
Abstract
Introduction
R
Irrigant agitation techniques have been introduced to enhance the dispersal of irrigants throughout the canal system, thus increasing their cleaning ability. 4 Passive ultrasonic irrigation (PUI) is based on inducing acoustic microstreaming and cavitations in the intracanal irrigant, 5 which may enhance the removal of the intracanal smear layer 6,7 and endodontic biofilms. 8 RinsEndo®, which uses pressure suction technology to deliver the irrigant solution in the root canal, activates it automatically (1.5 Hz). It improves the penetration of an irrigant in dentine, 9 the removal of the smear layer, 10 and reduction of bacteria. 11 However, the superiority of the PUI and RinsEndo over conventional syringe irrigation is still not confirmed. 8,12,13
Another way to activate irrigant solutions in root canals is the use of lasers, especially Erbium lasers. 14,15 Laser-activated irrigation (LAI) 15 is based on the strong absorption of the Erbium laser energy in water, which results in its vaporization, and formation of large elliptical vapor bubbles. During oscillation of the vapor bubbles, high intracanal pressure drives fluid out of the canal. When the bubbles implode, an underpressure develops and sucks fluid back into the canal, inducing a secondary cavitation effect. 15 LAI improves the removal of intracanal debris and the smear layer. 16 Regarding antimicrobial efficacy, LAI compared with syringe irrigation yielded contradictory results, 17,18 and there are only a few studies published so far on comparison with other agitation irrigation techniques. 19,20
The purpose of this laboratory study was to compare the antimicrobial efficacy of Erbium, chromium: yttrium, scandium, gallium, garnet (Er,Cr:YSGG) LAI, PUI, the RinsEndo system, and syringe irrigation against intracanal Enterococcus faecalis.
Materials and Methods
Specimen preparation
The study protocol was approved by the Ethics Committee of the School of Dental Medicine, University of Zagreb. The study sample consisted of 100 extracted human mandibular incisors and maxillary second premolars. All teeth had completely developed roots, and were without root caries or previous endodontic treatment. The presence of a single canal was determined by radiographs (Gendex, KaVo, Biberach, Germany) taken in mesiodistal and buccolingual directions.
After extraction, the teeth were stored in 0.5% chloramine-T solution at 4°C until use. Teeth were decoronated with a water-cooled diamond fissure bur number 016 (Komet, Rock Hill, SC) to obtain the working length (WL) of a residual root of 12 mm. Teeth with apical foramen that could be easily passed with a 20 K-file (Dentsply Maillefer, Ballaigues, Switzerland), or could not be initially passed with an 08 K-file, were not included in the study. The root canals were instrumented with the conventional sequence of rotary ProTaper Universal instruments (Dentsply Maillefer) to final F3 instrument [master apical file (MAF)]. After each instrument was used, the root canals were irrigated with 1 mL of 2.5% NaOCl using a syringe and 30 gauge needle (BD Microlance, Becton Dickinson, Madrid, Spain
Root canal contamination with E. faecalis
A suspension was prepared by mixing a pure culture of E. faecalis ATCC 29212, grown in blood agar plates containing 7% horse blood for 24 h, with 2 mL of sterile 0.85% saline solution. The density of 0.5 McFarland was measured by the densitometer (Densimat, BioMérieux, Marcy l'Etoile, France).
Each root canal was filled with 10 μL of the bacterial suspension using sterile insulin syringes (BD Plastipak, Becton Dickinson) without overflowing. The suspension was carried to the entire root canal length with a 15 K-file (Dentsply Maillefer). The samples were incubated at 37°C for 10 days in 100% relative humidity. Reinoculation was performed on the 1st, 4th, and 7th days after initial inoculation. After the incubation period, any residual medium was removed with sterile paper points. 21
Four randomly selected samples were stored in 10% buffered formalin and prepared for scanning electron microscopy (SEM) to visualize the pattern of colonization. They were split longitudinally using a diamond fissure bur
Testing procedures
The remaining 90 samples were randomly divided into four experimental groups (n=20/each) and a positive control group (n=10).
In group I, the 2.5% NaOCl was activated by the Er,Cr:YSGG laser (Waterlase, Biolase, San Clemente, CA) using an endodontic radial firing tip with diameter 275 μm and length 25 mm (Endolase Tip RFT2, Biolase) for 5 sec, repeated four times in a row. Physical parameters of the laser were: λ=2780 nm; power, 1.25 W; pulse repetition rate, 20 Hz; pulse energy, 62.5 mJ. The fiber was marked at 7 mm with a black marker in order to position it 5 mm short of the WL. 22 A total of 5 mL NaOCl was used.
In group II, 2.5% NaOCl (10 mL) was continuously pumped during 60 sec of PUI (Piezon Master 400, EMS, Nyon, Switzerland), set at medium power. A stainless steel 15 K-type file (Endosonore, Maillefer, Ballaigues, Switzerland), was placed at 2 mm short of the WL.
In group III, 2.5% NaOCl was delivered and agitated by the RinsEndo (Dürr Dental GmbH & Co., Bietigheim-Bissingen, Germany) system during 60 sec at a manufacturer's set rate of 6.2 mL min−1. The system was charged with a 20 mL syringe and cannula (ø: 0.45×12 mm), which was placed in the coronal third of the root canal.
In group IV, the root canals were irrigated with 5 mL 2.5% NaOCl for 60 sec using a 5 mL syringe and a 30 gauge needle (Becton Dickinson, Madrid, Spain
The samples in the positive control group were rinsed with 5 mL of sterile 0.85% saline solution, using a syringe and 30 gauge needle, which was placed 2 mm short of the WL for 60 sec.
After each protocol, the root canals were rinsed with 1 mL of 5% sodium thiosulfate for 30 sec, to neutralize the remaining NaOCl, and with 1 mL of sterile saline for 30 sec, to standardize all experimental treatments to the same number of rinsing procedures. 23
Sampling procedures
The root canals were sampled before and after each disinfection protocol. The canals were filled with 10 μL sterile 0.85% saline solution. After three aspiration-delivering cycles with a sterile insulin syringe, the canal content was aspirated and transferred to the first 0.5 mL Eppendorf tube, containing 90 μL sterile saline. During the sampling procedure, the teeth were held upside down to collect all the sampling fluid. After 10-fold serial dilutions and agitation in vortex for 1 min, aliquots of 10 μL were plated onto blood agar plates (211037, Becton Dickinson, NJ), and incubated for 48 h at 37°C in 100% humidity. Colony-forming units (CFUs) grown were counted and transformed into actual counts based on the dilution factor. Before the second sample was taken, a size 30 Hedström file (Dentsply Maillefer) was used to vigorously file the dentinal walls. 24
Polymerase chain reaction (PCR) analysis
All samples were examined by PCR. The suspension was heated at 95°C for 15 min and centrifuged for 1 min. Standard isolate of E. faecalis (ATCC 29212) was used as a positive control. The reaction mixture was composed of 1.0 PCR buffer, 2.0 mM MgCl2, 0.2 mM deoxynucleotide triphosphate (dNTP) (Fermentas, Vilnijus, Lithuania), six primers (each 0.5 μM), and two units of recombinant Taq DNA polimerase (Cinnagan Inc, Tehran, Iran). Primer sequences were designed based on the whole E. faecalis V583 genome: E16F (AGAGTTTGATCCTGGCTCA) and E16R (GGTTACCTTGTTACGACTTC); product 1522 bp; EfisF (ATGCCGACATTGAAAGAAAAAATT) and EfisR (TCAATCTTTGGTTCCATCTCT); product 803 bp; EfesF (GTGTTAAAACCATTAGGCGAT) and EfgsR (AAGCCTTCACGAACAATGG); product 650 bp.
Gel electrophoresis reaction was performed on 1% agarose gel (Cinnagen, Tehern, Iran). Samples that contained E. faecalis DNA, showed positive amplification of 1522, 803, 650 pairs base.
Statistical methods
The Mann–Whitney U test was used for intragroup analyses. The Kruskal–Wallis test was used for the intergroup comparative analysis of data of second samples. The significance level was set at 5%. Analyses were performed by using SPSS 11. 0 (Chicago, IL).
Results
There was a significant reduction in the number of CFUs after every treatment protocol (p<0.001). Table 1 and Fig. 1 present the distribution of the results (mean, median, range, reduction rate) before and after the treatment protocols. All three dynamic irrigation techniques were equally effective in reducing E. faecalis population (p>0.05), and superior to the conventional syringe/needle irrigation and positive control (p<0.001), between which there was no difference (p=0.795). According to the results of both the culture method and the PCR, after PUI and RinsEndo six samples were sterile, and after LAI nine samples were.
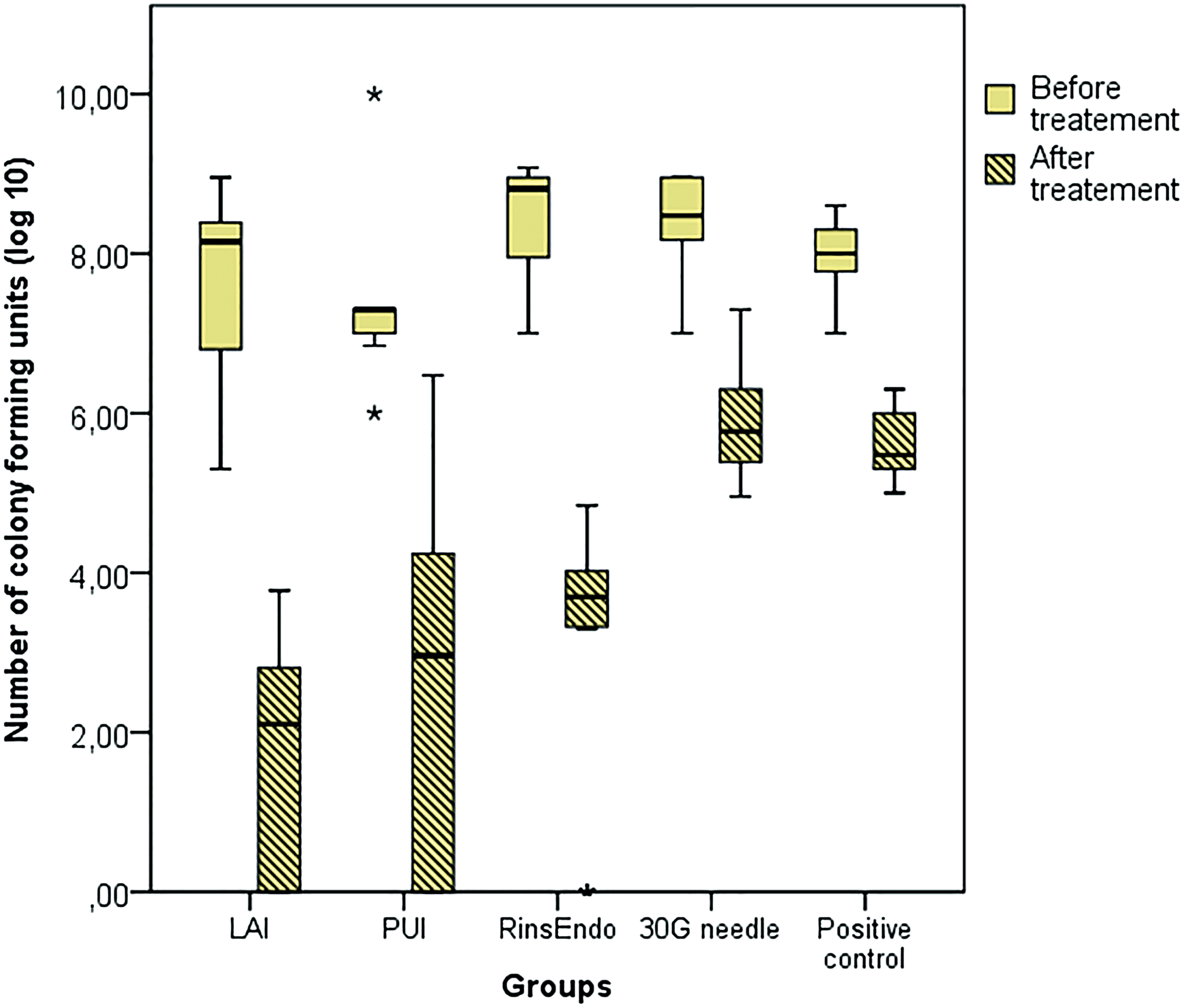
Distribution of counts of Enterococcus faecalis colony-forming units (CFUs) before and after the disinfection protocols.
CFUs, colony-forming units; LAI, laser-activated irrigation; PUI, passive ultrasonic irrigation.
Discussion
Although the effectiveness of LAI in root canal debridement has already been shown in many previous research studies, 25,26 there are only a few, so far, published on its antimicrobial efficacy, and most of them evaluated the activity of the Er:YAG laser. 17 –20 To the best of our knowledge, this is the first study that compared the efficacy of Er,Cr:YSGG LAI, PUI, the RinsEndo system, and syringe irrigation against the intracanal E. faecalis population.
The time taken for E. faecalis colonization or biofilm formation in the root canals varies among studies. 27 In some of them, a model of E. faecalis, incubated for a few hours, was used, 28 and in the others, one day of the incubation time was claimed to be sufficient for the biofilm formation. 24,29 However, a longer incubaton time for the bacteria presents a more mature and clinically relevant biofilm, which is why it is increasingly used in recent studies. 17,19,20 We used E. faecalis incubated in the root canal for 10 days, 23 and the pattern of colonization was confirmed by SEM. The first microbial evaluation method was culturing and counting CFUs, which is commonly used in studies on root canal disinfection. 17,23 However, because of the low sensitivity of the culturing, all samples were additionally tested by the PCR method in order to exclude false negative results in samples with a very low number of the bacteria that could not be cultivated. 30
The results of the study did not show any difference in the reduction rate of the bacteria between the active irrigation techniques, which were more effective than the syringe irrigation. Moreover, they were all able to eradicate the bacteria in few samples. These results are consistent with most previous studies, which proved the importance of hydrodynamic phenomena in root canal disinfection. 4,5,7 –9,28 Cachovan et al. 13 also reported better results after PUI than syringe irrigation. Although Bhuva et al. 12 and Siqueira at al. 30 did not observe this difference, numerous studies have concluded that PUI has better cleaning properties in the terms of the removal of debris, tissues, and the smear layer, than the conventional irrigation. 31
Different from our results, Cachovan et al. 13 found a higher reduction rate after PUI (20 sec) than after RinsEndo (1 min), using 5 mL 1.5% NaOCl. It can be assumed that the higher concentration of NaOCl (2.5%) and the same action time as was used in this study, despite the large difference in the total volume of NaOCl delivered during PUI (10 mL) and RinsEndo (6.2 mL), caused equal efficacy of the techniques. Moreover, it has been suggested that, when using agitation systems, there could be a point of saturation above which the increase in the volume of the NaOCl beyond a certain threshold will not improve the distribution of the irrigant and its efficacy. 23
Another possible reason for the equal antimicrobial efficacy of the active techniques in this study could be the simple morphology of straight canals and large apical instrumentation, which probably increased the NaOCl reaction kinetics equally. 32,33 This is particularly important for the performance of PUI, in which the contact between an ultrasonic tip and the dentinal wall may result in diminished amplitude and the reduction of irrigant's streaming velocity. 34 In the present study, the ultrasonic file size 15 was positioned to 2 mm short of the WL, where the diameter of the canal of 0.48 mm allowed its free oscillation. This study, however, does not address the effectiveness of the agitation in the curved canals. Further research is needed to compare the efficacy in complex root canals.
Our results confirm the possibility of the use of LAI in the elimination of intracanal bacterial biofilm instead of conventional irrigation, as has already been reported in few previous studies. 18,19 In the study of Sahar-Helfit et al., 18 the combination of chlorhexidine, EDTA, or saline with Er:YAG laser irradiation removed E. faecalis biofilm from root canal walls more effectively than single irrigation without the laser. Similarly to our results, Peters et al. 20 did not find any difference in the reduction rate between the PUI and LAI (Er:YAG, 50 mJ, 10 Hz) even when using a higher NaOCl concentration (6%) during the same time against older multibacterial biofilm. However, as in our study, LAI resulted in the largest number of sterile samples. It is probable that the energy of erbium laser irradiation could create more powerful hydrodynamic phenomena than the other active techniques in this study. The reason could be the formation of secondary cavitation bubbles as a result of the consecutive short laser pulses. 35 However, the question remains: can LAI achieve the complete elimination of the bacteria in all samples during longer time period? Ordinola-Zapata et al. 19 found better cleaning ability from Er:YAG LAI used at 20 mJ, 15 Hz, and 50 μs pulse duration in combination with 6% NaOCl than from PUI or conventional irrigation. Therefore, additional research is required to determine the laser parameters for the most effective antimicrobial action of LAI.
Conclusions
Under the conditions of this ex vivo study, the tested techniques–LAI, PUI, and RinsEndo—did not show the difference in the reduction rate of E. faecalis, but were more effective than conventional syringe irrigation.
Footnotes
Acknowledgments
This study was performed and financed as part of the research project Experimental and Clinical Endodontology no. 065-0650444-0418, and approved by the Ministry of Science, Education, and Sport of the Republic of Croatia.
Author Disclosure Statement
No competing financial interests exist.