
Abstract
Introduction
D
Currently there are at least two recognized mechanisms of action of desensitizing agents: (1) blocking fluid movement by occluding tubules, and (2) blocking pulpal nerve activity by altering the excitability of the sensory nerves. A wide variety of chemical and physical agents have been used for the treatment of the dentin hypersensitivity, such as anti-inflammatory agents (corticosteroids); protein precipitants (formaldehyde, silver nitrate, strontium chloride hexahydrate); tubule occluding agents (calcium hydroxide, potassium nitrate, sodium fluoride); and tubule sealants (resins and adhesives). 6 –10 Grossman 11 reported a number of requirements that an effective desensitizing agent or therapy must have. These are: the agent should be easy to use; not be an irritant to the pulp; be relatively painless on application; be rapid in action; be effective for a long period; not have staining effects; and be consistently effective. To date, however, no single agent or form of treatment has been found effective for all patients. During the past two decades, lasers have been one of the rewarding new modalities used for dentin hypersensitivity treatment. Many laser systems, including He-Ne, GaAlAs, Nd:YAG, CO2, Er:YAG, and Er,Cr:YSGG, have been used for dentin hypersensitivity therapy. 12 –15 Er:YAG lasers are effectual in both medical and dental applications because of having a thermomechanical ablation mechanism, and because of the high absorption of their wavelength by water. A previous in vitro study concerning dentin hypersensitivity treatment with Er:YAG laser showed that because of the encouraging 6-month results, this tool was the best treatment option for desensitization. 16
A recent review claims that ideal dentin hypersensitivity treatment should imitate natural desensitizing processes and lead to spontaneous occlusion of exposed dentine tubules. 17
From this standpoint, researchers improved a new physical agent, consisting of 8% arginine, an amino acid found in saliva, in combination with calcium carbonate for in-office application. Petrou et. al. 18 reported that when this product was applied to exposed dentin, surface tubules were sealed with a plug, which is resistant to normal pulpal pressures and acid challenge, and effectively reduces dentin flow and, thereby, reduces hypersensitivity symptoms.
To increase the effectiveness of dentin hypersensitivity treatment, researchers postulated combination treatments, such as lasers and chemical agents. Kumar and Mehta 19 reported that a combination of Nd:YAG laser and 5% sodium fluoride (NaF) varnish seemed to show efficacy, when compared with either treatment alone, in treating dentine hypersensitivity. Likewise, in an in vitro study, combination therapy with lasers and NaF gel groups showed more marked tubule occlusions than lasers alone. 20 However, in a clinical trial, after a 6 month follow-up period, no significant differences were noted between the laser and laser plus NaF gel groups. 21
In view of this knowledge, effective dentine hypersensitivity treatment modalities are still being surveyed today. Nevertheless, combination therapy with lasers and chemical agents may have more desirable outcomes for treating dentine hypersensitivity. With an interest in effective dentine hypersensitivity treatment, this study aimed to evaluate the in vitro effects of Er:YAG laser and an in-office desensitizing paste containing 8% arginine and calcium carbonate alone, or in combination by using scanning electron microscopic (SEM) analysis.
The null hypothesis was that there would be no significant difference in the diameters of open dentinal tubules and the numbers of open tubules per 100 μm2 between the Er:YAG laser alone and the combined treatment group.
Materials and Methods
Preparation of dentine specimens
Twenty freshly impacted extracted human third molars were used in this study. The molars were obtained from adults 23–30 years of age. Prior to preparation of dentine specimens, the teeth were stored in 4°C distilled water with thymol as a preservative to inhibit microbial growth until their use. Dentine slices with a thickness of 3 mm were then prepared from each tooth, which is described by Çakar et al. 20
Treatments
Forty dentine specimens with exposed dentinal tubule orifices were divided into four groups. No treatment was applied to the dentine samples in Group I, which served as the control group. Samples in Group II were irradiated with Er:YAG laser (DE- Light; Hoya ConBio, Fremont, CA) with a straight quartz round tip of 600 μm diameter at an energy level of 60 mJ per pulse, and a repetition rate of 30 Hz, for 10 sec. The laser beam was swept in a mesiodistal fashion with the beam directed perpendicularly to the dentine surface in noncontact mode (without water irrigation) at a distance of from 3–4 mm. Desensitizing paste was applied twice in 3 sec consecutively, according to according to the manufacturer's instructions, to the samples in Group III. And in Group IV, desensitizing paste applied twice in 3 sec consecutively, and then the specimens were irradiated with Er:YAG laser at the same parameters as were used with Group II.
SEM analysis
The surface morphology and dentinal tubular occlusions or patencies were observed with SEM. The dentine specimens were fixed in 2.5% glutaraldehyde in 0.1 M phosphate- buffered saline (pH 7.2) for 24 h at room temperature, washed with distilled water, and air dried. Then the specimens were critical point dried and coated with an≈20 nm platinum layer in a sputter-coater. The platinum-sputtered specimens were then placed in the vacuum chamber of the SEM (JSM 6335F; JEOL-USA, Inc., Peabody, MA) at an accelerating voltage of 10 kV. The SEM photomicrographs of each specimen were taken at 1000× and 2000× magnifications.
The number of dentinal tubules per square millimeter was counted in the center of each specimen on the 1000× photomicrographs. These calculations were facilitated by covering each photomicrograph with an overlay of tracing paper that was firmly attached to the photograph, and the tubules were marked off as they were counted. The tracing paper comprised a square frame with a border length representing 100 μm on the dentine specimen, allowing calculation of the number of tubules per 100 μm2.
The diameter of the dentinal tubules was determined at 2000× magnification, and the tubule diameters were measured on each specimen. The microphotographs were loaded in a computer program (AutoCAD® 2010; Autodesk Inc, USA) for eliminating the measurement errors. Only those tubules that had a nearly circular lumen were selected. The measurement of the smallest diameter across the tubule's orifice minimized the error caused by tubules cut obliquely. The size was calculated by using the reference scale bar on the photomicrograph. The diameters of the dentinal tubule orifices were measured on the photomicrographs and converted to the real size. A single investigator performed all morphometric measurements.
Statistical analysis
Descriptive statistics including means and standard deviations were calculated for each group. The statistical analysis was performed using NCSSS 2007 & PASS 2008 Statistical Software (Number Cruncher Statistical System, UT) program. Intergroup multiple comparisons of the groups were performed by Kruskal–Wallis test. The multiple (double) comparison Mann–Whitney U test was used when the Kruskall–Wallis test presented a significant difference. Significance for all the tests was predetermined at a probability value <0.05.
Results
In the SEM micrograph of Group 1, it was observed that smear layer was totally removed, and dentinal tubules of different diameters were aligned parallel with each other (Fig. 1). In the SEM micrograph of Group 2, Er:YAG laser applied dentine surface and dentine tubules are observed following citric acid application. In the SEM micrographs of Group II where Er:YAG laser was applied, it was observed that a small number of exposed dentinal tubules were present because of the melting of the dentine and the fact that their diameters were narrow (Fig. 2). In the SEM of Group 3, it the dentine surface and tubules could be observed where a hypersensitivity paste containing 8% calcium carbonate was applied following citric acid application. In Group III, it was observed that the superficial dentine tubules were obliterated, and the small number of remaining dentinal tubules had narrow diameters (Fig. 3). In Group IV, it was observed that almost all surfaces were obliterated in samples where 8% arginin-calcium carbonate containing hypersensitivity paste and Er:YAG laser in combination were applied (Fig. 4). The mean values and standard deviations of the diameters of open dentinal tubules and the numbers of open tubules per 100 μm2 are presented in Table 1. Significant inter group differences were detected for both parameters (p<0.05). The results of the Mann–Whitney U comparisons test are shown in Table 2. It was determined that the diameters of the open dentinal tubules and the numbers of open tubules per 100 μm2 in Group I were significantly higher than in Groups II, III, and IV. No significant difference was observed between Groups II and III and between Groups II and IV, whereas a significant difference was detected between Group III and Group IV in favor of Group IV in both investigated parameters.

Photomigraph of dentine specimen from citric applied group (×2000).

Photomicrograph of a dentine specimen treated with Er:YAG laser only (×2000).

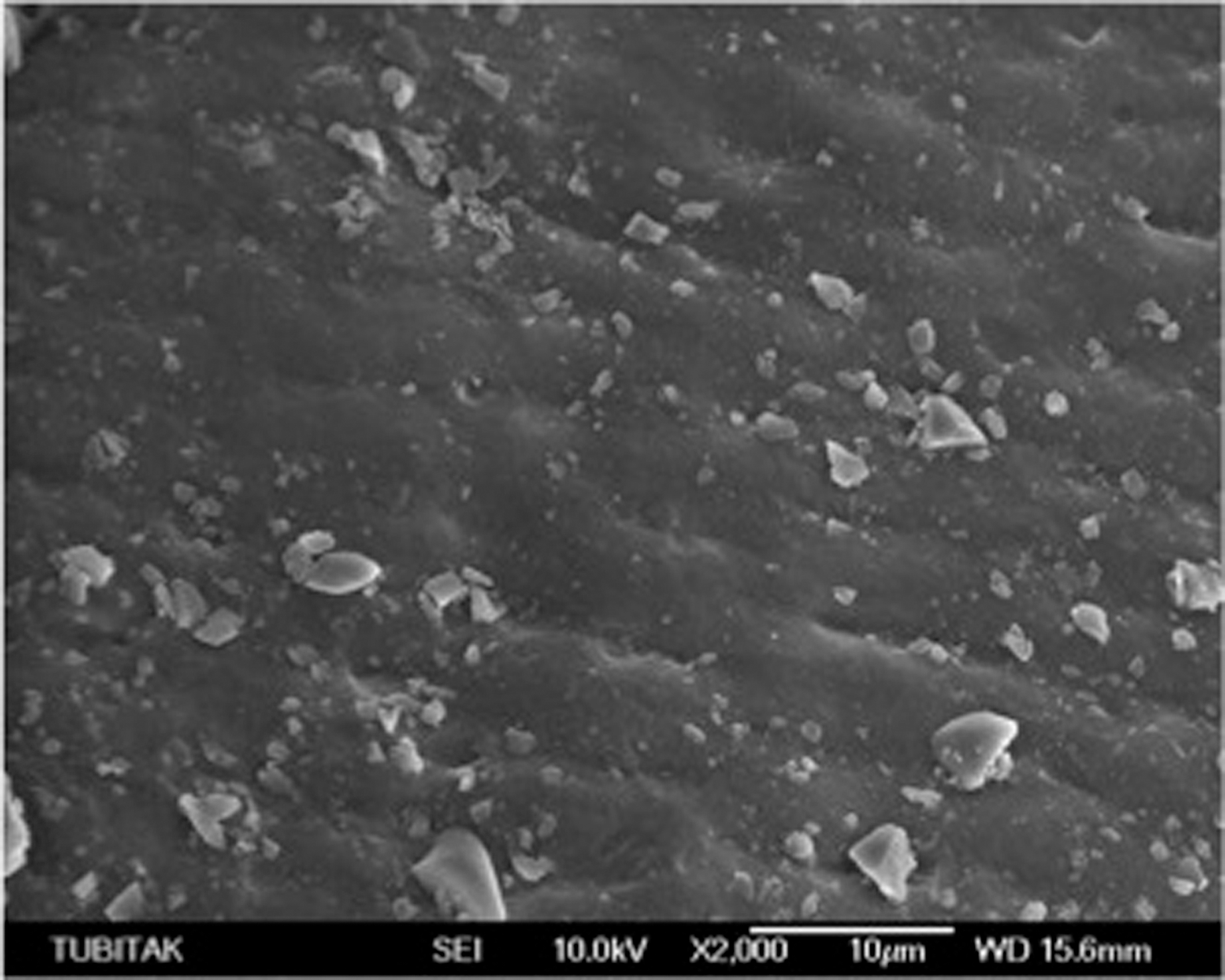
Photmicrograph of dentine specimen where hypersensitivity paste containing 8% calcium-carbonate applied group (×2000).
Photomicrograph of a dentine specimen from the combined treatment applied group (×2000).
Kruskal–Wallis Test, p<0.05.
Mann–Whitney U test, p<0.05.
Discussion
Dentin hypersensitivity is one of the most problematic and least solved oral conditions in dentistry. In the present study, the use of a new desensitizing paste consisting of 8% arginine and calcium carbonate combination, with or without Er:YAG laser to occlude dentin tubules, was assessed, and the null hypothesis was approved.
It is already known that dentinal tubules exposed to the oral environment are directly related to dentinal hypersensitivity. A theory proposed about dentine hypersensitivity and pain conduction is that dentinal tubules play a significant role in the transfer of stimuli from the dentine surface to the pulp. 5 According to the studies performed so far, dentinal hypersensitivity is related to the number of exposed tubules on root surfaces. 22,23 Factors such as the number and diameter of tubules are directly proportional to the intensity of the transfer of the stimulus. 22,24 The main target of a successful hypersensitivity treatment is the narrowing or complete obliteration of dentinal tubules.
This study was designed as an in vitro SEM analysis for the evaluation of the effects of the treatment modalities on surface morphology, thereby enabling the researcher to select the most effective methodology. For the evaluation of the effect of 8% arginin-calcium carbonate containing hypersensitivity paste alone or in combination with Er:YAG laser, the number of exposed dentinal tubules and the number of tubules per 100 μm2 were calculated.
In the present study, 20 freshly impacted extracted human third molars were used. The mean number and diameters of dentinal tubules may vary in different teeth, as they are affected by factors such as age, tooth type, depth of the dentinoenamel junction, and dentinal sclerosis. 25,26 Therefore, another reason for the use of impacted third molars in our study was that they were obtained from a specific age group (23–30 years of age) enabling an even distribution among groups. 26 The reason why the 3 mm portions below the cementoenamel junctions were sectioned was that 93% of dentinal hypersensitivity is observed in the cervical portions, 27 and also, special care was taken to include an adequate number of samples in each group to enhance the power of the statistical analysis.
In the literature, it is indicated that different amounts of decalcification occur following the applications of different concentrations of acid on dentine surfaces. Therefore, varying results are likely to be obtained in studies, as the degree of exposure will differ. It has been reported that 5 min preservation of the samples in 1% citric acid is the most appropriate methodology to remove the smear layer without damaging the surface structure. 28 In the present study, 1% citric acid was applied on root surfaces for 5 min. This procedure was performed to simulate dentinal tubules exposed to the oral environment in teeth with hypersensitivity symptoms. In the micrographs of the control group, clean and smooth surface images without smear layer and exposed dentin tubuli were observed. Our findings are in accordance with the literatüre. 19,20,29
Micrographs of Group II revealed a melted and irregular surface structure and homogeneous occlusion of dentinal tubuli openings. The reason for the irregular surface appearance is the closure of dentinal tubule openings by the melting of intertubular dentin. There was a significant reduction in the diameters of dentinal tubules (1.05±0.73 μm) and and average number of tubuli per 100 mm2 (0.03±0.03/100 μm2) compared with the control group (2.41±0.11 μm and 1.44±0.07/100 μm2, respectively). Aoki et al. 30 reported that Er:YAG laser application caused minimal thermal damage on sound dentin. The energy parameters used in the present study are 60 mJ/pulse and 30 Hz, and our values are consistent with those of Çakar et al., Ipci et al., and Gursoy et al. 20,21,29
The micrographs taken from Group III showed that following sensitivity paste application containing 8% arginin and calcium carbonate, the paste exhibited a well distribution on the surface; however, some materials in the constitution of the paste remained suspended on the surface as microparticules. It was observed that the application of 8% arginin-calcium carbonate containing paste narrowed the dentinal tubule diameters from 2.41±0.11 to 1.34±0.50 μm. The average numbers of dentinal tubules per 100 μm2 in Group III (0.06±0.04/ 100 μm2) was significantly reduced compared with the control group.
There is a limited number of investigations on dentin hypersensitivity using the 8% arginin-calcium carbonate paste used in the present study.
In the first pioneering study performed on this agent, Kleinberg et al. 31 reported that after application of 8% arginin and calcium carbonate containing paste on hypersensitive teeth, a very rapid relief was observed, which lasted for 28 days after a single application.
In another clinical study, Schiff et al. 32 utilized an 8% arginin-calcium carbonate containing paste and another polishing paste immediately after tooth surface cleaning. They observed that a statistically significant difference was observed in the 8% arginin-calcium carbonate containing group against tactile and air stimulants after 4 weeks. However, no significant difference was noted between the groups during the 12th week of the follow-up period.
In another clinical study, a polishing paste was applied on patients with hypersensitivity prior to scaling (as the control group) and 8% arginin and calcium carbonate was applied to an experimental groups. The patients were asked to report their level of hypersensitivity to tactile and air stimulants. The results showed that a significant reduction in hypersensitivity was observed after tactile and air stimulation in the experimental group, which was significantly lower than in the control group. 33
In an in vitro study, after 8% arginin and calcium carbonate containing paste was applied on exposed dentin surfaces, it was observed that an arginin, calcium, phosphate and carbonate containing plug was formed. The results of this study correlate with our findings in which the micrographs show the occlusion of dentinal tubules. 18
There are few studies of the innovative hypersensitivity reducing agent we used in our study. However, it had beenpreviously proposed as an alternative treatment modality. There are many agents that are used for the occlusion of dentinal tubules, such as the 8% arginine and calcium carbonate containing paste.
The most frequently used agent is NaF. In an SEM study performed using the polishing form of NaF, Kumar and Mehta 19 reported that in the group in whom 5% NaF polishing paste was applied, tubular diameters reduced from 4.13±0.49 to 1.93±0.17 μm, compared with the control group.
In an in vitro study, Çakar et al. 20 reported the average number of dentine tubules per 100 μm2 in the 2% NaF gel group to be 0.98±0.5, and the average tubular diameter as 1.51±0.23 μm. They further indicated that these differences were statistically significant compared with the control group. When the results of the aforementioned study are compared with ours, it can be concluded that the hypersensitivity paste we used more successfully occludes dentine tubules by itself, compared with the 2% NaF gel.
In Group IV of our study, 8% arginin-calcium carbonate containing hypersensitivity paste was used with Er:YAG laser. In the images, it was observed that almost all dentine tubules were occluded, and that there was a reduction in the diameters of remaining open dentinal tubules.
It was also observed that remaining microparticles of paste application persisted following laser application and, similarly to in Group II, there was a melted and smoother surface appearance.
In Group IV, in which a combined treatment was performed, the average tubule diameter, number of exposed tubules, and average number of tubules per 100 μm2 were 0.72±0.70 μm, 1.50±1.43, and 0.01±0.01, respectively. In double comparisons between groups, in all three evaluations, there was no difference with the Er:YAG laser group. However, a significant difference was noted when compared with the 8% arginin-calcium carbonate containing group.
In a similar in vitro study, when the tubular diameters and number of dentine tubules were compared in groups in which Er:YAG laser had been used alone and in combination with NaF gel, no statistically significant difference was noted. However, when surface morphologies were evaluated in micrographs, a more evident and less suspectible occlusion was noted in samples with combined treatment. 20
In the light of this information, 8% arginin-calcium carbonate containing hypersensitivity paste used in conjunction with Er:YAG laser is a promising method for the treatment of dentinal hypersensitivity, which is frequently observed and does not have a definite treatment in clinical practice.
Conclusions
The results of this study have shown that all applied treatment options were effective in the occluding and narrowing of dentinal tubules, and that a more prominent occlusion was observed in the combined treatment group, but that Er:YAG laser alone and combined treatment can both be effective in the treatment of dentinal hypersensitivity. This study plays a pioneering role in long-term clinical studies.
Footnotes
Author Disclosure Statement
No competing financial interests exist.