
Abstract
Introduction
D
Several modalities have been tried, with varying degrees of success, in the treatment of hypersensitive dentine. Laser systems are now discussed for their possible use in reducing DH. The neodymium-doped: yttrium, aluminium and garnet (Nd:YAG) and CO2 lasers are the most widely used, because of their property of causing melting and resolidification of superficial dentin, 4 although the erbium-doped: yttrium, aluminium and garnet (Er:YAG) laser with low power settings can also be used, because of its thermomechanical ablation mechanism and the high absorption of its wavelength by water. 5 –8
A new subspecialty in the medical and dental applications of lasers has developed, especially over the last decade, depending upon the therapeutic, rather than the surgical, applications of the laser. Low-level lasers have been widely investigated because of their low cost compared with other lasers, and their simplicity of use. The first low-level laser introduced was helium-neon (He-Ne), which combined a gaseous mixture to produce a wavelength in visible spectrum (632.8 nm) and low power output (5–30 mW). Because the wavelength produced by He-Ne was highly absorbed by soft tissues, its penetration was limited. Therefore, new diode lasers [galium, aluminium, arsenide (GaAlAs), indium, gallium, arsenide, phosphorus (In:Ga:As:P)] were introduced with slightly higher output and a wavelength that could penetrate the soft tissues without damaging them.
Two types of low-level laser therapy (LLLT) are present, simultaneous, and pure. The nondestructive thermal and nonthermal bioactivation occurs at the periphery of the target tissue; this is “simultaneous LLLT.” The laser systems that deliver power and energy densities below the destructive level, only to activate the irradiated tissue are “pure LLLT.” 9
The low-level or “soft lasers” provide cold thermal low energy wavelengths, with little temperature increase: <0.1°C. Low-level laser (400–900 nm) wavelengths have biostimulatory and biomodulatory effects. 10 –15 They are believed to stimulate circulation, increase cellular activity, increase vascularity, and provide analgesia, anti-inflammatory action, and accelerated tissue healing. 16 They mainly act on cell mitochondrial respiratory chain and membrane Ca channels. In accordance with this, several research studies have reported on the effect of LLLT on DH using GaAlAs laser therapy. 17 –19 The effect of LLLT in reducing pain has already been established, 18 which is related to the depolarization of c afferent fibers. 10,18,20,21 However, the effect of LLLT in reducing postoperative DH and pain following open flap debridement has attracted less attention. Therefore, the aim of the present study is to assess the effect of low-level laser in reducing DH and pain following periodontal flap surgery.
Aim and Objective
This randomized controlled double-blinded split-mouth study sought to compare DH and pain after 660 nm laser irradiation to test and control sites following periodontal flap surgery.
Materials and Methods
Thirty patients with chronic generalized periodontitis attending the Department of Periodontology, M. A. Rangoonwala Dental College and Research Centre, Pune, were selected for the study. There were 14 males and 16 females, between 23 and 56 years of age (mean age 36 years).
Inclusion criteria were: Having chronic periodontitis with a minimum of two sites in each quadrant with probing pocket depth ≥5 mm bilaterally, after 1 month following phase 1 therapy. Exclusion criteria were: (1) smoking, (2) debilitating diseases, (3) being pregnant or lactating, (4) having taken nonsteroidal anti-inflammatory drugs (NSAIDS) or antibiotics in the past 3 months, (5) having carious lesions, (6) having had desensitizing therapy during the last 6 months, (7) having cervical fillings, or (8) gingival recession. The purpose and design of the investigation were explained to patients and an informed consent form was signed. The study was performed according to a split-mouth design. Using a coin toss, 30 sites were randomly assigned for laser irradiation (test site) and the other 30 sites served as control sites. Thorough scaling and root planing were performed as part of phase 1 therapy, and patients were advised to use 0.2% chlorhexidine mouth rinses for 2 weeks. Patients were recalled after 4 weeks. Persistent pockets of ≥5 mm at minimum of two sites in each quadrant were scheduled for flap surgery.
The surgical procedure was performed by an experienced examiner. The measurements for assessing DH and pain were performed by a calibrated examiner who was trained to record the sensitivity patterns on a group of 10 patients who were diagnosed with DH at the Department of Periodontology, M. A. Rangoonwala Dental College. The intraexaminer weighted κ value was calculated by assessing the baseline values and re-examining the patients (κ=0.73).
The study was double blinded such that the subjects and the calibrated examiner performing the measurements were blinded to avoid bias. The approval of the Local Ethics Committee of M. A. Rangoonwala Dental College and Research Centre was obtained.
The surgical procedure was performed with the patient under local anesthesia (1:200,000 dilution) (Lignocad ADR (1:200,000), Cadila, Ahmedabad). An access flap technique was designed with intrasulcular incisions with a no.15c blade. Following debridement, the flap was repositioned to the presurgical level, and approximated with 4-0 silk sutures (Ethicon 4-0 Black Braided Silk Sutures, NW 5000, Johnson and Johnson Ltd, Himachal Pradesh). 22 Control sites were scheduled for the same procedure after 1 week.
GaAlAs laser (DR. Laser 200, 10DL001, KONDI Electrical Deposit Corporation, Hungary) (200–660 nm, 25 mW), 23 a semiconductor diode laser with a wavelength in the visible red spectrum (660 nm), and the average output power of 25 mW was used in sweeping motion for 3 min. 21,23 The irradiation was focused on the marginal gingiva at a distance of 3 cm, 23 and the spot area was 2.2 cm2 with a resultant power density of 11.36 mW/cm2. Laser irradiation was performed for the first 3 days following periodontal flap surgery 24 over the tissues on the test site. 25 All the laser parameters used for the treatment are described in Table 1. On the control sites, the laser was used as a placebo. Although it was placed on the marginal gingiva and was used in the similar motion, it was not activated.
Verbal rating scale (VRS) and visual analogue scale (VAS) were used for pain and DH assessment on 1st, 3rd, 5th, and 7th day after the surgery for both the sites. The VAS scale consists of a horizontal line, 100 mm long, anchored at the left end by the descriptor “no pain” and at the other end by “unbearable pain.” The patients were asked to rate their pain according to the scale. The distance of this point in millimeters from the left end of the scale was recorded and used as the VAS score. 23 VRS, a four point scale where 0=no pain, discomfort, 1=mild pain/discomfort, 2=marked pain/discomfort, 3=marked pain/discomfort lasting for >10 sec was also used. Air blast (thermo evaporative stimuli) with an air syringe at a distance of 1 cm from the site was used on test and control sites for 1–2 sec for assessing DH. 26
Statistical analysis
All the data were entered into a personal computer in Microsoft Excel sheet. Descriptive analysis was performed using SPSS software version 19. Data were analyzed using Mann–Whitney U test and Wilcoxon signed rank test. Mann–Whitney test to compare the difference between the median of the VAS and VRS between the test and control sites, and the Wilcoxon sign test to assess significant differences between the 1st and the 3rd, 5th, and 7th days.
Results
All the patients attended the follow-up sessions. The median of the VAS and VRS indexes for DH was obtained from thermal-evaporative stimuli. A Wilcoxon signed rank test was used to assess DH, and pain scores between the 1st day of treatment and the 3rd, 5th, and 7th day in all the sites. Mann–Whitney U test was applied to compare the difference between the median of VAS between the test and control sites. The percentage change in DH at the test site was higher (75.0%) than at the control site (55.0%) (Tables 2 and 3 and Fig. 1). The pain scores at day 1 did not differ significantly between the test site and the control site as assessed by VAS (p=0.105) compared with day 3 (p=0.015) and day 7 (p=0.001) (Table 4). Analysis of data showed statistically significant differences in VAS for pain on the test site on day 7 (p=0.005) compared with day 3 (p=0.004) of treatment (Table 5 and Fig. 2). Mann–Whitney U test was also applied to compare the difference between the median of the VRS between the test and control sites for DH and pain. There was a significant drop in VRS score for DH on the test site on the 7th day compared with the 1st day (p=0.006). Also, the average day 3, day 5, and day 7 DH scores were significantly higher in the control site than in the test site (p<0.05) (Tables 6 and 7 and Fig. 3). There was a 100% reduction in pain score observed on the test site compared with 66.7% on the control sites at day 7 (Table 8). Analysis of data showed a statistically significant differences in VRS for pain on the test site on day 7 (p=0.003) compared with day 1 (p=0.007) of treatment (Table 9 and Fig. 4).
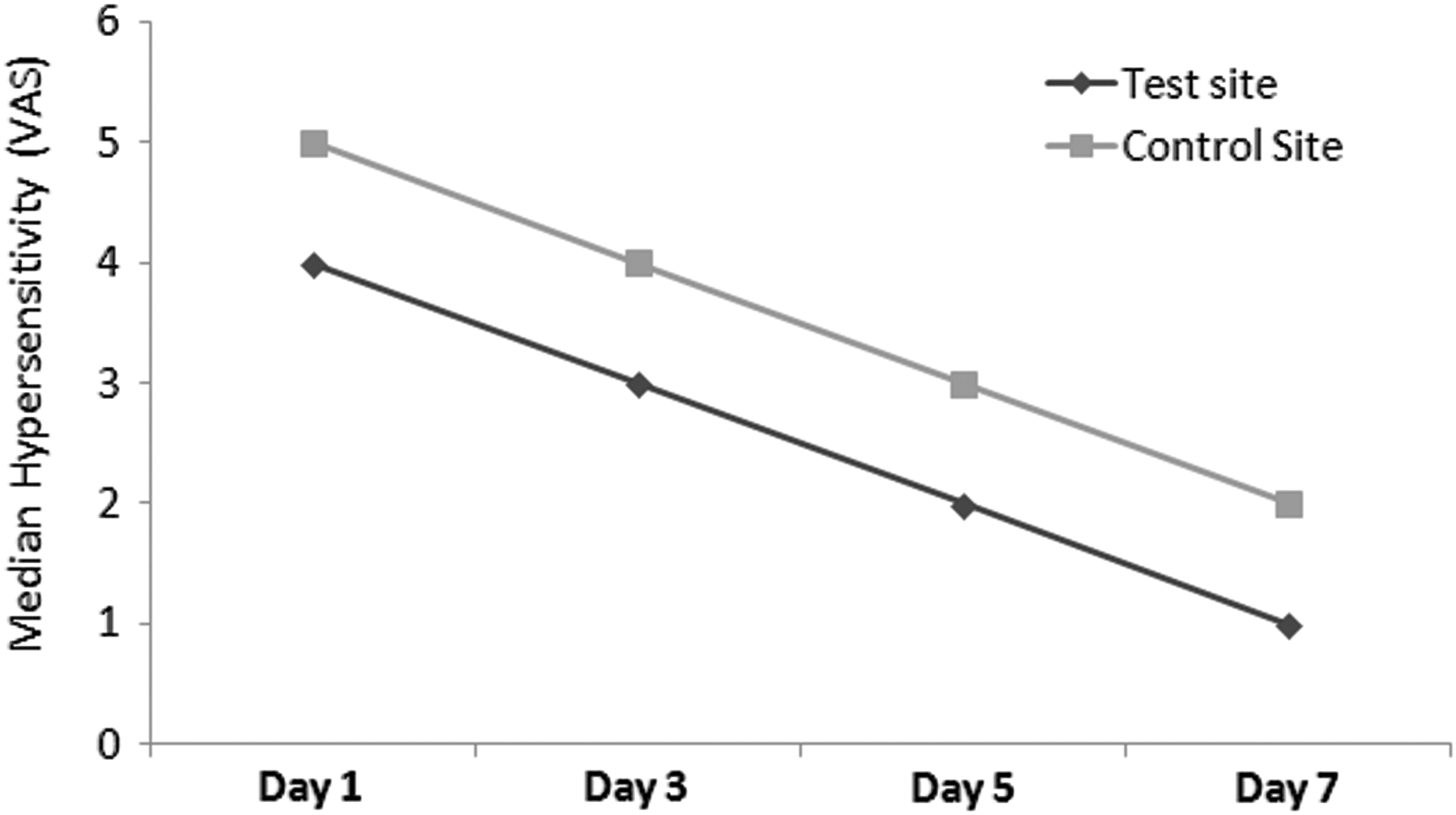
The intergroup dentinal hypersensitivity score [visual analogue scale (VAS)].
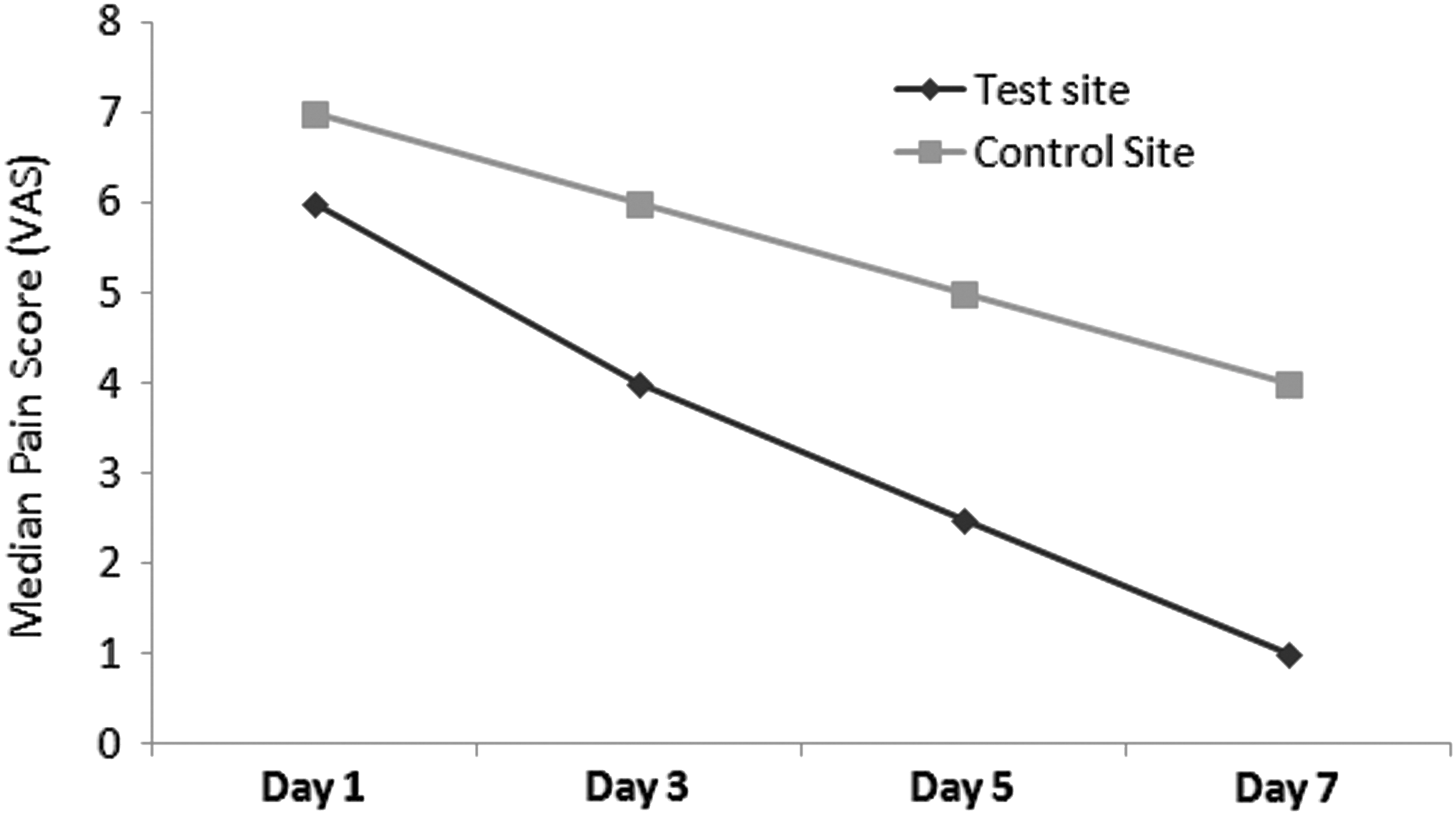
The intergroup distribution of pain score [visual analogue scale (VAS)].

The intergroup dentinal hypersensitivity scores [verbal rating scale (VRS)].
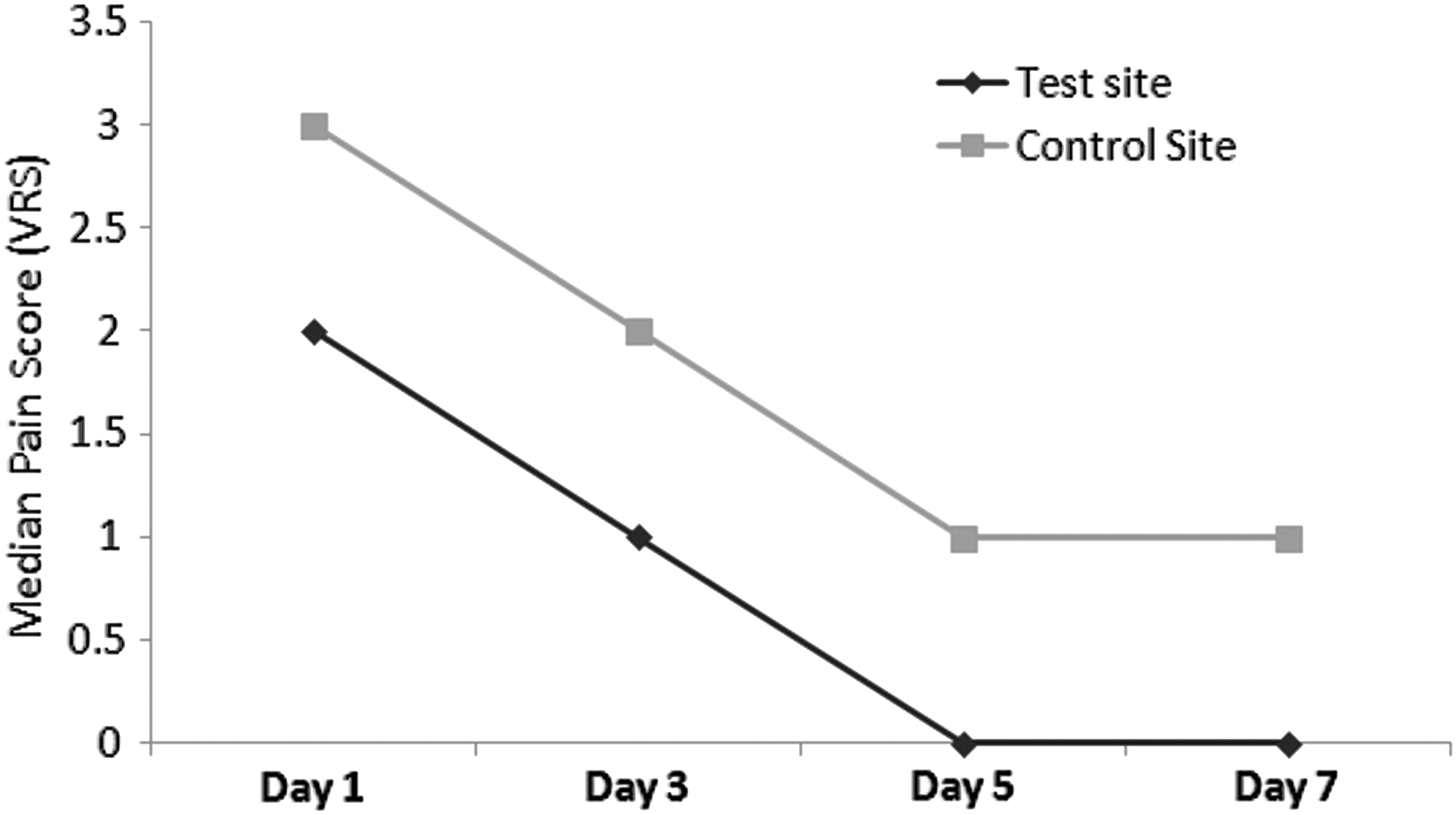
The intergroup distribution of pain score [verbal rating scale (VRS)].
Values are median (minimum–maximum).
p value<0.05 is considered to be statistically significant.
Discussion
Postoperative DH is one of the most frequent complaints following repeated scaling, root planing, 10,27 and periodontal flap surgery, especially during the 1st week and month. DH can be a major problem for periodontal patients, who frequently have gingival recession and exposed root surfaces. 10,28
The reported prevalence of DH following surgical therapy was 76.8–80.4% after 1 day, 29 36.8% after 1 week, 33.4% after 2 weeks, 29.6% after 4 weeks, and 21.7% after 8 weeks. 30 Although the removal of root cementum should be kept minimal, root instrumentation exposes dentinal tubules to the oral environment, thus exposing the dentin to a variety of bacterial, chemical, and mechanical stimuli. 31 DH usually reduces within a few weeks or months by formation of secondary dentin and natural occlusion of tubules by intertubular dentin. 32,33 This process can be supported by special toothpastes or mouth rinses containing desensitizing agents such as calcium hydroxide, potassium nitrate, strontium chloride, fluorides, and hydroxyapatite. Furthermore, DH can also be reduced by dentin bonding agents. 33
Pain is another postoperative complaint among patients; 77–90% of patients experience some degree of pain following scaling and root planing, and the average duration of moderate to severe pain is 6.1 h. 1,29 Periodontal surgery may also cause more pain and DH than scaling and root planing alone. 34 Open flap debridement surgeries cause pain in 79% of patients, whereas 89% complain of pain after gingivectomy and 93% complain of pain after flap surgery with osseous resection. Postoperative pain perception may be influenced by age, procedure modality, duration, location, extension, and degree of anxiety. 29,34
The advent of dental lasers has raised another option for the treatment of DH, and has become a research interest in recent decades. 17,19,33,35 Low-level lasers are widely used in dentistry because of their effectiveness in improving the healing process; lowering pain after surgery; and treatment of parasthesia, sensitive teeth, and many other painful conditions, in addition to promoting a faster dentin formation, and they are mostly recommended in periodontology to reduce the patient's complaints and discomfort caused by DH or pain after surgical procedures. 36,37
The present study tried to verify the effectiveness of the low-level laser irradiation for reduction or remission of DH and pain following periodontal surgeries. VAS and VRS were used to determine the amount of DH and pain following the treatments. There are many studies in the literature that have applied VAS as a reliable criterion for the presence and/or severity of pain after surgical procedures. This criterion is easily recognized by patients, and is sensitive and appropriate for evaluating the pain. 36 –38
The results of this study indicated that 660 nm LLLT has both desensitizing and analgesic action. There was statistically significant reduction in hypersensitivity between the laser-irradiated and control sites (p<0.05). Many studies have used GaAlAs laser treatment, and have demonstrated desensitization of hypersensitive cervical dentine, with an efficacy rate of ∼90%. 17,39,40
Various mechanisms have been proposed that elicit the effectiveness of low-level GaAlAs laser in decreasing DH. 23 The morphological analysis of dentin surface using scanning electron microscopy revealed that Nd:YAG laser irradiation causes melting and fusion of dentin, and, therefore, the closure of exposed dentinal tubules. 41 Nevertheless, some authors believed that the low-level laser caused depressed nerve transmission in the neural networks within the dentin. 12 Also, histological studies have reported that hard tissue formation is enhanced as a reaction of dental pulp to laser light. 38,39 Stimulation of odontoblasts, production of reparatory irregular dentin, and obliteration of dentinal tubules provoked by laser may be the reasons for the prolonged suppression of DH. 42 Some studies have found no significant difference between the low-level laser and placebo groups for reducing DH. 43
Reduction of pain following application of laser may be the result of the property of faster wound healing. This may be because of an increase in the movement of keratinocytes and acceleration in epithelialization caused by increased fibroblast proliferation and neovascularization. 44 Another study demonstrated that the secretion of fibroblast growth factor by macrophage and fibroblasts is increased following LLLT. 45 Laser effects on endorphin release could be the reason for the immediate pain relief in patients, but biostimulative effects happen gradually in a few days. In addition to the immediate analgesic effect, laser therapy used with correct parameters may stimulate the normal physiological cellular functions. Although information on the neurophysiological mechanism is not conclusive, it is postulated that a low-level laser mediates an analgesic effect related to the depolarization of C fiber afferents. 10,20,21 This interference in the polarity of cell membranes by increasing the amplitude of the action potential of cell membranes can block the transmission of pain stimuli in hypersensitive dentin. 42
In the present study, a clinical and statistically significant reduction was observed over time in DH for the laser-treated sites. It is generally accepted that tooth sensitivity may decrease with time as a result of the natural occlusion of tubules. 46 In the literature, there are many contradictory studies for the treatment of DH using low-level lasers. 19,22,47 –50 These differences are caused by the fact that there are various types of lasers and variety in laser parameters. Several other factors could have influenced results, such as surgical extension (number of teeth involved), time required to perform the surgical procedure, gingival inflammation grade, and number and severity of periodontal pockets. These variables were not possible to control during the study. Also, the laser beam was aimed and focused on the marginal gingiva of each tooth and not on the exposed dentin. It should be kept in mind that because of the controversies in information regarding the mechanism of the effects of low- level lasers in the treatment of DH, and the fact that the treatment procedure is not simple because of the interference of natural desensitization of teeth, mechanical occlusion of the exposed dentinal tubules by smear layer, or creation of secondary dentin, we still need more studies for investigation in this field, with longer follow-up periods, to assess long-term effects of LLLT.
Conclusions
The present study has demonstrated that the low level GaAlAs laser therapy could be a suitable tool for successful reduction of postoperative dentine hypersensitivity and pain. Further studies are needed in order to evaluate the long-term stability of the obtained positive results; especially, the mechanism of laser-induced desensitization should be investigated in subsequent studies.
Footnotes
Author Disclosure Statement
No competing financial interests exist.