland function during the radiotherapy treatment. However, the results of the present pilot study show that in patients given a 45 Gy minimum dose in the head and neck, 12 LLLT sessions applied for 6 weeks were unable to promote salivary flow increase. The degree of cell destruction caused by radiotherapy, especially on the parotids, might have been one of the main factors associated with the results. Nevertheless, xerostomia and quality of life showed improvement, thus highlighting the importance of advice to the irradiated patients and follow-up. New therapeutic modalities, especially in tissue engineering, must be further investigated in order to restore the gland function and, therefore, improve the quality of life of patients with radiotherapy sequelae.
Conclusions
In the parameters used, LLLT was not able to increase SFR, or decrease xerostomia, hence the hypothesis that LLLT could stimulate residual gland function in patients treated with head and neck radiotherapy has not been confirmed. The results may be associated with the late effects of radiotherapy on glandular structure, such as fibrosis and acinar atrophy.
Footnotes
Acknowledgments
The authors thank National Council for Scientific and Technological Development (CNPQ) and Radiotherapy Service of São Lucas Hospital (PUCRS, Brazil) for their contributions to the development of this research.
Author Disclosure Statement
No competing financial interests exist.