
Abstract
Introduction
T
Sodium hypochlorite (NaOCl) is a common irrigation solution used in endodontic therapy because it has bactericidal properties and dissolves organic tissue. However, this solution cannot remove the smear layer when used alone. 6 Another common irrigation solution contains EDTA, which reacts with calcium ions in the dentin to produce soluble calcium chelates, 7 and removes the mineralized portion of the smear layer. 8 Some researchers have reported that the ideal way to remove the smear layer is to alternate between EDTA and NaOCl. 9
Irrigation can be performed via manual or machine-assisted systems. 10 Manual irrigation techniques include positive-pressure irrigation (PPI), commonly conducted with a syringe and an endodontic needle. Machine-assisted irrigation techniques include sonic and ultrasonic methods, as well as newer systems such as apical negative-pressure irrigation, 11 plastic rotary files, 12 and photo-initiated photoacoustic streaming. 13 Two important factors should be considered during irrigation: whether the system can deliver the irrigant to the entire root canal system, and whether it is capable of debriding areas that are inaccessible to mechanical instrumentation, such as lateral canals and isthmuses. 12 Therefore, it is important to investigate whether these systems enable the irrigation solution to infiltrate the apical third of the root canal and the lateral canals.
Recent studies have shown that ultrasonic activation of irrigants improves debridement compared with conventional syringe irrigation. 14 An ultrasonically oscillating file transmits energy, causing acoustic microstreaming and mixing of the irrigant; it enables the irrigant to reach inaccessible regions, and enhances shear stress on the root canal surfaces at a distance from the file. 15,16
Passive ultrasonic irrigation (PUI) of the root canal involves activation of the irrigant without simultaneous instrumentation by an ultrasonically activated file in the canal. 17,18 Increased ultrasonic-device intensity leads the irrigation solution around the file, within the canal, to move rapidly. 19 De Moor et al. 20 compared the effects of PUI and laser-activated irrigation (LAI) on dentin debris, and concluded that the laser technique gives results comparable to those of the ultrasonic technique, with longer irrigation times.
LAI has been used for root canal irrigation. 21 –23 George et al. 23 performed an in vitro study examining the capacity of lasers to activate irrigants inside the root canal system, in order to increase their action on the smear layer. Deleu et al. 24 compared the efficacy of different irrigant activation methods in removing debris from root canal. They found that the Er:YAG laser demonstared the best results. LAI can remove the smear layer from the root canal wall, but may also cause extrusion of the irrigant through the apex. 22
The aims of this study were: 1. To evaluate three different techniques of smear-layer removal from the root canal surface: PPI, PUI and LAI, using 17% EDTA as the irrigation solution 2. To determine the best technique for each irrigation method, that is, applying it to the coronal upper third or the entire working length (WL) of the root canal.
Materials and Methods
Tooth samples
Sixty single-rooted human teeth (central incisors) extracted for periodontal reasons were used. (Ethics committee approval was received from Hadassah Hospital). Radiographs were taken from two angles before the endodontic procedure. Root canal preparation was performed using ProTaper™ (Dentsply Maillefer, Baillaigues, Switzerland) F3 Ni-Ti files with 2.5% NaOCl irrigation. All canals were rinsed with 10 mL of 17% EDTA using a syringe with 27-G needle (Navitip) for 60 sec during the working time, in the three tested techniques. The apices of all teeth were sealed with Super-EBA (Harry J. Bosworth Co., Skokie, IL) to prevent irrigant leakage.
After the various treatments, two longitudinal cuts were made with a high speed bur, and the teeth were split in half. All teeth were positioned in identical fashion.
The teeth were randomly divided into six groups, 10 teeth in each group. Group 1 was treated with ProTaper™ F3 Ni-Ti files, and served as a negative control. Group 2 was irrigated with 10 mL of 17% EDTA using a syringe with a 27-G needle (Navitip) with the apical opening placed inside the canal for 60 sec. Group 3 was subjected to PUI with 17% EDTA, performed with a stainless steel #25/.00 file (Irri-Safe; Acteon, Merignac, France) placed 1 mm short of the WL from the narrow apical part, driven by an ultrasonic device (Suprasson PMax; Satelec, Acteon, France) at a power setting of 5 for 60 sec. Group 4 was subjected to PUI with 17% EDTA, performed with a stainless steel #25/.00 file (Irri-Safe); driven by an ultrasonic device (Suprasson PMax) at a power setting of 5, placed in the upper coronal third of the canal for 60 sec. Group 5 was subjected to LAI with Er:YAG laser at a wavelength of 2940 nm (Syneron,Yokneam, Israel) equipped with a 17 mm 400 μm plan-ended sapphire tip. Radiation was 158 ms set to 0.5 W, 50 mJ, 10 HZ for 60 sec. The water spray of the laser was closed. An irrigation solution of 17% EDTA was injected during radiation. The laser tip was inserted 1 mm short of the WL. The coaxial water spray feature of the handpiece was shut off. Group 6 was subjected to LAI with Er:YAG laser (Synron) at a wavelength of 2940 nm equipped with a 17 mm, 400 μm plan-ended sapphire tip. Radiation was 158 ms set to 0.5 W, 50 mJ, 10 HZ for 60 sec. The water spray of the laser was closed, and an irrigation solution of 17% EDTA was injected continuously into the root canal during the radiation.
The laser tip was inserted in the upper coronal third of the root canal. The coaxial water spray feature of the handpiece was shut off.
Scanning electron microscopy (SEM)
All samples were dried and mounted on stubs and then coated with Au/Pd using a Polaron SC7640 Sputter Coater (Polaron, Hertfordshire, UK). The effects of the irrigation treatments on the smear layer were examined by SEM at a magnification of 1000× in the coronal, middle, and apical parts of the root canal. The samples were examined using FEI Sirion High Resolution SEM and FEI Magellan Ultra-High Resolution SEM (FEI, Eindhoven, The Netherlands).
Microanalysis of surface element distribution by energy dispersive X-ray spectroscopy (EDS)
The chemical content of the root canal surface following laser irradiation was evaluated in the coronal, middle, and apical parts. The aim was to measure the effects of the various treatments on the surface chemistry of the minerals. All samples were analyzed by an FEI Quanta 200 SEM (FEI, Eindhoven, The Netherlands) equipped with an EDAX (Tilburg, The Netherlands) EDS system (Sapphire Si[Li] ultra-thin window [UTW] detector, 10 mm2, spectral resolution 128 eV) at an accelerating voltage of 15.0 kV, spectral acquisition time of 50 sec, and dead time of ∼15%. The EDAX ZAF matrix correction was applied for quantifications. Differences in the surface distribution of several key elements of dentin, including Ca, P, and O, were evaluated. Spectral acquisition and quantification were performed using EDAX Genesis software. Element content was determined in wt % and all measurements were compared with controls.
Statistical analysis
All assays were performed in triplicate. The ANOVA model with repeated measures was applied to test Ca, P, O, and the Ca/P ratio in dentin for all treatment groups. Kruskal–Wallis nonparametric ANOVA was used to test the statistical significance of the differences among the groups. A p value of ≤0.05 was considered statistically significant. Data are presented as mean±SD.
Results
Examination of surface morphology
Figure 1 shows SEM micrographs of the dentin wall of the coronal (A), middle (B), and apical (C) thirds of the root canal. In the control group, a thick smear layer can be seen (Fig. 1, line 1). Irrigation with 17% EDTA through a syringe for 60 sec removed part of the smear layer in the coronal and middle areas; however, the smear layer on the apical third was unchanged (Fig. 1, line 2). The addition of PUI improved smear-layer removal in all parts of the canal, but the dentinal tubules were closed in the apical part and open in the coronal part (Fig. 1, line 3). Er:YAG LAI with 17% EDTA showed the best smear-layer removal from the entire root canal surface, including areas with open dentinal tubules (Fig. 1, line 4). The effect on smear-layer removal of PUI combined with 17% EDTA applied to the coronal third of the root canal (Group 4) was found to be depth dependent. The smear layer was removed from all parts of the root; however, the dentinal tubules were only open in the coronal and middle parts of the root (Fig. 1, line 5). In contrast, when the laser tip was only inserted in the upper coronal third (Group 6), the smear layer was removed, and tubules were open in all parts of the canal (Fig. 1, line 6).
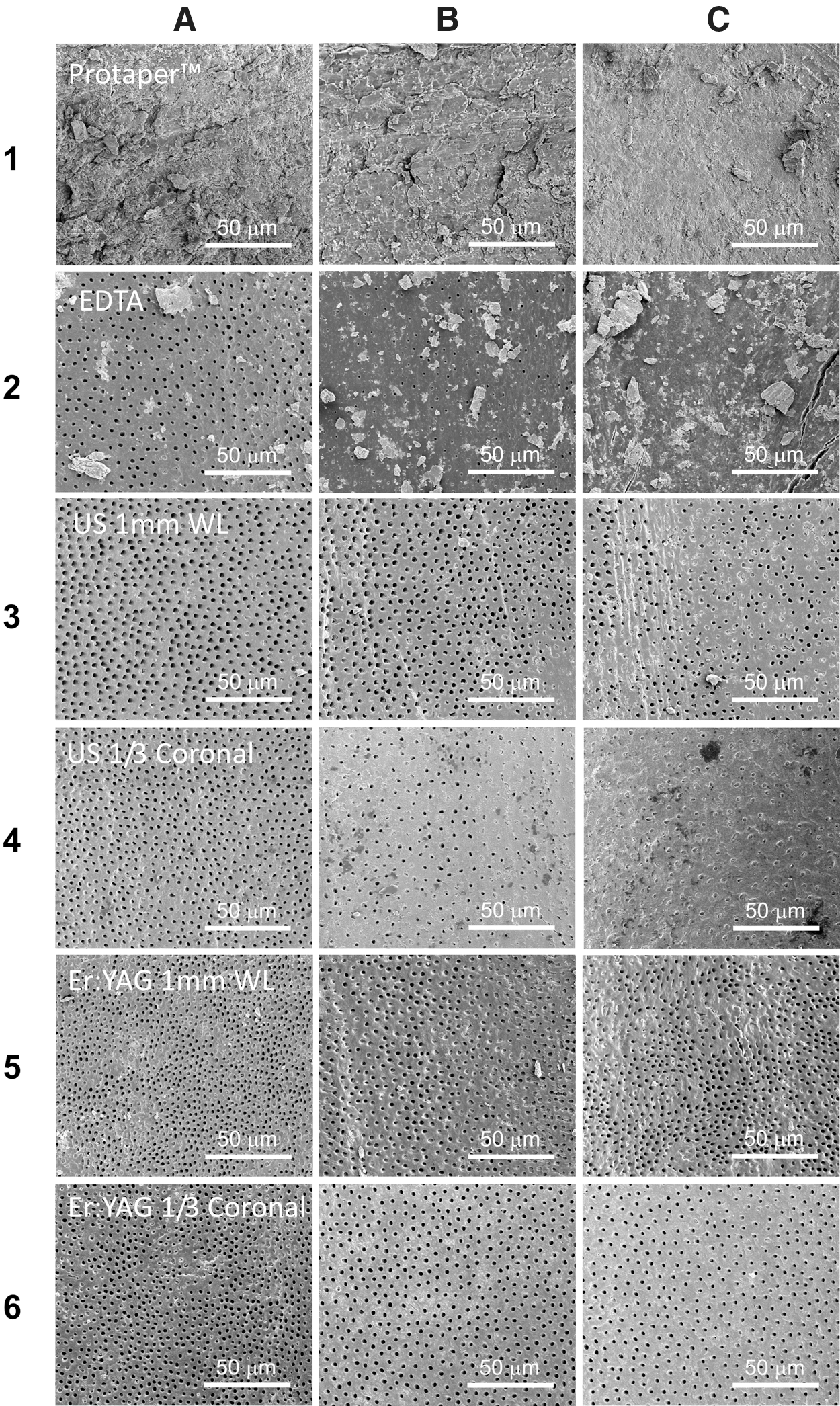
Comparison of the effects of positive-pressure irrigation, passive ultrasonic irrigation, and laser-activated irrigation on removal of the smear layer on the root canal surface.
Surface chemical analysis
The mean levels of Ca, P, and O and the Ca/P ratio in the surface dentin following irrigation with 17% EDTA alone, PUI combined with 17% EDTA, and LAI with 17% EDTA are shown in Figs. 2 and 3.
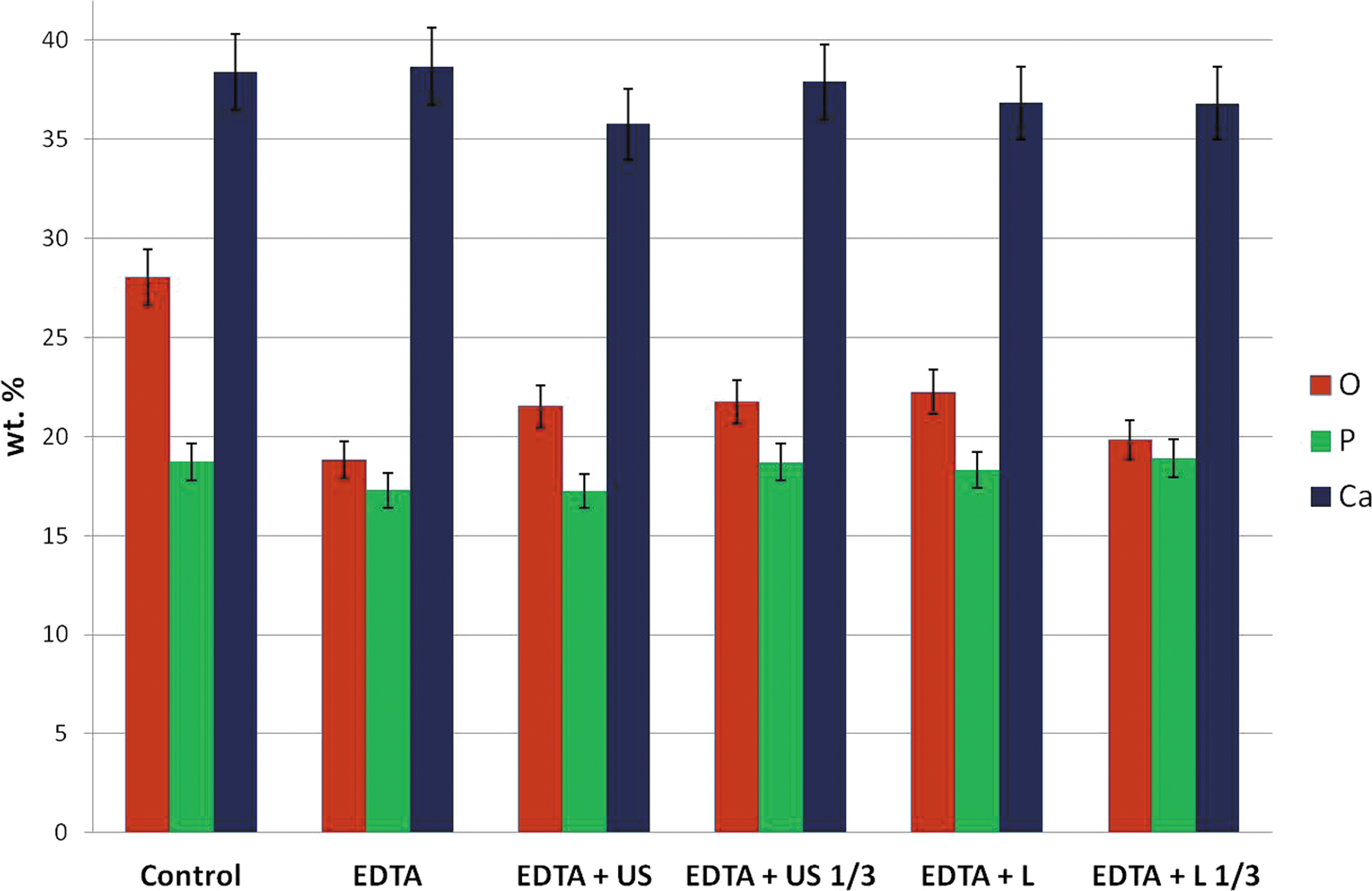
Mineral analysis of the root-canal surface after rinsing with irrigation solution alone, ultrasound irrigation with 17% EDTA, and Er:YAG laser activation with 17% EDTA.
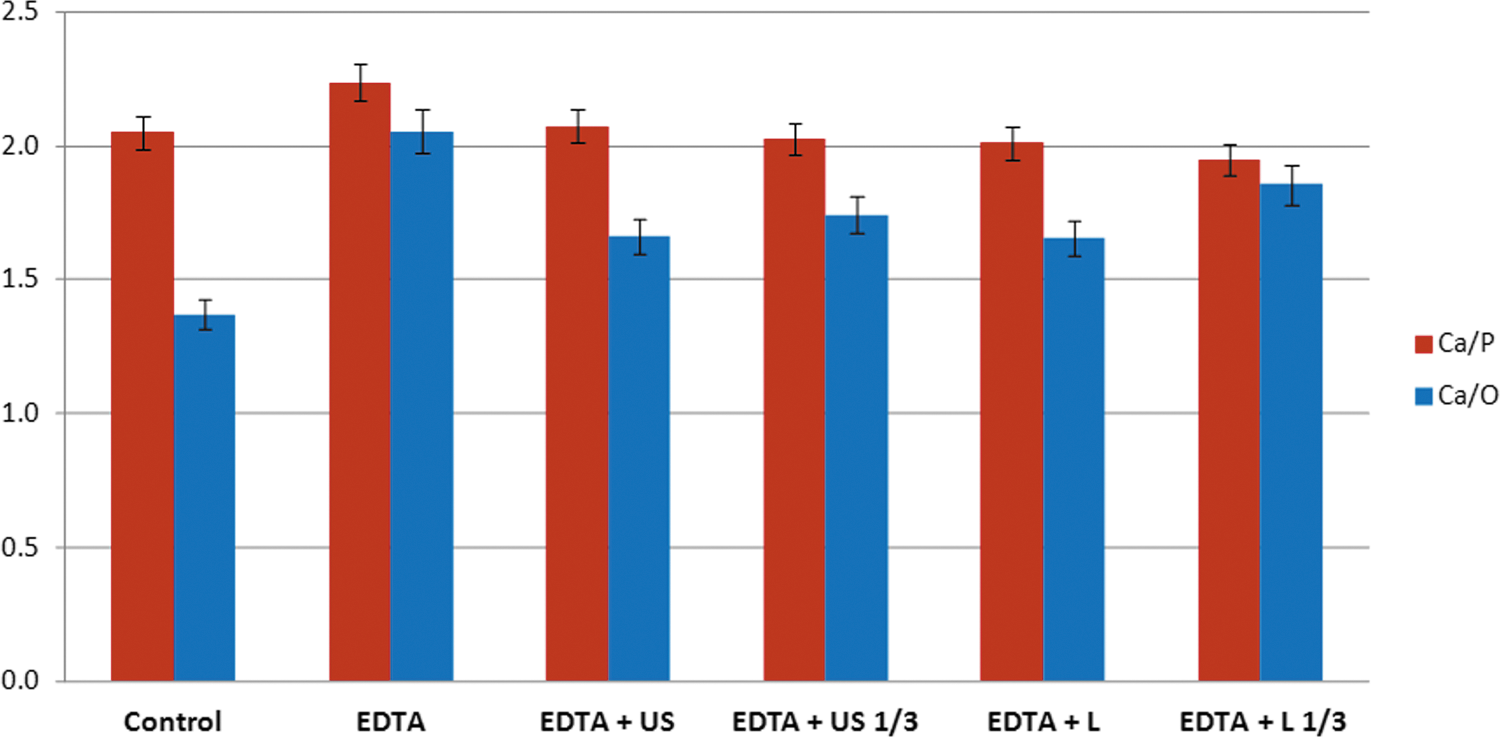
Changes in Ca/P and Ca/O in the root-canal surface after rinsing with irrigation solution alone, ultrasound irrigation with 17% EDTA, and Er:YAG laser treatment with 17% EDTA.
The control group had the highest levels of O; however, there were no differences in O levels among the treatment groups (Fig. 2). Changes in P levels in all groups compared with controls were small and statistically nonsignificant. There were no differences in Ca levels among the groups. The Ca/O ratio was highest in the 17% EDTA group, and lowest in the control group (Fig. 3). None of the differences in dentin surface mineral distribution were statistically significant.
Discussion
This ex vivo study was designed to evaluate the effectiveness of using a 17% EDTA irrigation solution with laser irradiation or with an ultrasonic device to remove the smear layer from root canal surfaces. These techniques were also compared to conventional syringe irrigation. Intact teeth were used to simulate the clinical situation as closely as possible. The maximum irrigation time was 1 min, to minimize detrimental effects on the dentin surface. The chemical constituents of the dentin wall of the root canal play a role in determining the success of the treatment, as demineralization may affect canal and tooth structure. Prolonged application of the EDTA solution might increase Ca2+ removal from the root dentin. Laser application, with or without EDTA, may also affect chemical composition of the dentin, leading to tubular erosion. 25,26 There are conflicting results as the duration of irrigants used in root canal treatment. One study suggests leaving a demineralizing agent in the root canal for at least 15 min to optimize cleansing, 27 whereas Ozdemir et al. 28 recommend avoiding extended treatment times because of excessive demineralization and erosion. Others have shown that EDTA solution removes the smear layer within 1 min of reaching the canal surface. 29 In our study, exposure to 17% EDTA was limited to 1 min to prevent potential changes in the dentin's microhardness, permeability, and solubility characteristics. 30
The standard irrigation technique during endodontic treatment employs a syringe and needle. Its effectiveness is unpredictable in the apical part of the canal, because the solution is only effective 1.5 mm beyond the needle tip. 31,32 The depth of needle penetration depends upon the size and morphology of the canal. 32 The results of the present study confirm that 17% EDTA irrigation with a syringe does not affect the apical segment of the root, and that the smear layer remains intact on this important part of the root surface.
Wu et al. 33 demonstrated that canal instrumentation alone leaves large portions of the canal wall untreated. One way to overcome this problem is to increase the size of the apical preparation. 34 However, it is recommended to avoid enlarging the apical foramen to more than number 40 during the endodontic treatment, to minimize the risk of stripping, apical transportation, and weakening of tooth structure. 35
Agitation techniques improve cleaning efficacy mechanically and chemically by enhancing irrigation dynamics. 36 The induced acoustic streaming directs jets of irrigant toward the root canal wall. Ultrasonic-activated irrigation removes debris, pulp tissue, and the biofilm from the canal wall via the shear stress produced by the acoustic streaming of the irrigant. 19 Jiang et al. 37 showed that dentin debris can be removed from the canal wall at 0.5 mm beyond the file tip, and that the cleaning effect is positively related to ultrasonic intensity. However Malki et al. 38 showed that an ultrasonically oscillating file can remove debris up to 3 mm beyond the file tip. Furthermore, the root canal curvature had no influence on irrigant flow. In this study, PUI of the upper coronal third and 1 mm short of the WL was tested to mimic the clinical situation. Smear-layer removal even improved in the apical third when PUI was applied. Nevertheless, debris remained, and the effectiveness was found to be dependent upon insertion depth. Specifically, the smear layer was removed from the apical third, but the dentinal tubules in this area remained occluded, whereas the tubules in the coronal and middle thirds were open.
Numerous types of laser have been developed to increase treatment effectiveness. 39 Recently, lasers have been used for cleaning and disinfection. 40 The removal of dentin debris from the root canal using LAI was investigated with an Er:YAG laser (2940 nm) 20,41 and Er,Cr:YSGG laser (2780 nm). 21
All of these studies showed that LAI is significantly more effective in removing dentin debris from the apical part of the root canal than PUI or manual irrigation when the irrigant is activated for 20 sec. The effect was based on cavitations, and the laser was activated at subablative settings that do not damage the wall, and hence avoid ledge formation.
Ledges may cause the formation of large elliptical vapor bubbles that expand significantly from their original volume and implode, increasing pressure and driving fluid out of the canal. 42 When the bubble implodes after 100–200 ms, a vacuum develops and fluid is sucked back into the canal, inducing secondary cavitations. As a result, the laser has the effect of a fluid pump. 42,43 One of the considerable limitations of laser is creation of an intense bubble stream close to the apex of the root canal, which may result in overextrusion of the irrigant. 22 Peeters and De Moor were pioneers in measuring the pressure during LAI. Measurement of pressure changes during laser-activated irrigant by an erbium, chromium: yttrium, scandium, gallium, garnet laser. They demonstrated the creation of pressure in the root canal with present-day recommended LAI settings exceeding the capillary blood pressure. 44
To overcome this problem, we positioned the tip of the laser at the upper third of the coronal part of the root canal to overcome the possibility of extrusion irrigation solution beyond the apical area. The laser fiber is unidirectional emission of its beam. In conventional techniques, the entire canal wall must be exposed directly to the laser beam. 45 To maximize the area of exposure, the laser fiber is moved in a spiraling motion along the canal wall, keeping it as close as possible to the apex; however, this technique is not completely efficient.
Conclusions
In the current study, we examined the coronal, middle, and apical areas of root canals treated with of Er:YAG LAI at a wavelength of 2940 nm equipped with a 17 mm 400 μm sapphire tip. The laser tip was inserted 1 mm short of the WL (Group 5) or in the upper third of the coronal area (Group 6). A 17% EDTA solution was activated by the laser. The sapphire tip was placed centrally in the root canal, and did not contact the walls. The depth of penetration did not alter the effectiveness of the LAI.
Fluid movement may differ in canals that are not regularly conical. In other words, LAI with Er:YAG laser is the most efficient method for removing the smear layer from the entire root canal wall. Working with the laser at the WL or in only the coronal third was equally efficient at removing the smear layer from the entire canal and superior to the other techniques examined.
Footnotes
Acknowledgments
This study was upported in part by the Hebrew University–Hadassah joint grant.
Author Disclosure Statement
No competing financial interests exist.