
Abstract
Introduction
T
First, it acts on the early stages of inflammation 8 through reduction of prostaglandin E2 (PGE2) concentrations and through inhibition of cyclo-oxygenase 2 in cell cultures. 7,12 –14 The second effect is a modulation of fibroblast metabolism and collagen deposition, that starts earlier because of the anti-inflammatory effect. Observed histological changes in tendons receiving LLLT include increased collagen production, 15 improved collagen bundle organization, 16,17 and an increased number of small blood vessels. 9,18 The collagenase-induced tendinitis model is suitable for studying the sequence of acute inflammatory responses in tendon tissue, 7 and animal models are commonly used in tendon disorder research. 19 Numerous authors describe the positive effect of the LLLT in experimental trials in rats, 15,16,19 –21 , mice, 22 or rabbits, 12 but to our knowledge, there are no studies investigating the effect of LLLT on experimentally induced tendinitis in sheep. The sheep is the most widely used experimental model for the study of human and equine musculoskeletal disorders and is recognised as a model of human and equine orthopedic disease, including tendinopathy. 23 –25 The present pilot study was designed to investigate the effect of Multiwave Locked System (MLS®) laser therapy on an experimental model of collagenase-induced tendinitis in sheep, in order to evaluate an adaptable treatment for human and animal athletes, and it is the first animal model study in which MLS laser therapy was used on sheep. MLS laser therapy is an innovative LLLT that features the MLS laser pulse. This is a patented pulse with combined, synchronized, and overlapping continuous and pulsed emissions, with wavelengths of 808 and 905 nm, emitted by a single handpiece.
Materials and Methods
Animals
Six healthy adult Bergamasca female sheep weighing 50–60 kg were used. The integrity of tendons was assessed by clinical and ultrasound examination prior to the experimental study. This preliminary study was approved by University Ethics Committee for Animal Experimentation (CEASA) and by the Italian Ministry of Health on May 17, 2010 (DM no. 97/2010-B).
Induction of tendon lesions by collagenase injection
The defect was realized as previously described in the hindlimbs 25,26 using the deep digital flexor tendon (DDFT). Sheep were sedated with 10 μg/kg of medetomidine (Sedator®, Ati srl Ozzano dell'Emilia, Italy) intravenous administration into the auricular vein, anaesthetized using 2 mg/kg of propofol (Rapinovet® Intervet Italia, Peschiera Borromeo, Italy), and positioned in lateral recumbency. After aseptic disinfection, in each sheep, 500 IU of sterilized bacterial collagenase type 1A (C-9891; Sigma, Milan, Italy) in 0.13 mL of saline solution was injected bilaterally (left and right hindlimbs) into the DDFT under ultrasonographic guidance. The injection was performed using a 23 gauge needle positioned 15 cm in the proximal–distal direction from the calcaneal bone. The needle was inserted into the thickness of the DDFT with a lateral approach, with the hock joint flexed at 90 degrees. A suture was applied near the injection point, in order to mark the precise point for treatment and tendon harvesting (Fig. 1). Perioperative antibiotic therapy with amoxicillin-clavulanic acid (Synulox® Pfizer Italia, Rome, Italy) 12.5 mg/kg subcutaneously (SC) was started and continued for 5 consecutive days. Analgesia was provided by administration of 0.01 intramuscular (IM) mg/kg of buprenorphine (Temgesic® RB Pharmaceuticals, Slough, UK) BID for 5 days.
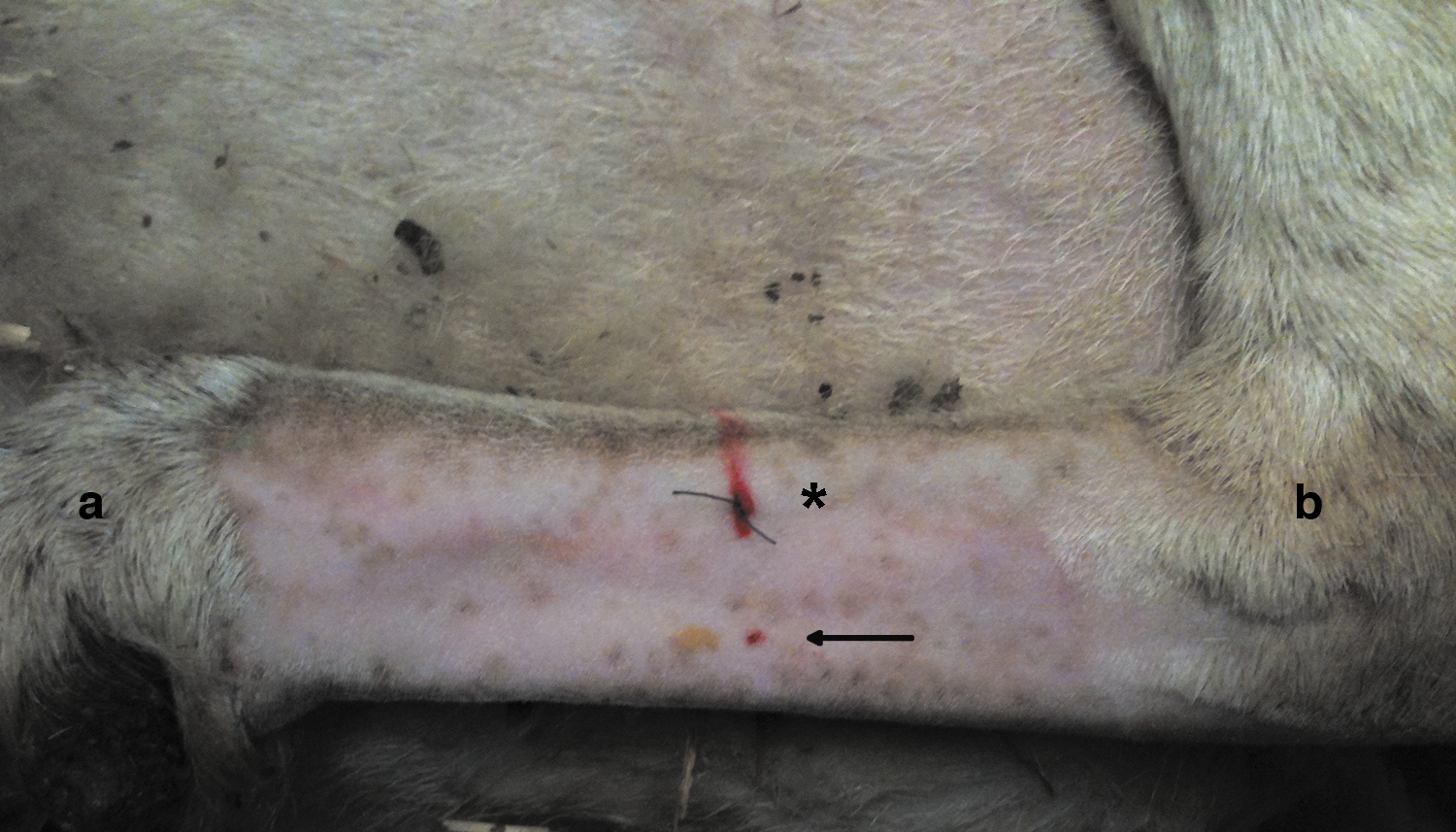
Macroscopic aspect of the limb. A suture (asterisk) is applied to each lesioned limb near the injection point (black arrow), in order to mark the precise point for treatment and tendon harvesting (a=metatarsophalangeal joint, b=hock joint).
MLS laser treatment
MLS laser therapy was performed using a Mphi vet laser device (ASA, Arcugnano-VI, Italy), equipped with combined, synchronized and overlapping continuous and pulsed emissions emitted by a single handpiece. Continuous emission or continuous interrupted emission was produced by an InGa(Al)As diode laser with the following parameters: wavelength 808 nm, peak power 1000 mW continuous wave, mean power 500 mW continuous interrupted wave, spot area 3.14 cm2, spot diameter 2 cm. Pulsed emission was produced by an InGaAs/GaAs diode with the following parameters: wavelength 905 nm, peak power 25 W, mean power 54 mW at 1500 Hz, pulsed wave, spot area 3.14 cm2, spot diameter 2 cm. The two propagation axes are coincident.
The six sheep, divided into two groups, were treated 7 days after collagenase injection. MLS laser therapy applications were performed, by the same operator, daily for 5 days, interrupted for 2 days and then continued for another 5 consecutive days, mimicking the therapy protocol reported by Bjordal and Lopes-Martins. 27 In order to administer the energy as evenly as possible with the Mphi vet laser device, considering the size and the shape of the treatment area, the scan modality was chosen.
This modality has been already described by other studies, 28 –34 and it is performed by moving the handpiece slowly and evenly over the treatment area following a grid pattern for an established treatment time. The reflection of the laser emission is reduced as a result of the special conformation of the handpiece head, which can be placed directly in contact with the skin. Furthermore, the equipment was calibrated before the start of every study. The calibration was done using the Powermeter Ophir Nova II Display S/N 573995. To increase the reliability of the data collected, the experimental design involves the use of an internal control for each animal: one of the two hindlimbs was subjected to treatment while the other limb was used as a control. The parameters used for the MLS laser therapy for group 1 were: wavelengths 808 and 905 nm, combined and synchronized continuous interrupted wave and pulsed wave, frequency 1500 Hz, duty cycle 50%, power level 100%, maximum power 1000 mW, mean power 554 mW, treatment area 47 cm2, total energy emitted 235 J, treatment times 7 min and 4 sec, and dose 5 J/cm2. In group 1, the left hind DDFT received MLS laser treatment at a dose of 5 J/cm2. The parameters used for the MLS laser therapy for group 2 were: wavelengths 808 and 905 nm, combined and synchronized continuous interrupted wave and pulsed wave, frequency 1500 Hz, duty cycle 50%, power level 50%, maximum power 1000 mW, mean power 304 mW, treatment area 47 cm2, total energy emitted 117.5 J, treatment time 6 min and 26 sec, and dose 2.5 J/cm2.
For both groups, the energy density was calculated using the following formula: total energy (J)/treated area (cm2). In group 2, the left hind DDFT received MLS laser treatment at a dose of 2.5 J/cm2. The right hind DDFT was considered, in both groups, as an internal control (without treatment). At 30 days after the beginning of the treatment (37 days after tendon lesion), the animals were sedated as described previously, anesthetized with 4 mg/kg intravenous (IV) propofol, and euthanized by an IV lethal injection into the auricular vein of 10 mL of a combination of drugs approved for euthanasia (Tanax®, Intervet, Milan, Italy)
Clinical and ultrasound follow-up
All sheep were clinically monitored daily by the same operator, to minimize possible errors or variations. The evaluations were performed always in the same manner, evaluating clinical signs that may be associated with an inflammatory condition, with the circumference of the limb at the point of injury expressed in cm and measured with a tape measure, swelling at the point of injury, the heat of the limb at the point of injury detected manually, with pain on palpation of the limb and degree of lameness having a score ranging from grade 0 to grade 4, as generally utilized in equine medicine. 35 With this grading 0 corresponds to 0, no lameness; 1, lameness is visible while trotting; 2, slight lameness while stepping and marked while trotting; 3, marked lameness while stepping and trotting; and 4, lameness with lack of support of the limb. Tendon thickness and echogenicity of healing structures were evaluated ultrasonographically, following directions, and the findings were reported by Dehghan et al. and Meghoufel et al. 36,37 Ultrasound examinations, obtained using GE Medical System LOGIQ P5 machine and linear probe 6–10 MHz, were performed 1 week after lesion induction (before the beginning of MLS laser therapy), at the end of treatment (21 days after lesion induction), and on the day of euthanasia (37 days after lesion induction).
Histological analysis
After euthanasia, the tendons were surgically removed from the calcaneus to the end of the metatarsal region, and the DDFT of bothhind limbs were harvested for histological analysis, as described by Martinello et al. 38 The removal of tendons was made 5 cm proximally and 5 cm distally to the location of the lesion (previously marked by a cutaneous surgical stitch). Harvested DDFT were cut to 1 cm pieces and the proximal–distal orientations were marked. Tissue samples for histology were fixed in 4% paraformaldehyde (PFA) and embedded in paraffin. Sections were cut at 5 μm, mounted on microscope slides, and stained; Harris's hematoxylin and eosin (HE) was performed. Sections were analyzed for cell density, vascularization (blood vessels areas), and tissue organization; the histological slides were already defined by specific histological markers as fibroblast and vessels numbers, characteristics of fibroblast, and tissue/matrix organization. The whole area of slices obtained from the superficial, central, and deep layer of each tendon was evaluated at the site of injury. In the same slides, in order to compare differences in cell numbers among groups, a quantitative analysis was performed; furthermore, the ratio of the vessel areas was calculated. From each tendon three segments were processed, five slides were taken from each segment, and three microscopic fields were examined per slide; therefore, in total, 540 fields were considered.
Statistical analysis
Digital analysis was performed using the STATISTICA 9 (StaSoft) software, and the results were expressed as the mean±standard error of the blood vessels' total area and number of cells. Data were checked for normality using a Shapiro–Wilk test. Differences among the experimental groups within each sampling were checked using a Kruskal–Wallis Test. In all analyses, a p<0.05 value was accepted as significant.
Results
Clinical evaluation and follow-up
After collagenase 1A injection, all sheep showed an inflammatory reaction with a mild localized thickening of DDFT and an increase, in the lesion point, of a few millimeters in limb circumference compared with the starting value (Table 1). Pain detected by palpation remained evident for the first 3–5 days as well as lameness, which ranged from grade 3 to grade 4; a local increase in temperature was detected manually for the first 3 days. Starting from day 7, a mild inflammatory reaction was observed in treated limbs of group 1 during MLS laser therapy, manifested by an increase of ∼1 cm in circumference (Table 1) and by an increase of local temperature of the metatarsus, whereas no increase of pain or lameness was observed. In group 2, no inflammatory response was observed in the treated limbs during the treatment. In both groups, a progressive reduction in limb circumference (Table 1), local temperature, lameness, and pain was observed after the treatment. In group 2, the limb circumference returned to a value almost comparable with the starting value (Table 1). For each sheep, the treated left DDFT generally showed a more rapid reduction in local inflammation than did the right DDFT, which served as control. The lesions were detectable ultrasonographically in the DDFT 7 days after their creation, and during the follow-up period. All treated limbs showed a more uniform filling of the lesions and collagen fiber alignment than did the control limbs (Figs. 2 and 3). However, the DDFT of the left limb of group 1 showed a major thickening compared with the DDFT of the control limb during the ultrasonographic follow-up period, until the day of euthanasia (Fig. 2).
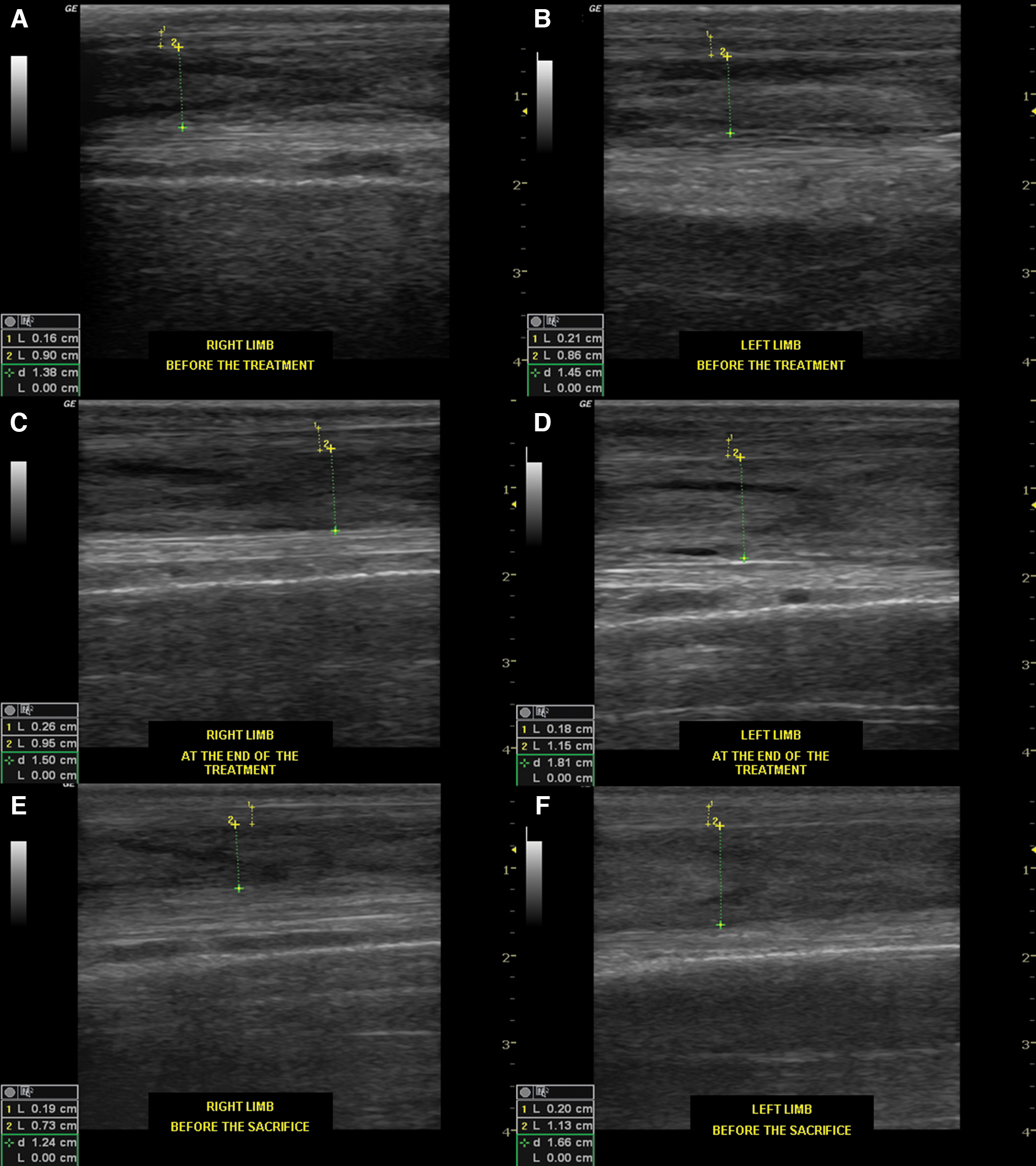
Longitudinal ultrasonographic images of representative deep digital flexor tendon (DDFT) treated with 5 J/cm2 and the relative control. The panel shows:
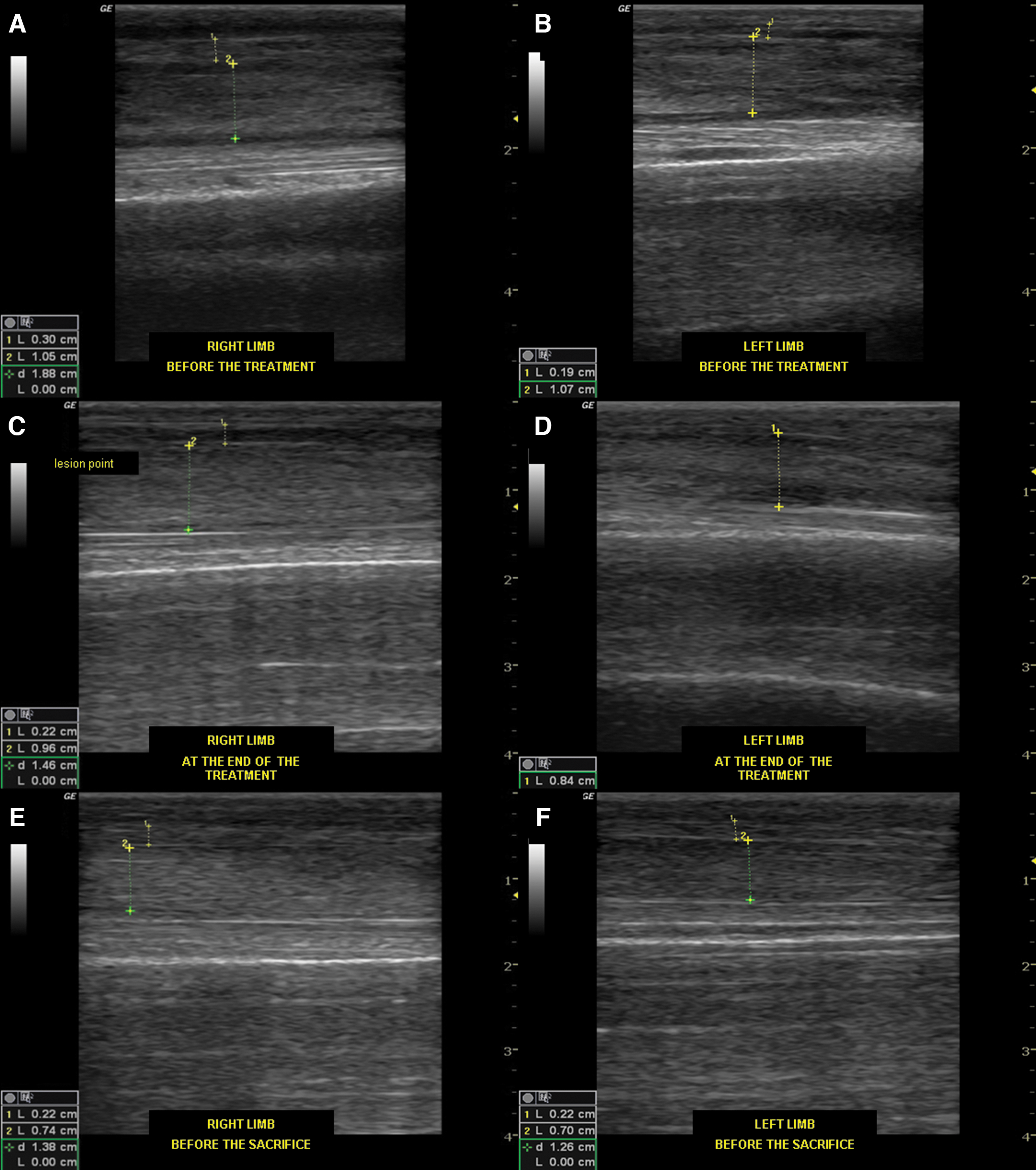
Longitudinal ultrasonographic images of representative deep digital flexor tendon (DDFT) treated with 2.5 J/cm2 and the relative control. The panel shows:
Mean value of circumferences of treated (left) and control (right) limb of both groups (group 1, left limb treated with 5 J/cm2; group 2, left limb treated with 2.5 J/cm2) recorded daily with a tape measure at the lesion point.
Histological analysis
Sections of tendons were obtained from the area of the lesions caused by collagenase. A serious disorganization of the extracellular matrix (arrows in Fig. 4), an increased cellular density (*in Fig. 4), and neovascularization (§in Fig. 4) were detected in the DDFTs of control limbs in both groups (Fig. 4B). After the lesion, the increase in cell numbers was characterized by infiltration of randomly distributed fibroblastoid cells with hyperchromatic nuclei; also the blood vessels were numerous and unaligned, and possessed dilated lumen. Furthermore, the matrix appeared less compact and there were empty spaces between fiber bundles (Fig. 4B). By contrast, all sheep treated with MLS laser therapy showed a more uniform and organized tissue repair and a decrement of cellularity (Fig. 4C, D) if compared with control limbs (Fig. 4B). Furthermore, a slight improvement in terms of realignment of collagen fibers was noted in the treated group (Fig. 4C, D), versus the untreated group (Fig. 4B). In group 1 (5 J/cm2), in the left treated legs, a significant decrease of fibroblasts was observed respect to lesioned tendons (Fig. 5A), whereas blood vessels areas did not differ between lesioned (Fig. 5B) and treated tendons (Fig. 5C, D). In group 2 (2.5 J/cm2), in the left treated legs, a decrement in the number of fibroblasts and a significant decrease of blood vessel areas were observed compared with control tendons (Fig. 5B).
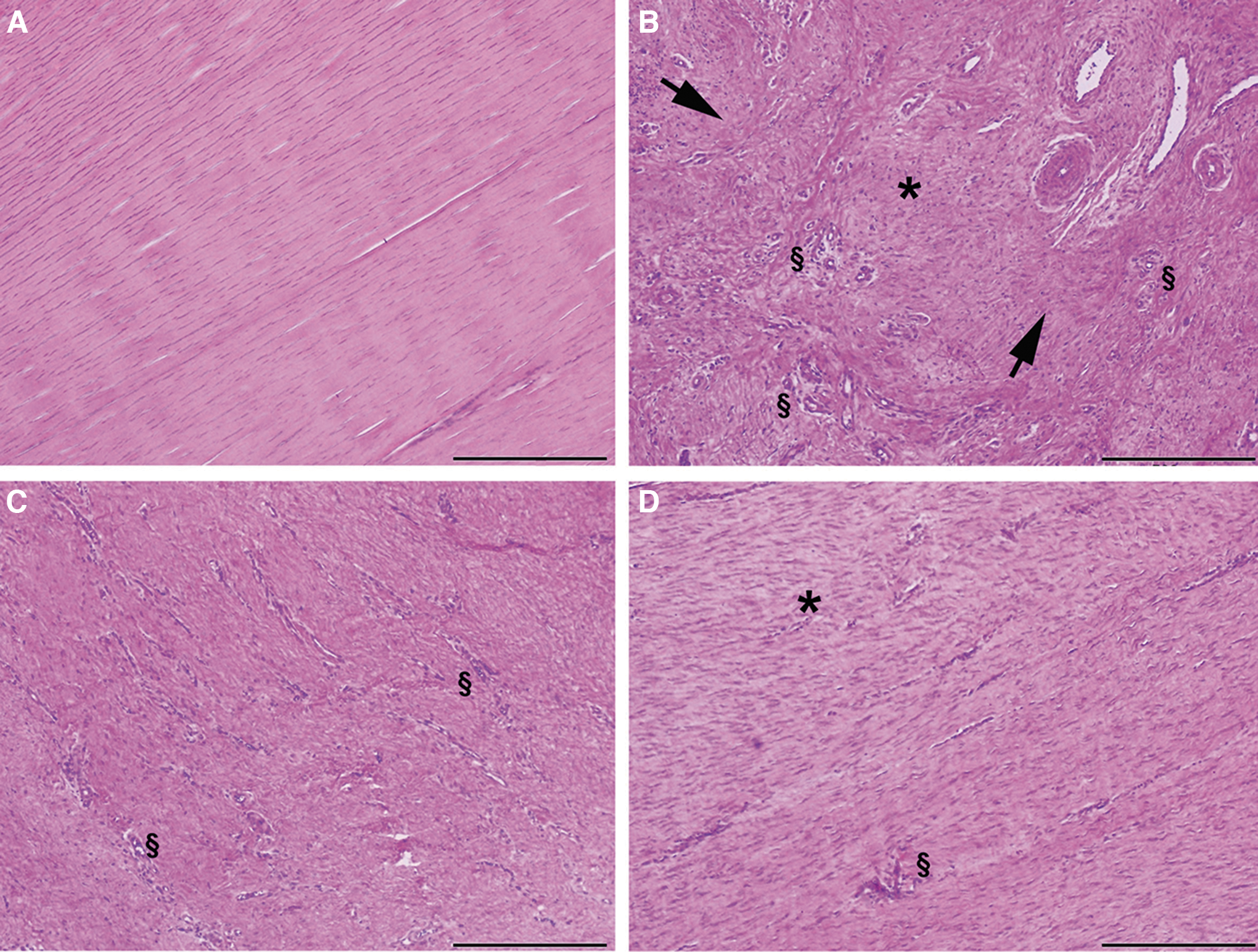
Histological characteristics of the tendon sample. Representative histological sections stained with hematoxylin and eosin (H&E): healthy tendon
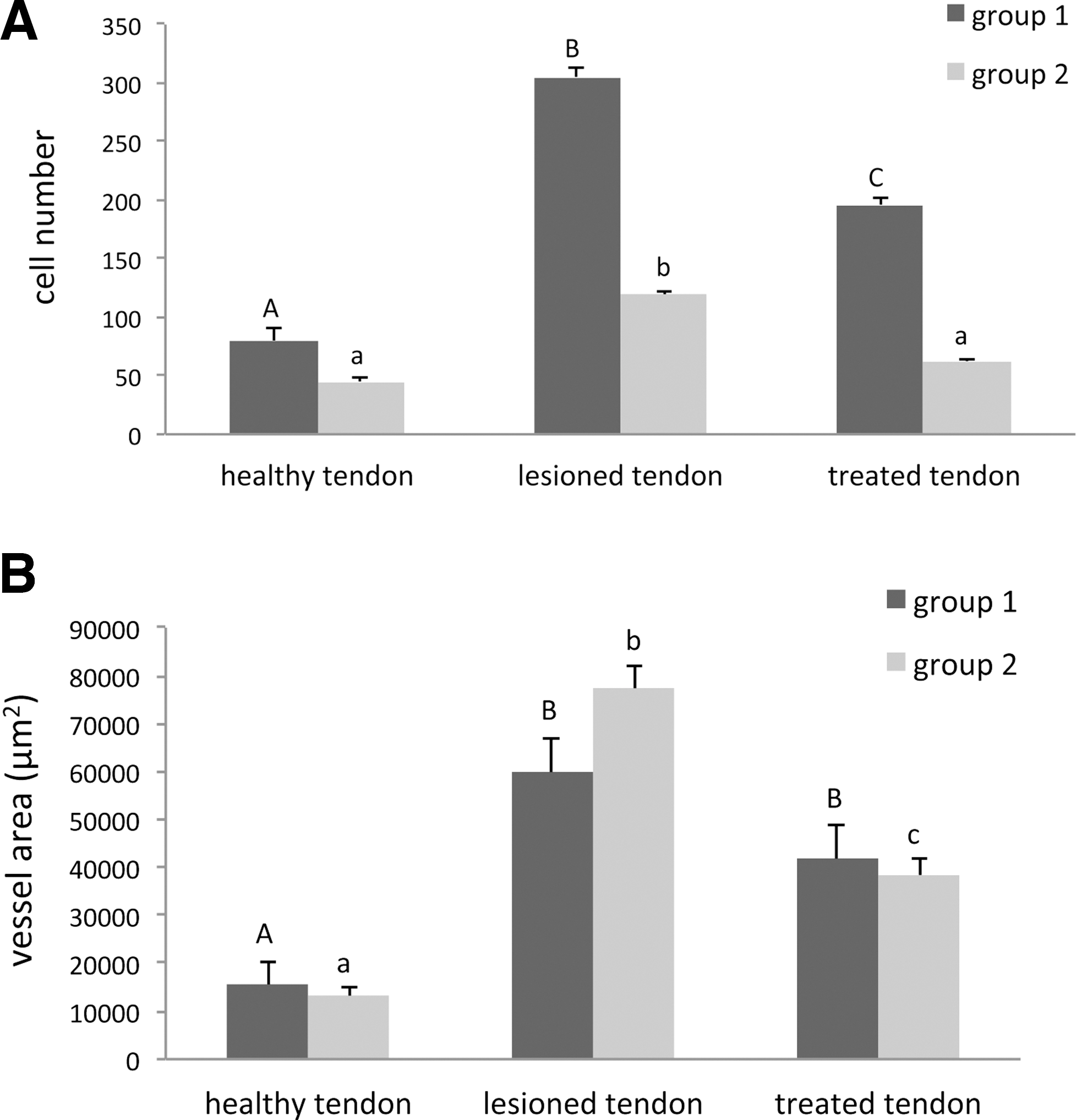
Graphics representing the cell number and the vessel area evaluation.
Discussion
Most of the studies previously reported in the literature have certainly laid the basis for the study of the treatment of tendinopathy with laser therapy. 6 –13,15 –17,20,39 In vivo studies have revealed that LLLT could enhance healing in the Achilles tendon by improving collagen fiber organization and preventing oxidative stress, as well as reducing fibrosis. 7 –9 However, the reported literature shows significant differences compared with the characteristics of our pilot study. In fact, to the best of the authors' knowledge, this is the first experimental pilot study that analyzes the clinical, ultrasonographic, and, especially, histological effects of LLLT, and in particular MLS laser therapy, on the tendon healing process in sheep.
In other studies, only biochemical and biomechanical aspects were assessed. 39 Furthermore, compared with other studies, we have preferred to analyze the effects of the laser as a single therapeutic tool without associating this treatment with other pharmacological or physiotherapeutic approaches. 7,33,40,41 We evaluated the effects of two different doses of MLS laser therapy, obtained using the MLS laser pulse, in the acute phase of tendon lesions induced with a bacteria-derived collagenase. This enzyme, already used in several experiments on rats, sheep, and horses, mimics the mechanisms of a traumatic event. 36,38 The use of sheep, chosen as a model for human and equine tendinitis, was because of the similar connective structure of the flexor tendons in this species; 23 –25 the sheep is the most widely used experimental model for the study of human and equine musculoskeletal disorders, and is recognized as a model of human and equine orthopedic disease, including tendinopathy. 26 –28 Therefore, for an accurate assessment of the effectiveness of LLLT, it has been decided not to use small laboratory animals, 23 as opposed to what was done previously in other studies in which rats and rabbits were used as experimental models. 7,8,16,19 –21,39 Sheep are good candidates for the development of an equine tendon injury model.
The MLS laser pulse has been specifically developed to combine dual wavelengths and both types of emission, continuous and pulsed, and has already been used in one animal study, 42 but never in an animal model study involving sheep. The protocols used in this study considered two different fluences of the laser in order to determine a suitable therapeutic range for physiotherapy treatment in human and veterinary medicine.
In 2009, Enwemeka reported that the high prevalence of dosage-related mistakes in published reports suggested that dosage determination errors were common among clinicians and other end-users. 43 The latest reviews on the effectiveness of LLLT in human medicine 6,9,19 highlighted the need to identify a specific treatment protocol for the disease, and the lack of precise instructions for treatment protocols together with the heterogeneity of the clinical cases, as the main causes of conflicting results obtained with LLLT for the treatment of tendinopathy. This fact is confirmed, because a clear relationship between the positive results and the use of the recommended doses was observed. 6 Several authors 9,16,17,21,40,41,43,44 reported the efficacy of LLLT in the increase of the mechanical properties, and the increase of orientation of collagen fibers and angiogenesis, using doses between 3 and 5 J/cm2 in the treatment of disorders of the calcaneal tendon. The use of the latter dosage, with wavelengths in the range of 780–820 nm, was also recommended in 2005 by the World Association of Laser Therapy (WALT). Other studies performed in an experimental model of collagenase-induced tendonitis in rats reported similar values of wavelengths ranging between 780 and 810 nm, and values of highly different energy densities ranging between 1 and 7.7 J/cm2. 7,8,20,39 In particular, as reported by Marcos et al., LLLT administered with an energy dose of 3 J/cm2 significantly increased COX-1 gene expression, and reduced cyclooxygenase (COX)-2 gene expression and COX-2-derived PGE2 production, vascular permeability, and edema formation. 7 Frigo described the negative effect on a primary fibroblast cell culture irradiated with an extreme value of 21 J/cm2, as it increased cell death and inhibited cell proliferation. 45
In the present animal model study, the authors decided initially to use the influence of 5 J/cm2, as this is the average value reported in the literature for the treatment of acute tendinitis in human medicine. Given the clinically and ultrasonographically excessive effects in the first group of animals, the authors chose to use the fluence reduced by 50% for the treatment of the second group.
The clinical response was different between the two groups: in the second group, treated with lower fluence, the symptoms could be defined as more pronounced and with minor differences between treated and control limbs; at the end of the trial, the external morphology of the tendon returned to the physiological state. In contrast, the tendon circumference of the first group did not return to normal after 1 month of follow-up. Considering that the healing of tendon tissue is a long-term process (15–18 months 46,47 ), we expected, after 1 month from the tendon injury, the lack of an inflammatory process and an active remodeling phase. From the clinical evaluation of the first group, with the use of the laser set at 100% intensity and a fluence of 5 J/cm2, it was not possible to state clearly that MLS laser therapy had an anti-inflammatory, analgesic, and anti-edema effect, as indicated by the manufacturer and related studies; 46 in particular, in two sheep, the clinical manifestation worsened slightly during the initial phase, with an increase of circumference at the injection site, local temperature rise, and a slow remission of symptoms. The aggravation of the inflammatory condition, observed during the applications of MLS laser therapy in the first group, seems to indicate that, for the treatment of an acute tendinitis with this type of laser emission, the dose of 5 J/cm2 was excessive for the therapeutic effect. Results from histological examinations indicate that both treatments induced a statistically significant cell number decrease, although only in the second group did the values return to normal. Moreover, the MLS dose of 2.5 J/cm2 (group 2) caused a significant decrease of the vessel area. This is in agreement with reports in the literature, in which it appears that the therapeutic window falls between 3 and 5 J/cm2 in order to obtain a more effective anti-inflammatory, analgesic, and biostimulating effect with LLLT. 13
Conclusions
In conclusion, the results obtained with the use of this particular model of laser (MLS) seem to indicate that the parameters used in the first group were, perhaps, excessive in cases of acute tendon injuries, probably because they seemed to exacerbate the inflammatory effect induced by collagenase; by contrast, the parameters used in the second group seemed to be suitable in cases of acute tendon injuries, for determining a biostimulating effect on the physiological mechanism of tendon healing.
It would be interesting to conduct further studies to corroborate the effect of fluences ranging between those used in this study.
Footnotes
Acknowledgments
The authors thank Anthea Rowlerson for her technical assistance in editing this article.
Author Disclosure Statement
No competing financial interests exist.