
Abstract
Introduction
T
Some previous in vitro 4 –7 and in vivo 8,9 studies have emphasized the conditioning of root surfaces and reducing the number of microorganisms by means of different methods adjuvant to manual instrumentation. The use of chemical agents showed an effective removal of the smear layer, but could not effectively and completely eliminate the bacteria present on the root surfaces. 10
In addition to these conventional tools, the use of lasers has been reported as an alternative treatment for root surface conditioning. 11 –13 Laser therapy has been considered an effective procedure in the management of periodontal disease because of its ability to debride and to treat dental hard tissues. 14,15 However, laser treatment might cause thermal side effects on the hard tissues, such as morphologic and chemical alterations of the tissues, especially when using some lasers at a high power density and/or in continuous focused mode. 16 –18 The clinical application of lasers in periodontal therapy has continued to expand in the last two decades; however, there are still some controversies about the efficacy. 7,19 –23
The laser types most commonly used in dentistry are: carbon dioxide (CO2); neodymium-doped: yttrium, aluminum and garnet (Nd:YAG), diode laser; erbium-doped: yttrium, aluminum and garnet (Er:YAG) laser; and erbium, chromium:yttrium scandium gallium garnet laser (ErCr:YSGG). 11,13,14,24 In addition to chemical root surface conditioning, the CO2 laser irradiation has been demonstrated to be effective in the removal of the smear layer, 25 and its role in enhancing the attachment of fibroblasts has been suggested when used in vitro at a low power on periodontitis-affected root surfaces. 15 However, the usefulness of CO2 laser irradiation in clinical situation as a conditioning tool is still unexplained, because of poorly understood mechanisms in some in vitro research studies. 26
The Er:YAG laser has been reported to be one of the most promising laser types used for periodontal therapy. 13,24 Some previous reports have demonstrated that Nd:YAG laser irradiation of root surfaces induces the formation of fissures, cracks, and craters, as well as resolidification of the mineralized tissues, 16,17 especially when inadequate irradiation parameters were used. In contrast, the Er:YAG laser has many advantages over the Nd:YAG laser when applied to mineralized tissues, because the Er:YAG is the most resonant among high intensity lasers. This is perhaps because the Er:YAG laser has a high absorption into water; therefore, it acts on the mineralized tissues by vaporizing their water, causing microexplosions and thus mechanical ejection of tissues (ablation). Er:YAG laser irradiation also exerts less thermal effect, that is, it does not produce major side effects on the irradiated tissues, especially when used with air/water coolant, 11,27,28 and it possesses an excellent ability as well as encouraging results for ablating calculus deposits. 14
Furthermore, some studies have reported a high bactericidal effect of high intensity lasers on periodontal pathogenic bacteria. 29 –31 This is perhaps because the laser irradiation may promote water vaporization inside the cytoplasm of bacterial cells, leading to cell rupture, 32 or may directly melt or coagulate the bacterial cells. 33
Regarding the biological compatibility of the Er:YAG lased root surface, most of the previous studies demonstrated increased cell attachment on the periodontally affected roots following the Er:YAG laser debridement alone, compared with conventional scaling and root planning (SRP); however, the effect of Er:YAG laser as a root conditioning tool following SRP has not been evaluated in detail in comparison with the CO2 laser.
The aim of the present study was to evaluate and compare effects of CO2 or Er:YAG laser irradiation for conditioning periodontally diseased root surfaces following SRP. This study attempted to assess the morphologic changes of the lased root surfaces and to evaluate the attachment of periodontal ligament (PDL) cells on the surfaces.
Materials and Methods
Experimental specimens and surface areas
Forty-five periodontally diseased single-rooted teeth were extracted with a hopeless prognosis, because of advanced periodontitis, from patients attending the Department of Oral Medicine, Periodontology & Oral Diagnosis, Faculty of Oral & Dental Medicine, Fayoum University, Al-Fayoum, Egypt. In addition, five fresh healthy teeth extracted because of either impaction or orthodontic reasons were obtained from the Department of Oral Surgery for the collection of PDL cells. The study protocol was approved by the university ethical committee and written informed consent was obtained from all the patients prior to tooth extraction. The experimental areas in the periodontally affected surfaces were cut from the roots of extracted teeth with a size of 4×4 mm and a thickness of 2 mm, and 45 root specimens were prepared.
Experimental groups and group subdivisions
The 45 specimens were randomly assigned into the following three groups: Group I: Control (untreated diseased) Group II: SRP+CO2 laser treatment; the irradiation was performed in a repetitive pulsed mode (2 Hz), using a 0.8 mm tip at 4 mm distance from the target (spot size 0.9 mm in diameter), with a power setting of 2 W, that is, equivalent to an energy density of 2.7 J/cm2. Group III: SRP+Er:YAG laser treatment; the irradiation was performed in a slight contact mode, using a 0.6 mm tip, at 40 mJ/pulse (14.2 J/cm2 per pulse at the tip end) and 10 Hz, under air/water spray.
Five specimens per each group (15 specimens in total) were used for root surface topographic examination, whereas the remaining 10 specimens per each group (30 specimens in total) were used for evaluating PDL cell attachment.
Ultrasonic scaling and laser application
The selected root surface specimens in groups II and III were scaled thoroughly with an ultrasonic scaler, with a mean treatment time of 35 sec. Then, either the CO2 laser (Luxar LX-20 Dental Laser™, Panasonic, Tokyo, Japan) or the Er:YAG laser (Erwin™, Morita, Tokyo, Japan) was applied to the root surfaces in parallel paths with three directions as follows: horizontally, from coronal to apical; vertically, from buccal to lingual; and obliquely, across these directions. This overlapping laser application technique was employed to secure complete lasing of the whole specimen's surface. The mean irradiation time was 51 sec for the CO2 laser and 45 sec for the Er:YAG laser.
PDL cell attachment assay
Cells were counted using a transmission light microscope and a counting grid. A concentration of 5×103/20 μL per each sample of PDL cells was pooled on the surfaces of the specimens in the whole groups. The incubation time periods for the cultures were set for either 1 or 2 weeks, at 37°C, in an atmosphere of 95% humidified air and 5% CO2.
The specimens were then processed and prepared for scanning electron microscopy (SEM) (S-4500 SEM, Hitachi Ltd., Hitachinaka, Japan) to evaluate PDL cell attachment. Five SEM photomicrographs per each sample, four at the four extremities sides and one in the center, were taken at the magnification of ×350 and a working distance of 15 mm. The cell counting of the attached fibroblasts was done within a representative standard area (0.03 mm2), three times blindly per each photomicrograph.
PDL cell quality was divided into three categories depending upon the shapes or forms as follows: flat, for a healthy one; oval, as an intermediate form; and round, as a diseased one. Also, the cell quantity was evaluated as follows: negative, empty areas without cells; light, separately dispersed cells with wide spaces; intermediate, interlaced cells forming a network with narrow spaces; and heavy, overlapped and multilayered cells without spaces. The cell density of each group was determined by scanning the whole specimen's surface through obtaining nine SEM images per each specimen, three images in each of the upper, middle, and lower thirds at low magnification (×50). This was done according to a method previously reported by Belal et al. 34
Statistical analysis
The statistical analysis of the obtained results was conducted using statistical software (SPSS version 10; SPSS Inc., Chicago, IL). After a one way ANOVA test was applied, the intergroup comparison was performed using a post-hoc Scheffe test, whereas the comparison within each group, between the used time periods, was analyzed by using a paired t test. Results were considered statistically significant at p≤0.05.
Results
Root surface topography
The specimens exhibited different characteristic features among the experimental groups (Fig. 1). The original diseased surfaces of the untreated control group generally showed an irregular rough feature (Fig. 1A). The CO2 laser group showed multiple areas affected by surface charring and microcracking (Fig. 1B). The Er:YAG laser group showed also a few areas affected with charring layers (Fig. 1C), but other main areas showed irregular surfaces with multiple projections, and opening of the dentinal tubules distributed throughout the irradiated surfaces (Fig. 1D). The latter feature was more pronounced in the Er:YAG lased specimens with more wider and funnel-shaped openings than the CO2 laser group.
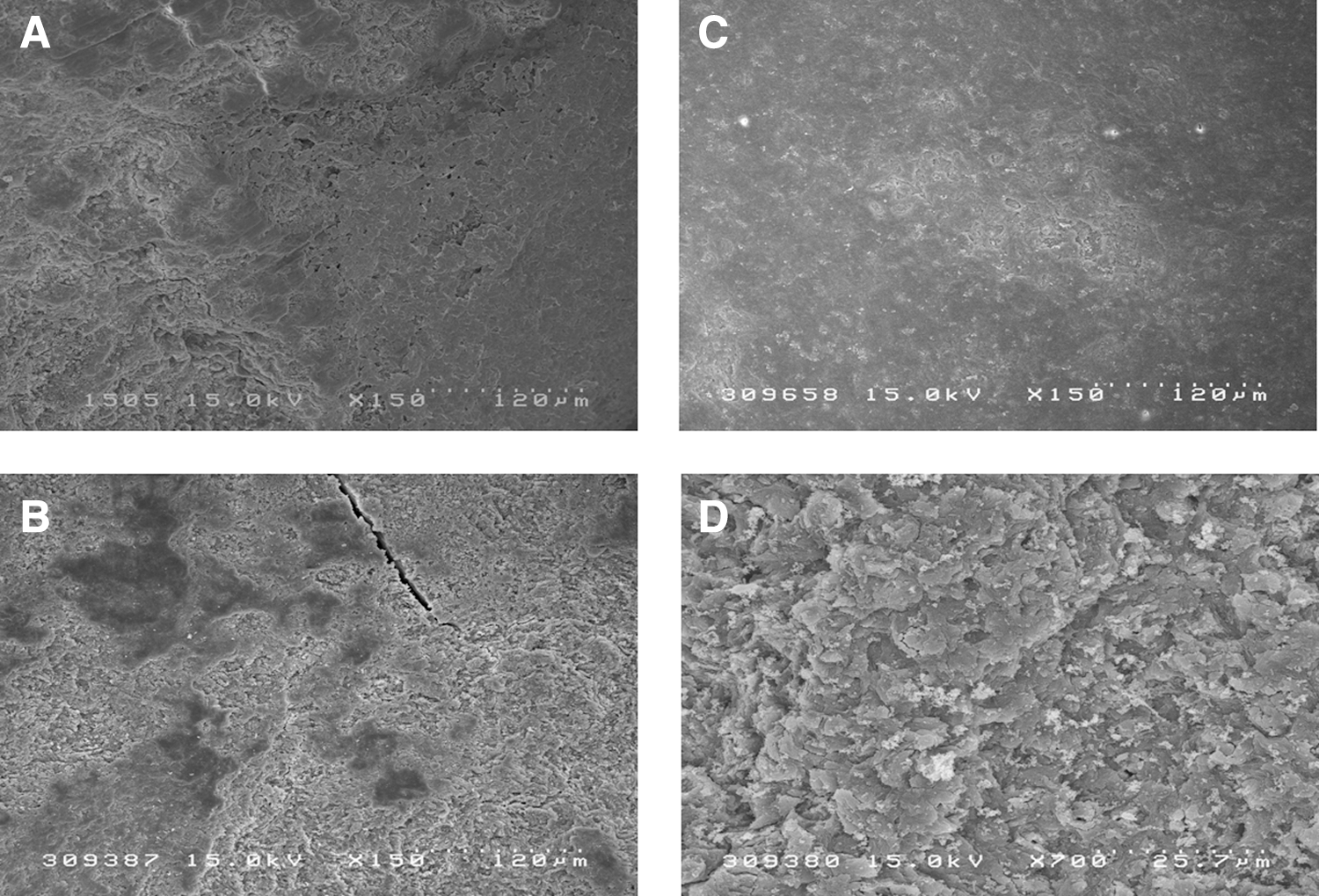
Scanning electron microscopic (SEM) photomicrographs of root surface topographic features following laser conditioning.
PDL cell attachment
The control group
This group was generally devoid of any PDL cell attachment except for the presence of some isolated dispersed cells in certain narrow areas (Fig. 2A).
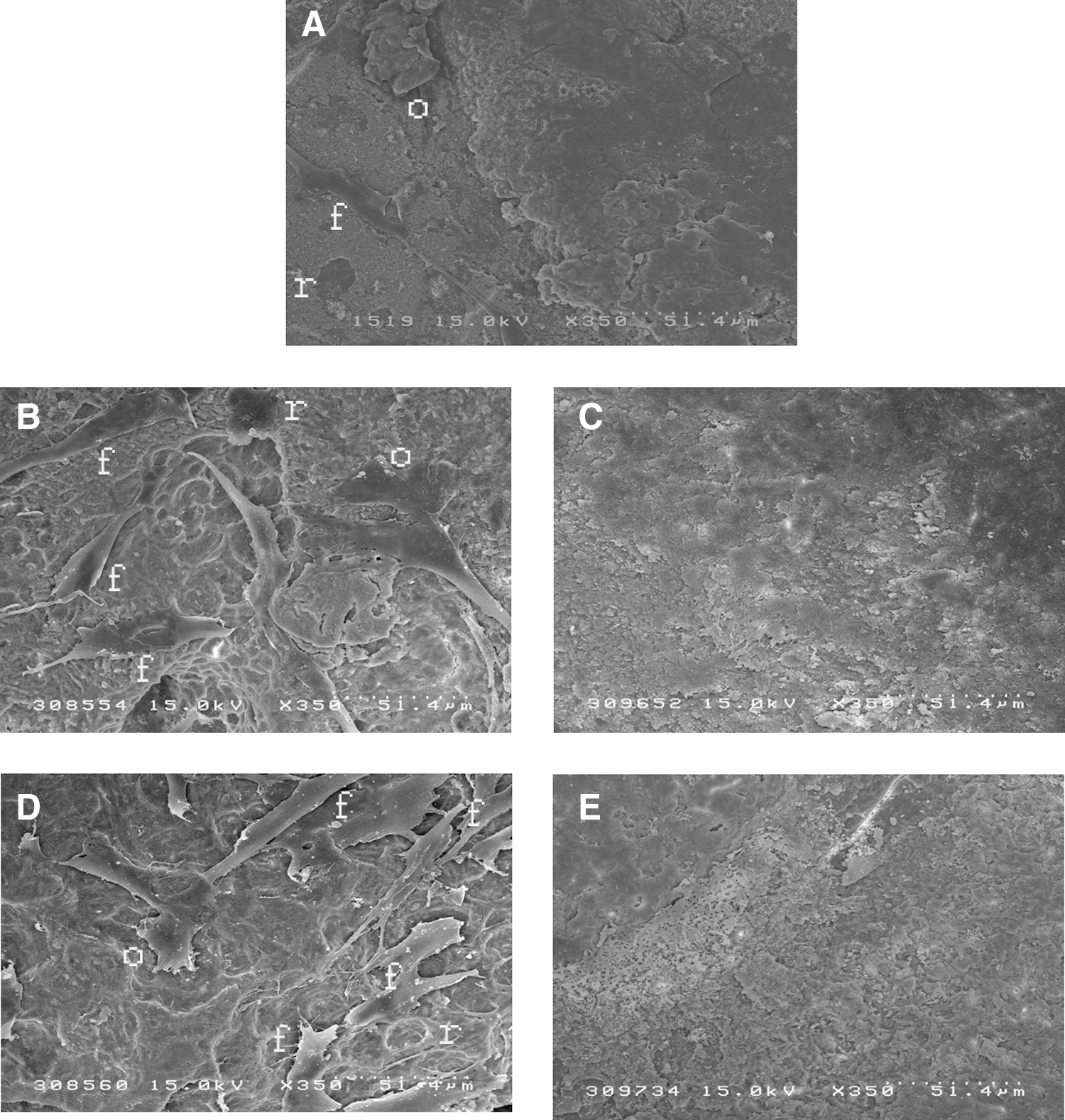
Scanning electron microscopic (SEM) photomicrographs of root surfaces following laser conditioning and periodontal ligament (PDL) cell incubation.
The CO2 laser group
In this group, some specimens exhibited the presence of the evidently flat elongated fibroblast cells that were well attached to the root surface and had smooth cell surfaces as well as long anastomosing cytoplasmic processes (Fig. 2B). Also, some specimens showed the root surfaces without PDL cell attachment (Fig. 2C) and instead, certain characteristic features such as evident charring layers and slight depression areas were detected.
The Er:YAG laser group
The Er:YAG laser group showed more positive results than did the CO2 laser group, regarding the attached cells. The root surfaces in these specimens were almost completely covered by confluent overlapped layers of flat healthy cells having smooth surfaces and forming an anastomosing network as well as a matted appearance (Fig. 2D). However, some specimens showed negative results (Fig. 2E) of some isolated cells that appeared in the irregular root surface.
Furthermore, a few numbers of dispersed round and oval cells were detected at certain areas of both CO2 and Er:YAG lased specimens (Fig. 2B and D).
PDL cell density
The control specimens showed the lowest mean values of periodontal ligament cells, with no tightly attached cells, mostly in oval shape. The CO2 lased specimens showed a significant increase in mean values of attached cells compared with the controls. The Er:YAG lased specimens showed the highest mean values of attached cells, mostly in flat form (Table 1, Fig. 3).
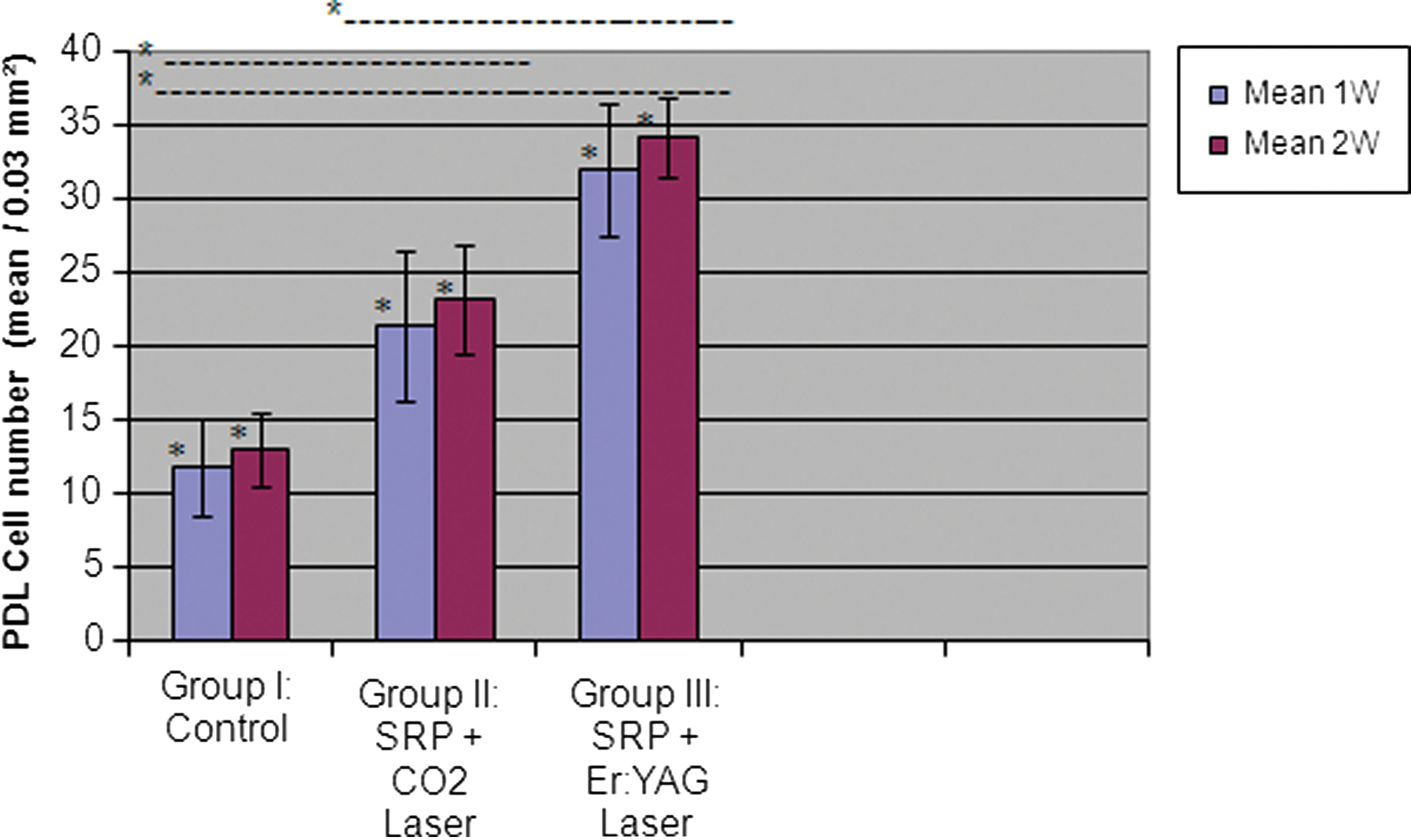
Histogram of the mean value of cell numbers on the treated root surfaces at 1- and 2-week incubation periods. *p≤0.05.
Significant; NSnot significant.
SRP, scaling and root planning.
The intergroup differences in the number of attached cells showed a statistically significant difference noticed for both the CO2 and Er:YAG laser groups over the control group and more specifically for the Er:YAG laser group over the CO2 laser group (p≤0.05) (Table 1). On the other hand, the comparison within each group between 1- and 2-week incubation periods did not show any statistically significant difference.
Regarding the evaluation of the attached cell shape at the 2-week incubation period, the Er:YAG and CO2 laser groups showed the highest ratio of flat PDL cells and the lowest ratio of both oval and round cells compared with controls (Fig. 4). In addition, there were no significant differences observed either among the two laser groups at the two incubation time periods using the ANOVA test, or within each experimental group using the paired t test (Table 2).
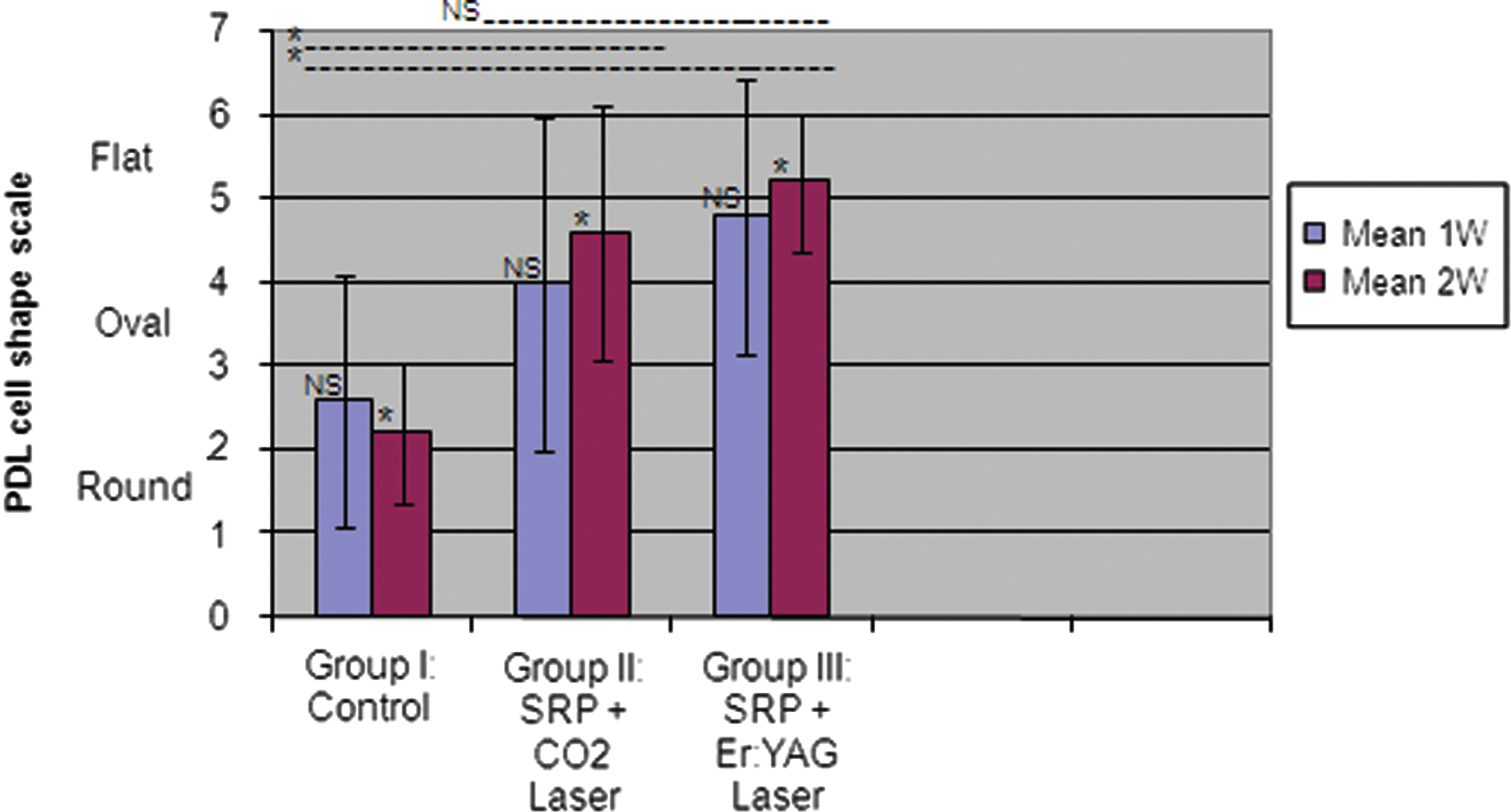
Histogram of mean value of cell shape on the treated root surfaces at 1- and 2-week incubation periods. *p≤0.05; NS, not significant.
Significant; NSnot significant.
SRP, scaling and root planning.
Discussion
The obtained results in the present study showed an evident difference in the root surface features among specimens irradiated with CO2 and Er:YAG lasers (Fig. 1B–D, and Fig. 2C and E, respectively). This may be explained by the occurrence of different tissue interactions resulting from the different wavelengths of these lasers. In accordance, some previous reports 35 –37 stated that the mechanisms of hard tissue interaction produced by CO2 and Er:YAG lasers have been classified as photothermal vaporization and mechanical ablation, respectively. Sasaki et. al. 38,39 and Almehdi et al. 40 suggested that CO2 laser irradiation shows mainly thermal effects on dentin and cementum, whereas Er:YAG laser removes these root surface structures by thermomechanical or photomechanical ablation, with minimal thermal effects.
The untreated specimens of the control group of the present study showed only an occasional attachment of isolated PDL fibroblasts at certain areas on some specimens (Fig. 2A), and this is perhaps because of the presence of contamination and toxic substances such as lipopolysaccharides (LPS), as well as a prominent loosely textured debris layer on the affected root surfaces. 15,41 The use of SRP+CO2 laser irradiation in the present study resulted in a significant improvement of cell density and differentiation from the controls (Table 1, Figs. 2B, 3, and 4); however, the results were lower than those of the SRP+Er:YAG laser irradiation.
The lesser performance of the CO2 laser irradiation in the present study when compared with Er:YAG laser was probably the result of the pronounced presence of root surface charring layers with surface cracking as well as pitting and depression areas of the treated specimens (Figs. 1B and 2C) that may suggest the production of a thermal response more than which occurred in the Er:YAG lased specimens (Figs. 1C and D, and 2E). An irregular root surface texture and rough topography in some specimens with a globular and porous appearance are also perhaps explanations for such poor results.
These findings can be supported by results of some previous studies, 25,42 because Morlock et. al. 42 suggested similar findings such as random distribution of pits and crater formation as well as melting of the mineral phase, and resolidification as porous globules following Nd:YAG laser irradiation at low energy levels with an extended time period. In addition, Misra et al. 25 used CO2 laser irradiation and reported charring in the specimens with an increased exposure time under a constant energy level of 3 W and a constant 5 cm distance. These findings can suggest the presence of some important factors that may influence the output of laser irradiation therapy, and can even determine the degree of charring and carbonization occurring on the root surfaces. These factors are: the distance between specimen surface and laser point, the laser penetration power, the exposure time of the used laser, and the pathological condition of the tooth. However, the present trial determined the used laser parameters according to a previous pilot study.
The SRP+Er:YAG lased specimens showed the most efficient and significant results in the present study regarding cell density and differentiation (Table 1, Figs. 3 and 4), because confluent monolayers of healthy well-differentiated flat attached cells were formed on the treated surfaces (Fig. 2D). Perhaps this is can be explained by an evident removal of the smear layer produced after SRP and opening of the dentinal tubules (Figs. 1D and 2E). This can be supported by our previous positive findings 43 upon using Er:YAG laser irradiation alone or combined with Recombinant human platelet-derived growth factor BB (rhPDGF-BB) on periodontitis roots, but without using SRP. Other explanations may be because of the occurrence of decontamination 33 and detoxification 44 as well as exposure of the underlying collagenous matrix, that makes the surface more biocompatible and attractive to PDL fibroblasts. Furthermore, Pant et al. 26 postulated that these effects may be explained as a direct consequence of root surface biomodification, through which some of the extracellular matrix components acting on the attachment mechanism of PDL cells became more exposed.
In addition, the water irrigation that is used with the Er:YAG laser irradiation may be effective in reducing the thermal effects and cleaning the irradiated surface. Previously, Visuri et al. 45 recommended the use of water during Er:YAG laser irradiation to prevent high thermal generation, and Sasaki et. al. 38 detected the slight formation of byproducts on the dental surfaces upon using Er:YAG laser irradiation without coolant. In general, the Er:YAG laser irradiation in the present study showed irregular surface with multiple projections and occasional opening of the dentinal tubules. However, some large particles were observed at certain areas, which may suggest a temporary and momentary temperature increase at such areas. This thermal effect was not as high as that noticed in CO2 lased specimens. On the other hand, the idea of using water coolant with CO2 laser irradiation in the present study was not advisable, because Sasaki et. al. 39 demonstrated in a previous pilot study, during the initial stages of the research, that CO2 laser ablation had an impaired performance when water was applied.
In the present study, another control group of SRP only was not included because of the limited number of samples; however, in the previous several studies, 46,47 the better or favorable results in the cell attachment to the surface treated with Er:YAG laser compared with the SRP-treated surface have been demonstrated, and the advantageous positive effect of Er:YAG laser treatment has already been clarified. Meanwhile, the cause of the better result of SRP+Er:YAG laser irradiation over the untreated control in the present trial was considered the synergic effect of each therapy.
Further studies using a large sample size and different laser settings may be necessary to determine the ideal parameters for achieving a more compatible root surface condition needed for a maximum regenerative healing capacity during periodontal therapy. In addition, biochemical experiments would need to be added for differentiation from other previous studies. Finally, periodontal clinical studies are necessary before any firm conclusions can be reached.
Conclusions
The results of the present study can conclude finally that (1) both CO2 and Er:YAG laser can significantly stimulate periodontal ligament cell attachment, but CO2 laser has some deleterious effects on root surfaces; and (2) Er:YAG laser may constitute a useful conditioning significant tool to enhance periodontal ligament cell attachment to periodontitis-affected root surfaces without notable undesirable effects.
Footnotes
Acknowledgments
The authors are grateful to Abdulaziz Yassin, Prof., Department of Public Health & Community Medicine, Faculty of Medicine, Tanta University, Tanta, Egypt; Community Medicine Consultant, MOH, Saudi Arabia, for his help with the statistical analysis, and both Prof. Mohamed B. Khidr and Prof. Aly E. Shehata from the Department of Oral & Maxillofacial Surgery, Faculty of Oral & Dental Medicine, Fayoum University, Al-Fayoum, Egypt, for their kind support of this study.
Author Disclosure Statement
No competing financial interests exist.