
Abstract
Introduction
B
The pathophysiology of BRONJ remains poorly understood, but the main theory focuses on the impact of BPs on bone, particularly inhibition of osteoclast function and subsequent suppressed bone turnover. 1,2 Antiangiogenic properties of aminobisphosphonates (NBPs) and soft tissue toxicity have also been documented with in vivo and in vitro studies. 3
Several systemic and local potential risk factors associated with the development of BRONJ have been identified. Intravenous use, nitrogen-containing forms of BPs, and dentoalveolar trauma are the factors that are more frequently associated with BRONJ development. 4 The significance of other factors such as renal dialysis; obesity; diabetes; and chemotherapeutic agents including cyclophosphamide, erythropoietin, and corticosteroids; tobacco use; and genetic susceptibility are still being investigated. 5
Ruggiero et al. introduced a staging system for BRONJ that recognizes three different clinical levels, which was later modified by Bagán et al. in 2009 with the introduction of two levels of second stage BRONJ lesions. 5,6 Following identification of an unexposed form of the disease by Junquera et al., the American Association of Oral and Maxillofacial Surgeons (AAOMS) introduced Stage 0, which is defined as a BRONJ lesion with no evidence of exposed bone, but the presence of nonspecific symptoms and/or clinical and radiographic findings of a possible BRONJ lesion. 1,7
Treatment strategies of BRONJ have so far been controversial, and there are no documented standard strategies that have shown consistent resolution of BRONJ. 8 Recommendations range from conservative management to extensive surgical intervention, including resection and subsequent reconstruction. First introduced as a therapeutic modality by Mester et al., low-level laser therapy (LLLT) is used in various areas of the biological sciences to promote tissue regeneration of injured tissues. 9,10 Biostimulatory effects of LLLT have been mainly attributed to increase in cell proliferation and metabolism, and expression of several genes involved in healing processes. In their recent study, Lee et al. studied effects of GaAlAs diode laser biostimulation on BP exposed oral keratinocytes, and demonstrated favorable results on overcoming the inhibitory effects of BPs. 11 In a similar study, Bayram et al. investigated the effects of GaAlAs diode laser biostimulation on alkaline phosphatase (ALP) activity of zoledronate treated human osteoblast-like cells (Saos-2), and reported reduction in the detrimental effects of zoledronate and improved cell function/proliferation with LLLT applications. 12
Laser therapy with its ease of application and widely reported favorable effects on tissue healing can be a preferable supportive treatment method for BRONJ lesions. The aim of this study is to retrospectively evaluate the treatment outcomes of 11 patients diagnosed with stage II or III (AAOMS Classification) BRONJ lesions. The surgical removal of BRONJ lesions was performed with pre and postoperative antibiotic administrations, followed by GaAlAs diode laser applications. Successful treatment outcomes of stable mucosal closure and elimination of all symptoms were obtained in all patients.
Materials and Methods
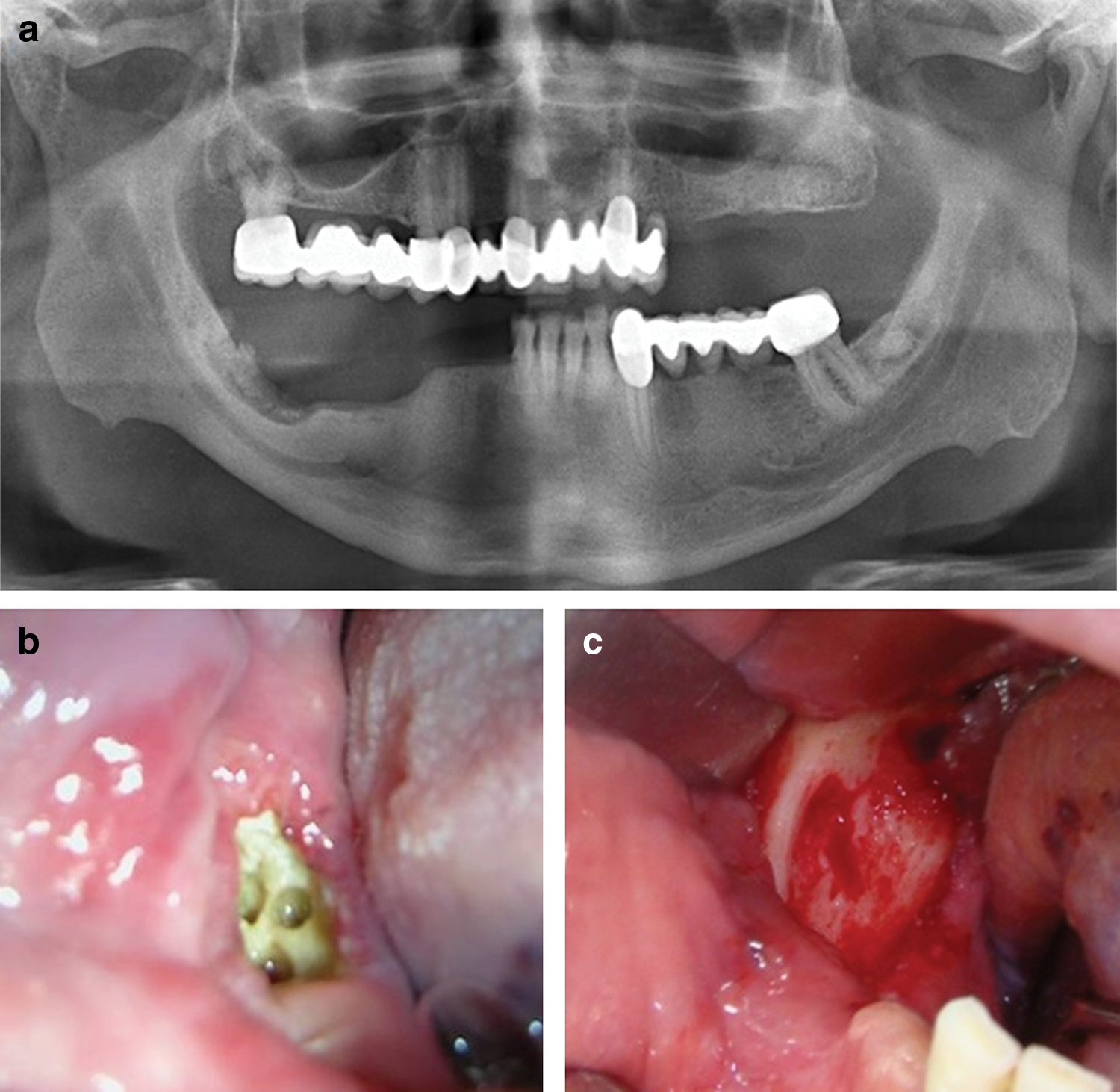
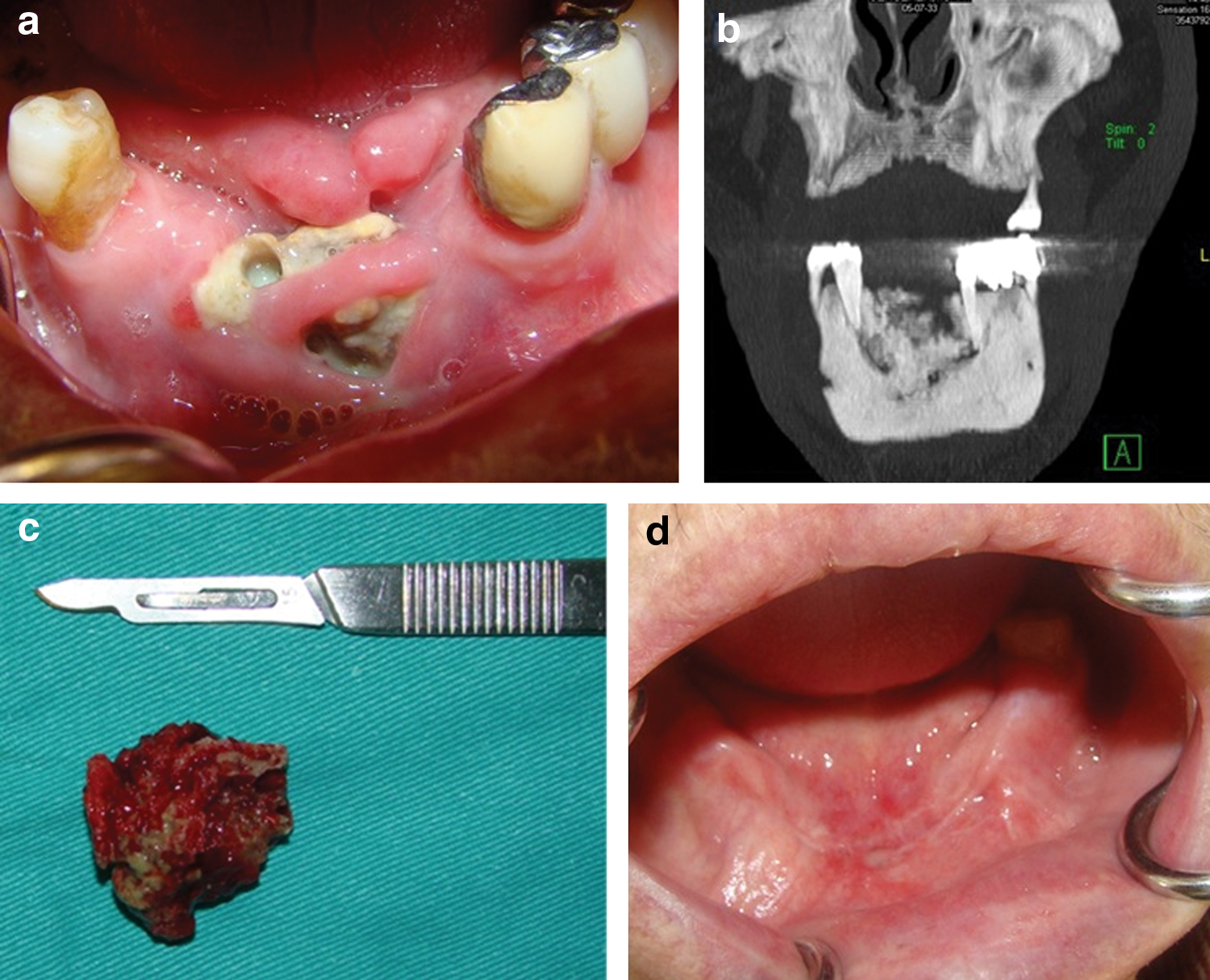
The present study was conducted at Hacettepe University, Faculty of Dentistry, Department of Oral and Maxillofacial Surgery, Ankara, Turkey. Following their classification based on clinical and radiological evaluations, 11 patients (7 males, 4 females, with a mean age of 64.1, ranging between 50 and 78) with AAOMS Stage II and III BRONJ lesions requiring surgical removal in addition to medical therapies were included in the study. (Figs. 1 and 2). All patients had previously been diagnosed and treated for malignant neoplasms with intravenous BPs. A database with detailed history on the route, type, and duration of BP use, sites of BRONJ development, number of individual lesions, predisposing event, primary tumor necessitating the BP therapy, and clinical staging of BRONJ lesions was recorded for each patient (Tables 1 and 2).
(
(
BRONJ, bisphosphonate related osteonecrosis of the jaws; AAOMS; American Association of Oral and Maxillofacial Surgeons.
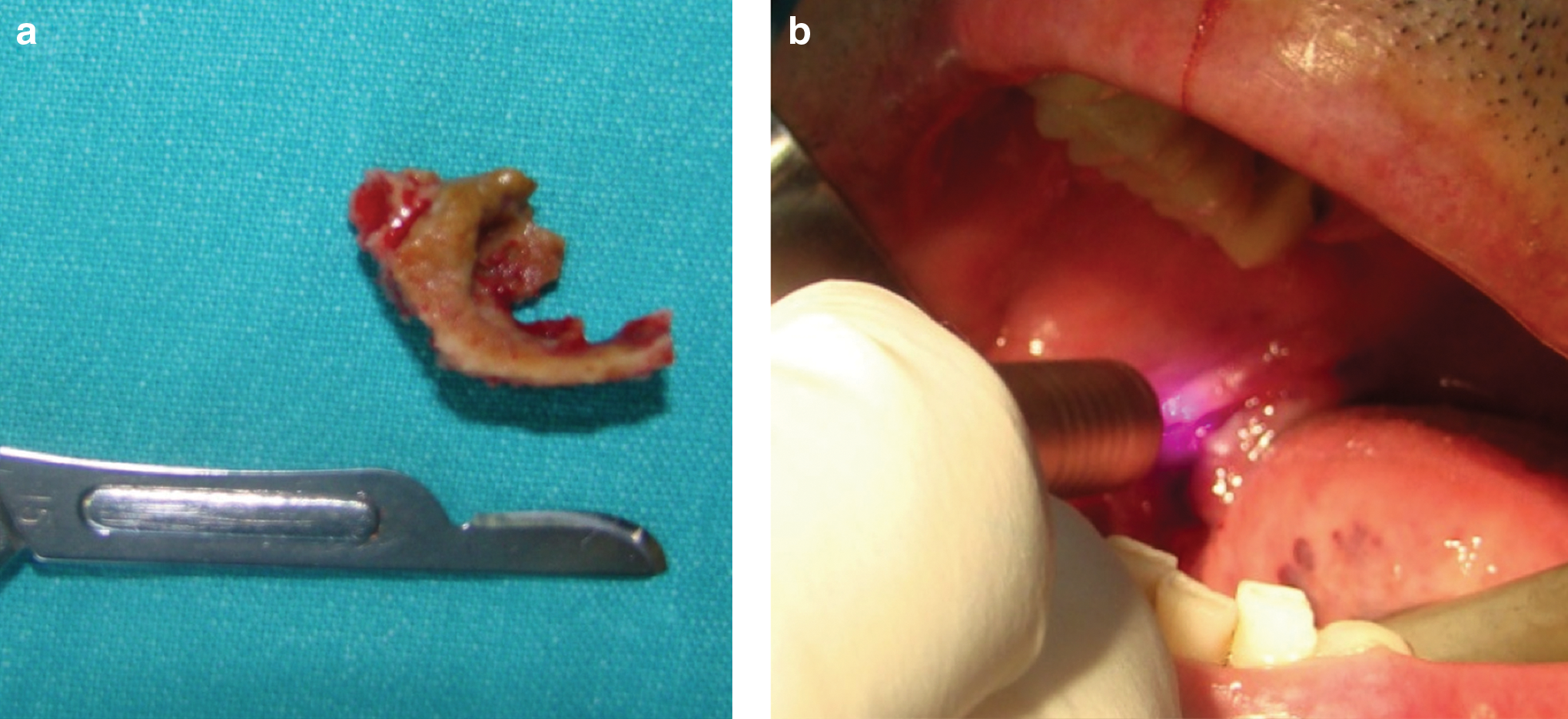
Following consultations to departments in charge of their systemic treatments, all patients were hospitalized preoperatively at the Department of Internal Medicine, Unit of Infectious Diseases, Hacettepe University, Ankara, Turkey for administration of IV antibiotics, and received an antibiotic therapy regimen consisting of sulbactam– ampicillin, 1500 mg four times a day for 7 days. All patients were operated on under general anesthesia. General outline and key points of the surgical procedure were as follows. A mucoperiosteal flap of minimal disturbance to surrounding tissues was reflected. Necrotic bone and overlying granulation tissue were removed. Removal of bone around the margins of the lesion was performed with a bur under copious irrigation, until bleeding bony tissue with a healthy appearance was attained (Fig. 1c). Symptomatic neighboring teeth were extracted and sharp bony edges were removed. Wound margins were renewed, further soft tissue adjustments were performed when required, and tension-free primary closure was achieved. The surgical intervention caused the least possible trauma to surrounding tissues from the incision planning to the closure in all cases. Specimens were sent for histopathological evaluation (Fig. 2c and 3a). All patients received IV antibiotic administration similar to preoperative application during the postoperative hospitalization period. Intraoral LLLT applications were performed on the postoperative days 1, 3, 5, 7, and 10 (Fig. 3b) with a GaAlAs diode laser device (Fotona XD-2, Ljubljana, Slovenia) with the following parameters: continuous wave, noncontact stationary mode, 808 nm wavelength, 0.5 W power, with a spot size of 0.28 cm2 (R=6 mm), for 3 sec per point (10 sec per cm2 and a total of ∼120 sec per entire surgical site), at an energy density of 5 J/cm2 (energy per point,1.4 J). The entirety of the surgical sites was covered with LLLT applications on multiple points from buccal (labial) to lingual (palatal) aspects at a distance of 0.5–1 cm from oral tissues, which theoretically did not affect the spot size with the handpiece that was used. A summary of the parameters of LLLT application and treatment characteristics is given in Table 3. Recommendations of the World Association for Laser Therapy (WALT) on LLLT were referred to, in order to keep the laser energy at a therapeutic dose level.
(
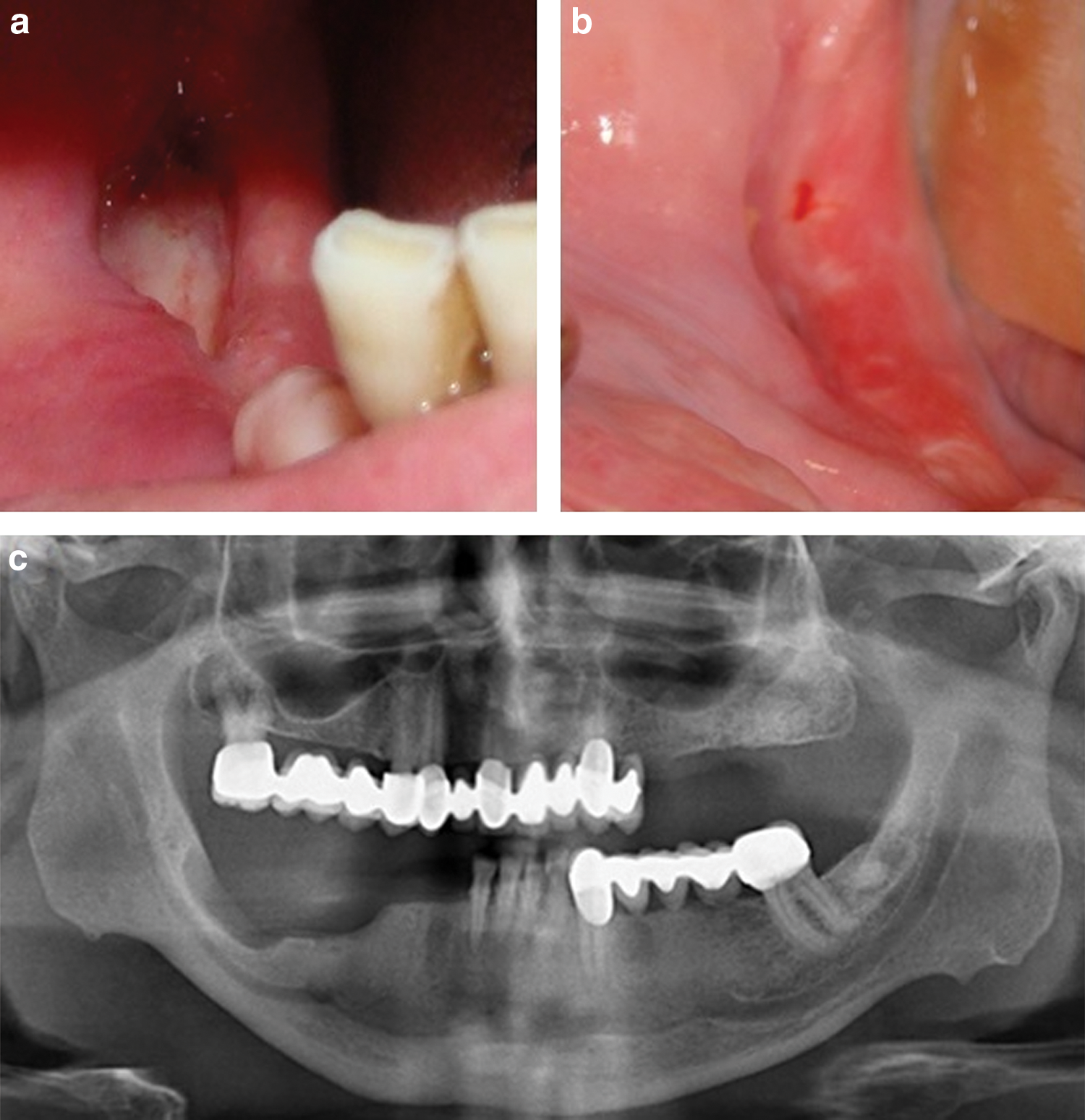
Following their discharge, patients were prescribed an antimicrobial mouth rinse (benzydamine hydrochloride 0.15% – chlorhexidine digluconate 0.12%) and a combined antibiotics regimen (amoxicillin–clavulanate 1000 mg p.o. twice daily, clindamycin 150 mg p.o. four times daily) for 7 days. Sutures were removed on postoperative days 7–10, as the healing process of the wound sites was evaluated for each patient. The postoperative healing period was observed for each patient at weekly and monthly follow-ups within the limitations of that patient's systemic condition and cooperation (Figs. 2 and 4) (Table 2).
(
Results
A summary of the demographic data of the patients as well as type, duration, dose and route of BP treatment; primary disease necessitating BP use; and predisposing local factor are given in Table 1. Table 2 summarizes the localization and number of individual lesions in each patient, AAOMS staging of the lesions based on clinical and radiologic evaluation, healing course, and follow-up length for each patient.
• All patients involved in the present study had been on BP therapy for malignant systemic diseases with associated bone disorders, with multiple myeloma being the most frequently encountered primary disease (four cases). Prostate cancer (three cases) and breast cancer (three cases) with bone metastasis were the second most frequently recorded systemic diseases.
• All patients in the present study had received IV zoledronate application prior to onset of symptoms. The route of administration (IV) and the dose of zoledronate were identical for all patients (4 mg/28 days) with one exception (3 mg/21 days).
• Tooth extraction performed prior to onset of symptoms was identified as the most significant predisposing local factor (nine cases). Denture irritation was recorded as a contributing local factor in two patients.
• Consultations with departments and clinicians managing primary diseases were made for all patients. Intermittence of the BP therapy (drug holiday) was approved for five of the patients. These patients did not receive the last dose of their BP regimen and also did not receive further BP therapy until complete intraoral healing with resolution of all symptoms was achieved. Six patients had already been on a “drug holiday” of durations ranging from 1 month to 3 years prior to BRONJ treatment.
• Whereas nine patients presented with one lesion, two patients had multiple BRONJ lesions. Of all lesions identified in the present study, nine cases were encountered in the mandible and five were encountered in the maxilla. All but two lesions were classified as AAOMS Stage II BRONJ lesions based on clinical and radiological evaluation. Two lesions extending to surrounding anatomical structures [inferior border of the mandible (one case) and maxillary sinus (one case)] were classified as Stage III BRONJ lesions.
• Maintenance of the primary closure and an uneventful healing was achieved in seven patients. Because of the broad extent of the lesions and inadequate bony support, failure of primary closure and consequent secondary healing was observed in four patients. More favorable results were achieved in patients who had been on drug holiday for longer periods.
• Gradual relief of previously recorded symptoms notably evident after postoperative day 3 was recorded for each patient. Pain, the most commonly reported chief complaint prior to treatment, accordingly regressed following postoperative day 3, as none of the patients reported pain on postoperative day 10 when final LLLT application was performed.
• Histopathological evaluations of obtained specimens were nonspecific for all patients.
Discussion
This study retrospectively evaluates the treatment outcomes of 11 patients. Although compatible with the current literature, because of the limited number of subjects included in the study, its findings on the correlation between BRONJ development and parameters such as type, dose, route, duration, and discontinuation of BP treatment as well as other determinants (age, gender, primary disease necessitating BP treatment, predisposing local factor) are not conclusive. However, systemic and local factors that are frequently associated with BRONJ development such as advanced age, IV use of nitrogen containing BP (zoledronate), and history of dentoalveolar trauma, are accordingly amplified in the findings of the current study.
The main goals of BRONJ treatment, as is most frequently pointed out in the current literature, are to eliminate clinical symptoms such as pain, treat infection of the soft tissue or the bone, and minimize the progression of bone necrosis. 13 Clinical markers of success include an intact mucosa with no signs of infection or sinus formation; radiographic markers include the arrest of progression of bony abnormality and remodeling of the affected area. 14 Unlike the goals of BRONJ treatment that are clearly identified, treatment options have so far remained controversial. 4 –6,13 Recommendations ranging from conventional surgery to medical and/or surgical approaches combined with supportive modalities such as hyperbaric oxygen therapy, parathyroid hormone, platelet rich plasma, and LLLT applications have been documented. 4,8,14 –18
Numerous studies on the management of BRONJ with variable success rates have been published. 19 –23 Of the two different approaches that can be clearly identified, conservative management of BRONJ with antibiotics, antiseptic mouthwashes, and pain control is often advocated for earlier stages, but is associated with relatively poor outcomes for further stages of the disease. 19 –21 Hoff et al. reported a 23% healing rate after conservative management, whereas Janovska et al., in their study on 11 patients, concluded that a conservative approach was not curative for BRONJ. 20,21 The other option, different extents of surgical removal of necrotic bone supported with medical therapy, is associated with relatively higher success rates than is conservative management. 22,23 Lazarovici et al. reported wound healing in 84% of the patients with superficial curettage of the lesions. 22 Similarly, Kühl et al. concluded that exploration of the lesion and resection of the necrotic bone were beneficial for 80% of the BRONJ patients in their study. 23 More radical surgical management comprising en bloc resection and reconstruction is advocated where there are large segments of necrotic bone or a pathological fracture (AAOMS Stage III). 19 Guidelines for optimal surgical intervention also remain unclear. Whereas some authors recommend the removal of the symptomatic segment only, causing minimal soft tissue disturbance, others advocate more extensive soft and hard tissue debridement and primary closure of the wound. 14,24
Our findings of eliminated symptoms and intact oral mucosa on operative sites with no recurrent lesions can be regarded as clinical success, and if confirmed with further research, may serve in an effort to reach a consensus on the most viable treatment option for BRONJ lesions with similar extent. Removal of avascular exposed segments, curettage of surrounding hard and soft tissues followed by primary closure of the wound site with pre and postoperative antibiotics administration, based on the authors' experience, are indispensable medical-surgical elements of clinical success in the treatment of BRONJ lesions.
Several studies in the literature have reported the use of lasers in BRONJ treatments, used as the main surgical tool or as an adjunct to other therapeutic approaches. Resection of necrotic bone segments with Er:YAG laser combined with Nd:YAG LLLT applications have previously been described by Vescovi et al. 15 Findings of their study indicated more accomplished outcomes of BRONJ management and improved quality of life with laser surgery and subsequent LLLT application when compared with medical therapy alone or other treatment options. A relatively recent study of the same group of researchers also evaluated treatment outcomes of a similar treatment approach of AAOMS Stage I BRONJ lesions, which confirmed the findings of their previous study concluding that conservative surgical strategies, possibly with laser, may determine a higher control of AAOMS Stage I BRONJ lesions in the long term. 25
When applied at a low intensity level, lasers are proven to have analgesic, antimicrobial, anti-inflammatory, and biostimulation effects that may enhance the healing of patients with BRONJ lesions. In a recent study, da Guarda et al. reported positive effect on healing of a BRONJ lesion and remission of painful symptoms with GaAlAs laser biostimulation. 16 Likewise, Scoletta et al. described the use of pulsed low-level diode laser biostimulation in multiple myeloma patients suffering from BRONJ. 17 They reported statistically significant differences in pre and postoperative scores of parameters such as edema, fistula, and pus formation when laser biostimulation was used. Managing pain, a commonly reported finding of BRONJ, accordingly benefits from LLLT applications. In correlation with Scoletta et al.'s study, Romeo et al. obtained satisfactory results in pain control parameters in BRONJ patients with GaAs diode laser applications. 18 Tooth extraction, which is regarded as a potential risk factor in patients on IV BP treatment, was safely performed with subsequent LLLT applications, and favorable results were obtained in Kan et al.'s study. 26
These positive clinical results can be clarified by experimental studies focusing on the intracellular effects of lasers when applied at a low-intensity level. In their study, Honmura et al. reported anti-inflammatory effects of LLLT and enhanced healing when they compared tumor necrosis factor (TNF)-α and interleukin (IL)-1expression levels on experimentally induced inflammation in rats.
27
In a relatively recent study, Huang et al. reported increased MG63 cell proliferation and reduced inducible isoforom nitric oxide synthase (iNOS), TNF
Antimicrobial effect is another potential benefit that can be provided with LLLT application. In a recent study in which authors evaluated the antimicrobial effectiveness of different lasers on contaminated titanium discs, Tosun et al. indicated favorable antibacterial effects of GaAlAs diode laser application, reporting antibacterial effectiveness up to 100%. 31 Likewise, Maver-Biscanin et al. reported destruction of oral bacterial and fungal species with LLLT applications. 32
With regard to variable success rates of recommended treatment strategies, it can be concluded that there is need for additional studies to obtain more evidence concerning treatment outcomes of BRONJ. 23 LLLT application has the potential of providing enhancement in healing of traumatized oral tissues via several routes, including anti-inflammatory, antimicrobial, and biostimulatory effects. Therefore, the favorable findings of the present study may be regarded as indicative of the contribution of LLLT. Additionally, when the history of IV zoledronate use in all of our patients is taken into consideration, which is commonly associated with relatively poor treatment outcomes, the findings of the present study may be considered particularly remarkable. In our experience, BRONJ lesions can effectively and safely be treated when the surgical procedure is performed in an atraumatic manner, under high doses of antibiotic therapy, and supported with diode laser LLLT applications, which satisfactorily and safely serve as a complementary method to conventional medical and/or surgical interventions.
Conclusions
Because of its noninvasive, nonpharmacologic characteristics; ease of application; clinically proven capacity of improving tissue repair; and favorable results obtained in the present study, laser power when applied at a low-density level, may serve as a strong supportive modality when treating patients with BRONJ lesions. However, further controlled clinical trials performed in different oral care centers with a larger sample of patients are required to confirm LLLT's role in the “ideal treatment” of BRONJ lesions.
Footnotes
Author Disclosure Statement
No competing financial interests exist.