
Abstract
Introduction
T
Ethylenediaminetetraacetic acid (EDTA), a calcium chelating agent, is commonly used to remove the smear layer. 7 Previous research has demonstrated that a final irrigation with 17% EDTA, followed by sodium hypochlorite (NaOCl), removes the smear layer in its entirety. 8
In recent studies, lasers have been proposed as an alternative method for disinfecting root canals and removing smear layer and debris. 9,10 The erbium, chromium: yttrium-scandium-gallium-garnet (Er,Cr:YSGG) is a water-absorbing infrared laser that has the potential to clean root canals in different output powers of 1–3 W. 5,9,11 Removal of the smear layer by using an Er,Cr:YSGG laser has been studied previously using different techniques, and under different conditions. Nevertheless, inconsistencies in the sizes of firing tips and apical preparation in some of these studies raise questions about the actual depth of laser irradiation. 11 The effect of laser-driven irrigation using Er,Cr:YSGG lasers for the purpose of cleaning root canal walls has been studied by Peeters and Suardita. 5 However, their combined model of EDTA irrigation and laser irradiation without entering the firing tip into the root canal space did not assess the singular effect of laser irradiation on smear layer removal. In addition, new methods of removing the smear layer should be explored, as previous literature has shown that EDTA irrigation can increase the fracture susceptibility of tooth roots. 12 Previous literature has also failed to evaluate the quality of smear layer and debris removal in all three segments of the root canal space. The purpose of the current study is to evaluate the efficacy of Er,Cr:YSGG laser irradiation using two different output powers on smear layer and debris removal in the coronal, middle, and apical thirds of root canal walls compared with the conventional EDTA/NaOCl irrigation technique.
Materials and Methods
The present study was approved by the Ethics Committee of the Dental School of Tehran University of Medical Sciences, Tehran, Iran. A total of 60 caries-free single-rooted human teeth with straight canals, extracted for periodontal reasons, were selected. Study teeth were radiographically assessed to ensure the absence of calcification, resorption, or curvature in the root canals. The teeth were cleaned (soft tissues and calculi were removed from the teeth) and placed in 5.25% NaOCl for 2 h for surface disinfection. All samples were then stored in distilled water until the time of root canal preparation.
The crown of each tooth was sectioned at the cementoenamel junction (CEJ) by a water-cooled low-speed diamond disk (Struers, Ballerup, Denmark), creating an average root length of 14–17 mm. A K-file #15 (Dentsplay Maillefer, Ballaigues, Switzerland) was inserted into the root canals until it was visible at the apical foramen. The working length was determined visually by subtracting 1 mm from the measured length.
The root canals were prepared using a step-back technique and two rotary files (VDW, Munich, Germany). Five instruments were used at working length in each canal according to the manufacturer's instructions in the following sequence: (1) size 15, 0.05 taper; (2) size 20, 0.06 taper; (3) size 25, 0.06 taper; (4) size 30, 0.05 taper; and (5) size 35, 0.04 taper. Root canals were irrigated between each instrument using 5 mL of 0.2% Chlorhexidine (CHX) (Natural Pharma, São Paulo, Brazil). A final rinse with distilled water was implemented to remove CHX from the root canals. The specimens were then randomly divided into three experimental groups, based on the method used for removing the smear layer, and one positive control group (group 4) which received no further treatment (n=15 per group).
In group 1, root canals received an irrigation regimen composed of 2 mL of 17% EDTA (pH=7.4) (DiaDent, Europe B.V. Almere, Netherlands) for 1 min, followed by 5 mL of 5.25% NaOCl for 2 min. In group 2, the canals were filled with distilled water and received 2.78 μm Er,Cr:YSGG laser irradiation (Waterlase Millenium, Biolase Technology, San Clement, CA), with a 320 μm diameter radial firing tip (RFT3 Endolase, Biolase Technology, Inc; calibration factor of 0.85) and the following parameters: panel output power of 1.5 W, pulse duration of 140 μs, pulse frequency of 20 Hz, and 15% water pressure to 15% air pressure ratio. 13,14 The energy per pulse of 42 mJ and energy density of 5.25 J/cm2 were calculated. The laser tip was inserted into each canal at the working length and moved continuously in a circular motion from the apex to the crown at a speed of 2 mm/sec. In group 3, the irradiation protocol was identical to that of group 2; however, the output power of the laser was set at 2.5 W. Laser irradiation was performed at room temperature (25°C) and repeated three times with a 20 sec break between each irradiation. To ensure standardized and stable power outputs, a power-meter (FieldMaster, Coherent Inc., Auburn, CA) was used to calibrate the output powers prior to each irradiation. Finally, all root canals were irrigated with 5 mL of saline solution and then carefully dried with sterile paper points #35 (Dentsply Ind. e Com. Ltda., Petropolis, RJ, Brazil).
Scanning electron microscope (SEM) evaluation
Root slices were prepared by sectioning the roots parallel to the roots' long axis using a water-cooled diamond blade on a precision cutoff machine (Mecatome, Persi, France). For each root, the half section that contained the most substantial part of the root was coded and retained in a desiccator under a vacuum for 24 h. The coded specimens were mounted on an aluminum stub, coated with 25 μm of gold-palladium, and examined under an SEM (JSM-6400; JEOL, Tokyo, Japan). Sixty scanning electron microscopy photomicrographs were taken of the coronal, middle, and apical thirds of each specimen at 2000× magnification. Smear layer was defined as a surface film of debris that was retained on the dentine after instrumentation.
15
Debris was defined as dentine chips, remnants of pulp, and particles that were attached loosely to the root canal wall.
15
The images were analyzed independently by three calibrated, blinded evaluators according to the following five score criteria
5
for both the smear layer and debris removal evaluations. Score 1: No detectable smear layer, and clean root canal walls with very little to no debris; all dentinal tubules were clean and open. Score 2: Clean surfaces containing small agglomerations of debris and/or a thin homogenous smear layer; most of the dentinal tubules were open. Score 3: Many agglomerations of debris, and a homogenous smear layer covering <50% of the canal wall; only a few dentinal tubules were open. Score 4: Mostly contaminated surfaces with a heavy homogenous smear layer and a large amount of debris covering >50% of root canal walls; no dentinal tubules were open. Score 5: Contaminated root canal walls entirely covered by a heavy and inhomogeneous smear layer and debris.
The Cohen κ analysis was used to analyze the agreement among the three evaluators. The data were analyzed using the Kruskal–Wallis nonparametric analysis of variance and Dunn tests. The significance level was set at α=0.05.
Results
The Cohen κ analysis showed excellent reliability and reproducibility among the evaluators with values ≥0.9 for both categories. The results for the smear layer and debris scores in the coronal, middle, and apical segments of the root canals in each group are shown in Tables 1 and 2.
NaOCl, sodium hypochlorite; EDTA, ethylenediaminetetraacetic acid.
NaOCl, sodium hypochlorite; EDTA, ethylenediaminetetraacetic acid.
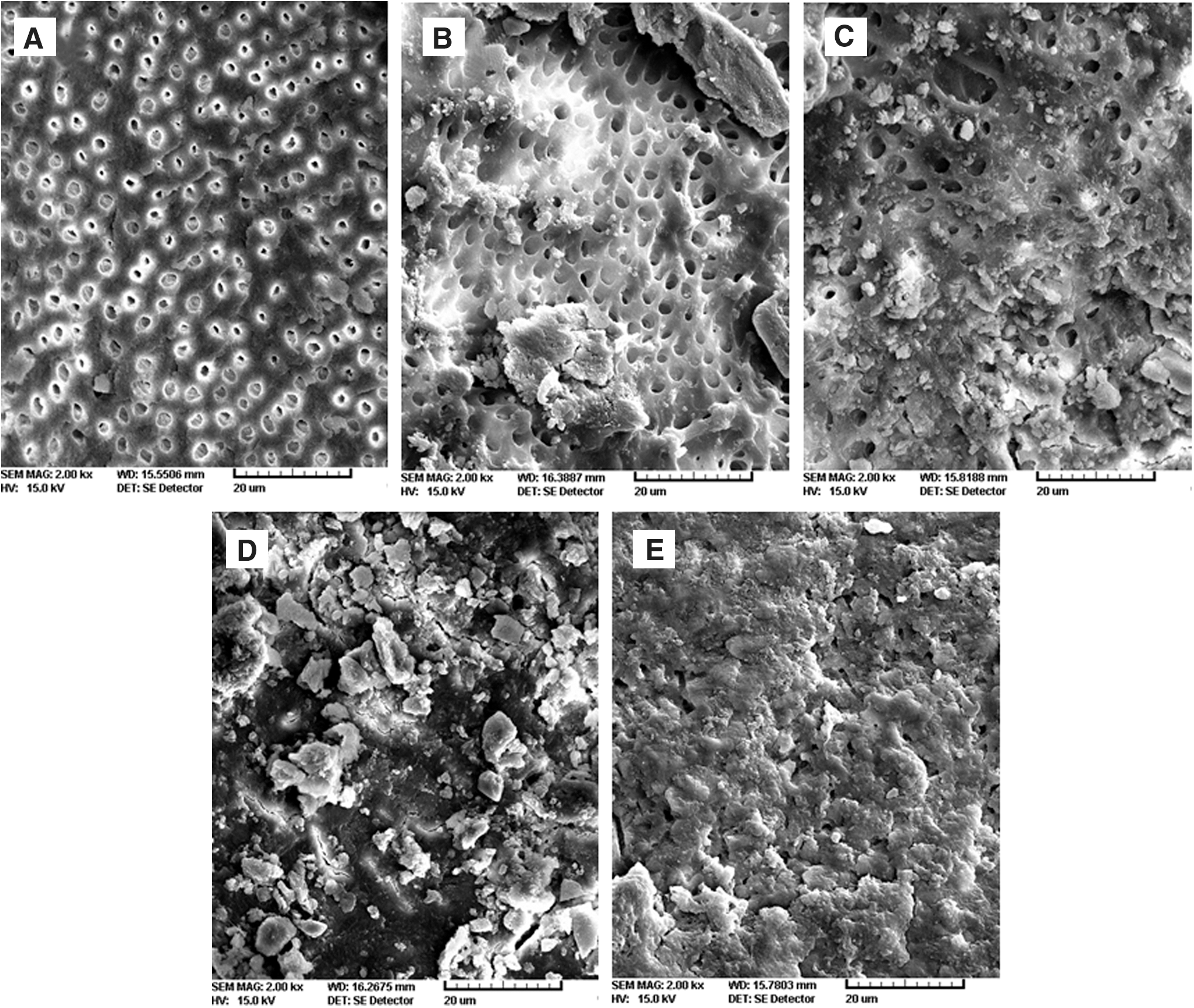
Figure 1 shows examples of different scores for the smear layer and debris observed in the samples.
Analysis of the smear layer
The Kruskal–Wallis test showed a significant difference among all groups/areas regarding the smear layer scores (p<0.001). The analysis of the root canal surfaces in group 4 (control group) showed the presence of a heavy smear layer (score 5) throughout the entire length of the canals (Fig. 1E). The results of the Dunn test showed that the scores of the smear layer for the group 1 (EDTA+NaOCl), group 2 (1.5 W laser), and group 3 (2.5 W laser) were significantly different from the control group in all areas (adjusted p<0.001). No significant difference was observed between groups 1 and 2 in all sections – the coronal, middle, and apical thirds – of the root canals. In group 3, substantial amounts of smear layer were observed with several areas of thermal damage to the dentinal walls (Table 1) (Fig. 1D). Analysis of the scores showed significantly higher scores for the smear layer in group 3 than in groups 1 and 2 in all sections (p<0.0.5). In each experimental group, the SEM results of the apical third of the canals presented the highest amounts of smear layer left remaining (Table 1).
Analysis of the debris
The Kruskal–Wallis test showed a significant difference among all groups/segments regarding the debris scores (p<0.001). In the coronal third of the canals, the quality of debris removal was significantly better in group 1 than in group 2 (adjusted p<0.05), and it was significantly better in group 2 than in group 3 (adjusted p<0.05). In the middle and apical thirds of the canals, group 1 showed significantly better results than each of the laser groups (adjusted p<0.05). There was no significant difference between the laser groups regarding debris removal in the middle and apical thirds of the canal walls. In each experimental group, the SEM results of the apical third of the canals presented the highest amounts of debris left remaining (Table 2).
Discussion
Removing the smear layer without causing unfavorable changes in root structure has proven to be a challenge. Irrigation with EDTA followed by NaOCl has been shown to be a reliable method of smear layer removal. 16,17 In the present study, in group 1, smear layer removal was achieved by using 2 mL of 17% EDTA followed by 5 mL of NaOCl for 3 min. Analysis of the data confirmed the efficacy of this regimen in removing debris and the smear layer. However, recent studies have raised concerns about the unfavorable effects of this protocol on dentinal walls and resultant tooth structure. Uzunoglu et al. 12 showed that using EDTA for smear layer removal reduces the fracture resistance of root canal treated mandibular incisors. In addition, the use of EDTA for >1 min can erode and damage root dentin. 18 The long-term effects of EDTA irrigation on the survival of root canal treated anterior teeth deserves further study.
In the present study, laser beams were able to reach the full working length of the study teeth because the firing tips used were smaller than the master apical file size. Chlorhexidine was used for irrigation during instrumentation, and water was used as an intra-canal medium during laser use to ensure that the results obtained after laser use were solely caused by the effects of the laser, and not the irrigation techniques. The generation of shock waves through the activation of water, and the formation of vapor bubbles, are the mechanisms by which erbium lasers are thought to remove the smear layer. 19,20 Illustrative of the above-described phenomena are the results obtained from group 2 in the present study. The Er,Cr:YSGG laser, when used at an output power of 1.5 W, effectively reduced the smear layer in the apical, middle, and coronal sections of the root canal wall. This outcome is consistent with the hypotheses generated in other studies. 13
In contrast to its efficacy regarding smear layer removal, the Er,Cr:YSGG laser failed to effectively remove debris as compared with EDTA and NaOCl (Table 2). Previous studies have shown better results for debris removal using laser-activated irrigation with Er,Cr:YSGG lasers, and Er:YAG lasers compared with passive ultrasonic irrigation techniques. 15,19 However, the models utilized in these studies were made of artificially constructed dentinal grooves. The present study offers a more clinically relevant scenario in which debris removal is evaluated segmentally, and, therefore, at all levels of the root canal.
The difference in the mechanism of action between EDTA and the erbium laser is the likely cause of the results obtained from the experimental groups regarding debris removal. With the exception of a study by Peeters and Suardita, 5 previous literature has not evaluated a Er,Cr:YSGG laser's effectiveness within the context of simultaneous smear layer eradication and debris removal. However, in the clinical environment, smear layer removal and debris eradication are both integral components of the same cleaning process. They occur simultaneously, and ultimately result in a cleaner root canal. The study by Peeters and Suardita 5 showed the combined effect of laser irradiation and EDTA irrigation (called “laser irrigation”) together on the apical third of root canal walls, and, therefore, the exclusive effect of laser irradiation on debris removal is uncertain within the study design. These findings need further investigation. On the other hand, as previous studies showed, use of EDTA can be detrimental to the root structure of teeth with thin roots. 18 Activation of EDTA during laser irrigation can potentially increase the probability of damage. There is lack of information about the possible side effects of laser irrigation on dentinal walls.
The effects of different powers (1–6 W) of erbium laser irradiation on dentinal walls have been studied previously. Cracks and carbonizations on dentinal walls are the result of high power irradiation emitted from erbium lasers (>4 W). 10 In addition, irradiation with low power (1 W) erbium lasers can also cause cracks and carbonizations in the absence of a coolant. 10 Chemical analysis of specimens irradiated with Er,Cr:YSGG lasers with an output power of 3 W showed no significant change in the Ca/P ratio of dentinal walls. 11 Although the study shows an absence of change in dentin at the molecular level, it did successfully document the presence of thermally damaged tooth structure. 11 Thermal damages were described as carbonizations, the partial melting of dentinal tubules, and the occlusion of tubule orifices in the melted regions. 11 Results obtained from group 3 (2.5 W) of the present study showed similar results regarding thermal damages. Also, the higher power of laser irradiation (2.5 W) failed to remove the smear layer when compared with the lower power (1.5 W). This finding may not be consistent with previous studies. 10,11 Differences in study methods include the size of the laser tip, the characteristics of laser irradiation, the size of the apical preparation, and the type of media utilized. These findings show that when a Er,Cr:YSGG laser tip reaches the extent of the working length, increasing the power >1.5 W not only causes thermal damages potentially, but also does not remove the smear layer effectively. In other words, the high power laser itself might become a source of smear layer formation because of the structural damage that it causes in the dentinal structure.
In the present study, all experimental groups showed better smear layer and debris removal in the coronal and middle thirds of the study teeth than in the apical thirds. This finding is consistent with the results of other studies. 21 The increased incidence of accessory and lateral canals in the apical third where the laser beam or irrigation solution cannot reach may be the reason for this finding. Although complete removal of the smear layer in the apical third has been achieved by using a laser- driven irrigation protocol, the combination of laser irradiation and EDTA irrigation, by Peeters and Suardita, 5 with laser irradiation for 60 sec, raises safety concerns for clinical applications. A similar study showed that laser irradiation using EDTA as an intra-canal media can predictably remove the smear layer in the apical third of root canals. 22 The outcome of the present study shows that an Er,Cr:YSGG laser alone is not a predictable tool for removing the smear layer and debris from the apical third of root canals. According to previous studies, 5,22 a combination of laser irradiation and a chelating agent may help to obtain cleaner root canal walls in the apical third of root canals.
Conclusions
Based on the results of the present study, root canal treatment with an Er,Cr:YSGG laser at 1.5 W output power showed a similar degree of effectiveness in smear layer removal to that of conventional treatment with EDTA and NaOCl irrigation. Conversely, the application of the Er,Cr:YSGG laser failed to remove debris from the root canal walls as compared with the more traditional EDTA and NaOCl irrigation technique.
Footnotes
Acknowledgments
This project was funded by grant #15778 from the Tehran University of Medical Sciences and Health Services. The authors acknowledge the technical support of the staff of the Laser Research Center of Dentistry, Tehran University of Medical Sciences, Tehran, Iran, and thank Dr. Javad Kharrazifard for his assistance with the statistical analysis of this research, and Dr. Arabella Christian from the Post-Graduate Endodontic Department, School of Dentistry, University of Maryland in Baltimore, for her English revision of this article.
Author Disclosure Statement
No competing financial interests exist.