
Abstract
Introduction
M
Muscle fatigue, or decline in performance, will be dependent upon several factors, including type of muscle fibers recruited during exercise, and intensity and duration of the activity. 3 The most common explanation for muscle fatigue is an accumulation of hydrogen ions that impairs contractile function. Alternative explanations have considered effects of ionic modifications on muscle action potential, such as the presence of inorganic phosphate (Pi) and magnesium ion, lack of Ca2+ or its releasing from different mechanisms, and effects of reactive oxygen species (ROS). 1 Furthermore, some strategies have identified the intensity of the muscle fatigue process through lactate levels in blood, 2 functional performance, and electromyography (EMG) activity. 4,5 These assessments can provide overall responses about muscle recruitment and contraction. In this context, the root mean square (RMS) and median frequency (MF) are two EMG parameters commonly used to infer muscle fatigue. 4,5
Low-level laser (light) therapy (LLLT) interacts with biological tissues 6 and has been used to treat pain and promote tissue healing. 7,8 Moreover, recently, LLLT has been used successfully to decrease muscle fatigue in experimental models and clinical trials. 9 –11 Muscle fatigue resistance can be increased with LLLT if applied before (muscular preconditioning) or after intense exercises (muscle recovery), increasing tetanic contractions and maximum repetitions (RM) using fitness equipment or free weights. However, these LLLT benefits to biological tissues are controversial, possibly because of a possible biphasic dose-response, which has been already reported in the literature. 12,13
With these perspectives in mind, some authors suggested that LLLT associated with exercise training can reduce muscle fatigue. 10,14,15 On the other hand, few studies applied LLLT to skeletal muscles during rest intervals of intense exercise. 16,17 Moreover, few studies have investigated LLLT's effects on muscle fatigue resistance using EMG analysis. 18,19 and no study has combined LLLT's effects on EMG in isokinetic exercises.
The purpose of this study was to analyze LLLT's effects on muscle fatigue resistance of the quadriceps femoris muscles during RM of knee flexion-extensions using an isokinetic dynamometer, in conjunction with EMG analysis (MF).
Material and Methods
This study was approved by the Research Ethics Committee of the Federal University of Rio Grande do Norte (CEP/UFRN, protocol 401/09) and registered at ClinicalTrials.gov (NCT01972100). All participants who agreed to participate in this study were registered, received basic information about the objectives and procedures of the study, and signed a consent form in accordance with the Declaration of Helsinki.
Seven men aged 21±3 years with body mass index (BMI) of 22.6±2.1 kg/m2 were enrolled in this study. These volunteers were classified as clinically healthy using the Physical Activity Readiness Questionnaire (PARQ) for physical activity. Smokers or those using anti-inflammatory drugs or any drugs affecting normal physiological conditions were excluded. In addition, volunteers with lower limb lesions limiting flexion-extension of the knee joint were also excluded. All participants were instructed do not do any physical exercise or drink alcohol.
Study design and randomization
This study was randomized, crossover, and double-blinded with placebo. Randomization procedure was performed by a simple drawing, to set an order to apply all treatments: active laser (LLLT) or placebo laser (Placebo). Therefore, if a participant received active laser (LLLT) during the first week of evaluation and exercises, the third week (including here 1 week of washout period) was placebo LLLT, and vice versa. This study design made it possible to decrease the variability between volunteers and duplicate the number of subjects in this study: seven plus seven as a result of the crossing procedure between groups (Fig. 1).
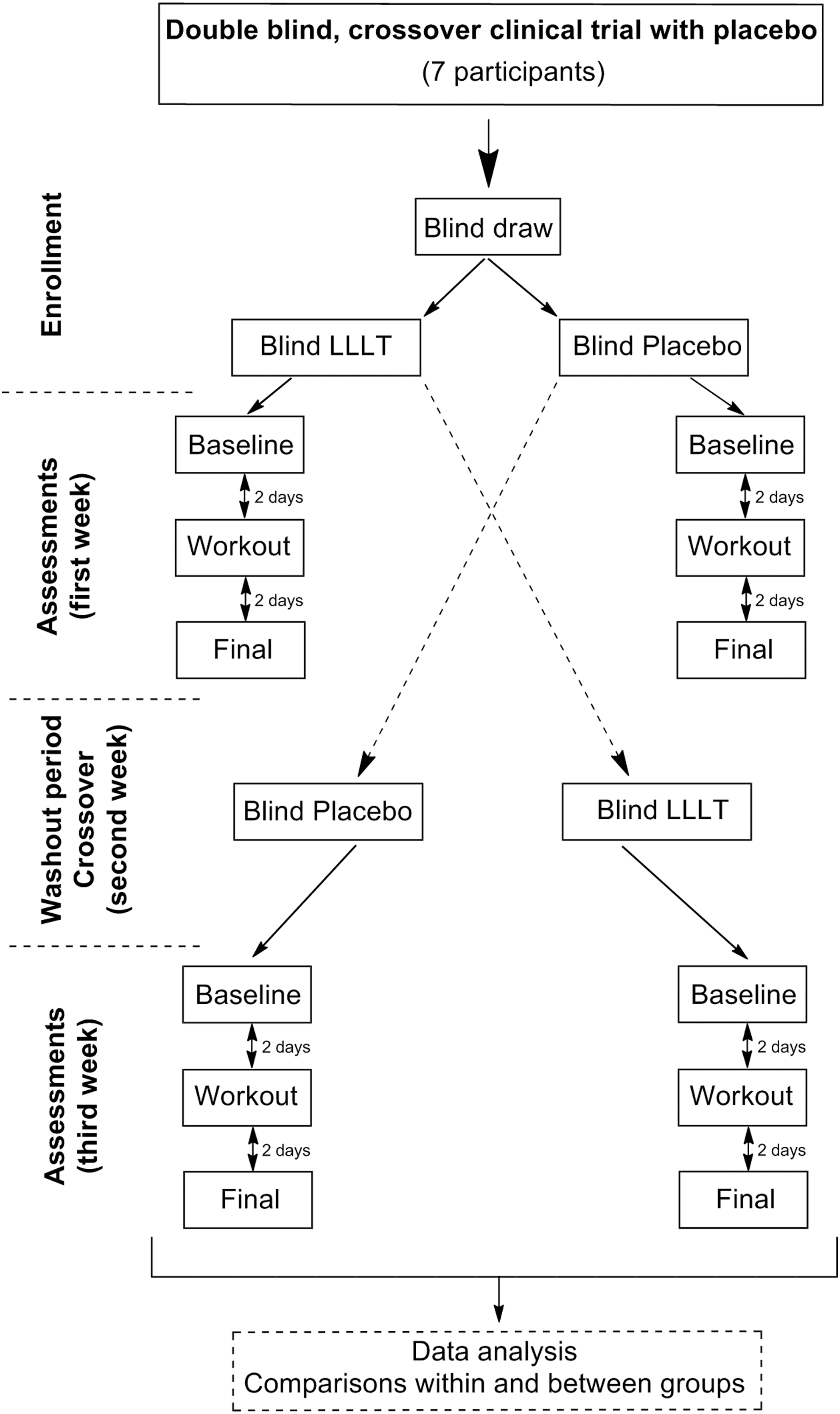
Flow chart of the study. LLLT, low-level laser therapy.
A technician conducted the drawing procedures without communicating to participants and evaluators which therapy (LLLT or Placebo) would be applied on muscles. Thus, participants and evaluators were blinded to the allocation of treatment. Participants, evaluators, and technicians used opaque goggles during LLLT procedures in order to protect their eyes from LLLT (active or placebo) irradiation.
Procedures
Volunteers were recruited from gyms in Natal city, RN, Brazil. All volunteers attended this study for 3 consecutive weeks. At the 1st and 3rd weeks all volunteers were evaluated three times with 2-day intervals between each day to assess the following.
Baseline
Electromyography fatigue index (EFI) was recorded using MF signal of the rectus femoris (RF), vastus medialis (VM), and vastus lateralis (VL) muscles during RM of knee flexion-extension using an isokinetic dynamometer (Fig. 2). This evaluation was conducted until voluntary muscle fatigue or exhaustion, which was understood to be the inability of the volunteer to maintain the exercise or when the volunteer decided to stop.
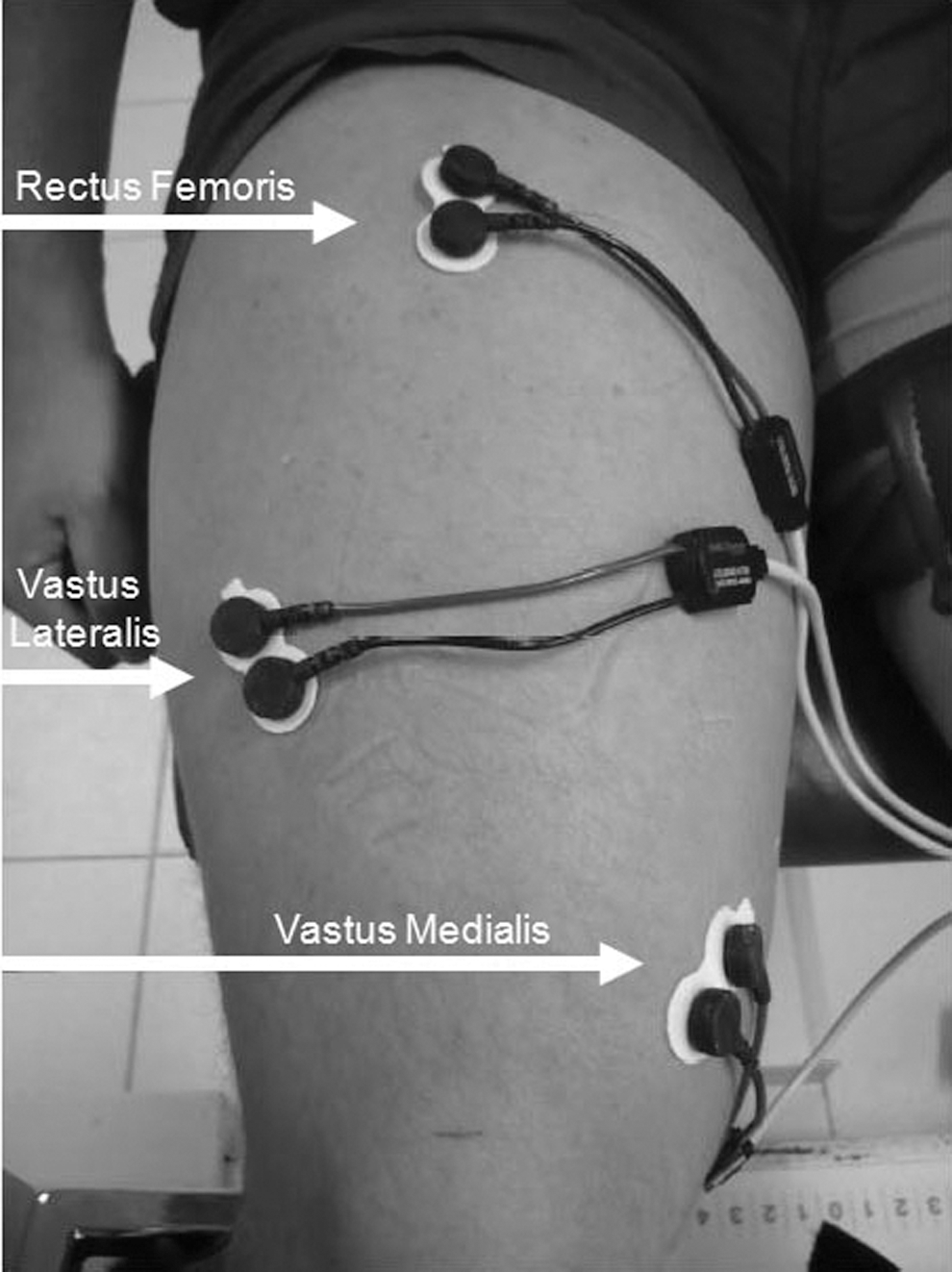
Position of the surface electrodes on the vastus medialis, vastus lateralis, and rectus femoris muscles during electromyography fatigue index assessment.
Training session (workout)
Workout comprised three sets of 20 maximum repetitions of knee flexion-extension at 60 degrees/sec using an isokinetic dynamometer. During rest intervals (between sets of exercise), LLLT or Placebo was applied perpendicularly on the quadriceps femoris muscles exactly over the same points where electrodes were placed for EMG records of RF, VM, VL, and two other points on the RF muscle distributed at 3 cm below and 3 cm above of the first point (Fig. 3). A rest interval of 4 min between each set of exercises was established for all groups, in order to make it possible to apply LLLT or Placebo.

Active or placebo low-level laser therapy applied on the vastus medialis, vastus lateralis, and rectus femoris muscles (white circles).
Final evaluation
A final evaluation was conducted 2 days after the training session, with the same procedures described for baseline evaluation.
During the 2nd week there were no exercises or evaluation; that is, it was a washout period 20 needed to cross participants between groups: LLLT to Placebo, or vice versa (Fig. 1).
During baseline evaluation, training session (workout), and final evaluation all volunteers received loud oral incentives from the evaluator to apply maximum effort. Evaluators and all volunteers were blinded to laser procedures.
Instruments
RM was assessed using an isokinetic dynamometer (Medisa®, Spain). For acquisition and processing of the EMG signal during the isokinetic test, we used a signal conditioning module (MCS 1000) with four channels (EMG System of Brazil) and an analog-digital converter (A/D) (CAD, 12/36-60K) with a resolution of 12 bits. This equipment has a ratio of common mode rejection>80 dB, a signal sample of 1000 Hz, and a frequency range between 20 and 500 Hz. As the programmed gain is set to 50 times, signals were amplified 5000 times. The software used was EMGLab (EMG System of Brazil, Brazil) which calculates the MF by fast Fourier transform. Self-adhesive surface electrodes were used and separated by a standardized distance of 2 cm with an internal gain of 20 times. An oval reference electrode was placed on the malleolus of the unassessed lower limb.
RM using the isokinetic dynamometer and EFI evaluations
RM using the isokinetic dynamometer was evaluated at 60 degrees/sec until exhaustion or fatigue; that is, at the moment that participants were not able to keep muscle contraction throughout a preset range of motion (75 degrees of knee flexion-extension) or when the participants made a voluntary decision to stop. Volunteers were positioned and stabilized with belts on the chair in order to avoid compensatory movements. Next, they performed a pre-test to familiarize themselves with the isokinetic machine. Afterwards, the RM test was started and recorded the number of RM and the EMG signal of the MF concomitantly.
For MF signal, markings were made on the quadriceps femoris muscles to place all electrodes. Next, the skin was shaved and cleaned with alcohol. For the RF muscle, electrodes were placed at the point corresponding to 50% of the distance between the anterior superior iliac spine (ASIS) and upper margin of the patella. For the VM muscle, electrodes were placed at the point corresponding to 20% of the distance between ASIS and the knee joint at the medial side. For the VL muscle, electrodes were placed at the point corresponding to 33% of the distance between ASIS and lateral side of the patella. All these points were used as recommended by Surface Electromyography for the Non-invasive Assessment of Muscles (SENIAM) 21 (Fig. 2). The reference electrode was placed on the medial malleolus of the unassessed lower limb. Electrodes were attached to the skin with adhesive tape and elastic bands to ensure stability. In addition, heart rate (HR) was recorded at rest and during maximal effort; that is, the moment that volunteers stopped the test or were not able to keep muscle contraction throughout a preset range of motion.
The maximum number of RM performed at baseline and final assessments were used as comparisons within groups. Percentage differences between maximum number of RM performed at baseline and final assessments of each group were used for comparisons between groups.
EFI was calculated from the average of the MF signal in Hertz (calculated by fast Fourier transform) of the first five and last five RM using the isokinetic dynamometer. EFI analyses used the MF signal of the final evaluation related to the same number of RM performed at baseline evaluation.
Percentage decay of MF signal (decay %) from baseline to final assessment was used to verify EFI within groups. Delta (Δ) of the percentage decay of MF signal of all muscles tested (RF, VM, VL) was used for comparisons between groups.
LLLT and placebo LLLT
A single technician applied active LLLT or placebo LLLT. No participants or evaluators knew which therapy was applied (double-blind procedures). A laser device (AsGaAl, λ=808 nm; Photon Laser Apparatus III; DMC® São Carlos, SP, Brazil) was used in this study with all parameters described in Table 1.
There were three applications (three times) at the training session (between sets).
LLLT was applied in contact mode and perpendicular to the belly of quadriceps femoris muscles at five equidistant points: three points on the RF; one point on the VM, and one point on the VL (Fig. 3). LLLT was applied on the dominant lower limb between the first and second, and the second and third, and after the last set of exercises (workout), totaling three applications (three times) on the same day. Placebo (laser off) followed the exactly the same procedures as those for active laser. However, the laser probe was not turned on; that is, the button that starts light irradiation was not pressed. In addition, the display of the laser device was covered and volunteers and evaluators used appropriate goggles for infrared light. LLLT was not applied on the quadriceps femoris muscles before or after the baseline or final assessment.
Sample size calculation
Sample size was calculated based on significant differences (in percentage) between groups related to the number of RMs performed using the isokinetic dynamometer at baseline and final assessments. Statistical power of 80% and large effect size (upper to 0.75) were set as satisfactory.
Statistical analysis
Data were expressed as means, standard deviations, and percentage of change related to baseline. Nonparametric statistic was derived using Wilcoxon and Mann–Whitney U tests for comparisons within and between groups, respectively. Nonparametric tests are more stringent, and were used because of the small sample size of this study. Statistical significance was set at 5% (p<0.05).
Results
Number of RMs
The LLLT group increased the maximum number of RM (p=0.027), whereas the Placebo group decreased them (p=0.027). In addition, LLLT developed more RM than the Placebo group (p=0.002). These results are summarized in Table 2.
Comparisons within and between groups measured by Wilcoxon test and Mann–Whitney U test, respectively.
Statistical significance (p<0.05).
% of RM, difference in percentage between baseline and final evaluation for the maximum number of maximum repetitions (RM) performed; ↓ or ↑, direction of the difference.
EFI
Both groups had significant decay in MF for all muscles, comparing pre and post evaluations at baseline and end-point (p=0.017) (Table 3).
Statistical significance (p<0.05) measured by Wilcoxon test.
%, percentage of decay in MF signal;↓or↑direction of the decay.
The LLLT group had a smaller increase (as a percentage) of EFI for the VM (p=0.027) and the VL (p=0.042) (Table 3), whereas Placebo had a larger increase (as a percentage) of EFI for the RF (p=0.023) (Table 3).
Comparisons between groups for EFI showed that the placebo group had a significantly greater EFI or decay in MF signal for the VM (p=0.004) and the RF (p=0.004). These results are summarized in Table 4.
Statistical significance (p<0.05) measured by Mann–Whitney U test.
%, percentage of decay in MF signal; ↓ or ↑ direction of the decay; Δ, difference in percentage between baseline and final results of the decay (%) in MF signal reported in Table 3.
HR
Comparisons of the HR between groups had no statistical significance (p>0.05). At rest at baseline, there was no statistical difference (p=0.734) between Placebo (91±18.9 bpm) and LLLT (94±14.4 bpm). At the maximum effort at baseline assessment, both groups presented similar results without statistical difference (p=0.588): Placebo (157±16.8 bpm) versus LLLT (160±17.6 bpm).
At rest at the final assessment, there was no statistical significance (p=0.294) between Placebo (88±9.7 bpm) and LLLT (94±7.2 bpm). At the maximum effort at the final assessment, both groups presented similar results without statistical significance (p=0.710): Placebo (155±16.7 bpm) versus LLLT (159±23.8 bpm).
Sample size
Statistical power and effect size for the maximum number of RM between groups (as a percentage) were calculated in order to ensure the minimal power of 80% and large effect size (upper to 0.75). Our results showed a difference between groups, with a statistical power of 84%, effect size of 2.15 (huge effect), and minimum of five volunteers allocated in each group or treatment. These calculations demonstrate that our sample size was small, but adequate.
For EFI, VM had a statistical power of 80%, effect size of 2.15, and minimum of five volunteers per group (sample size). RF had statistical power of 81%, effect size of 2.05, and also a minimum of five volunteers per group. The only muscle with no statistical significance between groups was VL. For this muscle, a minimum of 44 volunteers would be necessary to achieve a satisfactory statistical significance.
Discussion
Our method LLLT irradiation between sets of exercise and after the last series increased the maximum number of RM between groups with statistical significance. This difference was used as the main clinical result to investigate if EFI could be also modulated by LLLT.
The protocol of assessment used in this study aimed to assess the maximum number of RM with controlled velocity and range of motion, whereas previous studies had used free weights without accurate control of the movement. 18,19,22 However, peak torque, power, work or any other isokinetic results were not used in any analysis. The velocity of 60 degrees/sec was used in order to promote an important resistance to the movement (flexion-extension) and thus achieve maximal efforts during the test and exercise protocol. Maximum effort was very similar between groups, as can be seen through the absence of statistical difference in HR and a significant increase in EFI post-evaluation for all muscles in both groups when compared with pre-evaluation of the baseline or final. Moreover, the exercise protocol with three sets of 20 RMs at 60 degrees/sec was standardized, bearing in mind all statements of the American College of Sports Medicine, which suggest long-duration sets with high muscle time under tension and minimal rest recovery for local muscular endurance. 23
The literature has reported for several years that LLLT interacts with photoreceptors in the mitochondrial respiratory chain, promoting an increased enzymatic activity and flow of electrons, 6,9,24 which in turn increases adenosine triphosphate (ATP) synthesis. 25 Possibly, these effects can increase energy availability (ATP) and, consequently, optimize muscle work during exercises. 9,14,15 However, LLLT should penetrate deeply through the skin and achieve the muscles. For this reason, this study used an infrared wavelength (808 nm) that is inside of the best optical window to stimulate biological tissues, as has been reported previously. 12 This optical window suggest low absorptions of the light by skin, melanin, water, hemoglobin, and oxyhemoglobin for wavelengths between 600 and ∼1000 nm. 12
Ortenblad and Stephenson 26 reported that aerobic muscles under anaerobic conditions can release large amounts of ROS, leading to muscle fatigue. With these perspectives in mind, some authors performed a muscular preconditioning in intense and fatiguing tests using LLLT. 22,27,28 These authors hypothesized that a local action of LLLT possibly can prevent exercise-induced muscle damage and ischemic muscle injuries and reduce creatine kinase (CK) activity and ROS. Moreover, LLLT possibly can promote vasodilatation and, consequently, more oxygen and nutrients can be delivered to muscles, allowing better physiological conditions to perform muscle contraction.
The increased maximum number of RM in our study corroborates with previous results 22 that observed the same results after a single irradiation of LLLT (655 nm, 5 J, and 500 J/cm2) on the biceps brachii of volleyball players before a fatigue test. Leal Junior et al. 27 also reported that LLLT applied on football and volleyball players before an exercise session could reduce lactate and CK levels, suggesting that LLLT can delay the onset of muscle fatigue.
Another important result of this current study was the smaller increase in EFI when LLLT was applied over the quadriceps femoris muscles, decreasing the decay of the MF. The use of MF to infer EFI has been reported previously. 4,5 Decay in MF signal is related to reduced muscle blood flow, more muscle fatigue, and accumulation of lactate that may decrease muscle membrane excitation. 4 Therefore, MF can become a valuable tool to assess muscle fatigue in studies involving LLLT once this therapy can increase blood flow and microcirculation, decrease production of lactate, and promote a faster removal of this metabolite. 27,29
The smallest EFI in the VM and VL occurred only in the LLLT group (Table 3), and in the RF and VM in the LLLT group compared with Placebo (Table 4), which can be related to LLLT's effects on mitochondria, energy metabolism, and also to the dose of light (energy in J) applied on the RF. VM and VL muscles have good mitochondrial density because of the predominance of fiber types I and II, 30 which in turn are related to fatigue resistance. 1,2 This increased potential for fatigue resistance possibly could be stimulated by LLLT's effects on the mitochondrial electron transport chain and ATP synthesis, offering more energy to muscle contraction and recovery.
RF is the main muscle agonist of the knee extension in the open kinetic chain, 31 and for this, received three times more LLLT than VL and VM, whereas the placebo group significantly decreased MF signal for this muscle. Previous studies did not find significant effects of LLLT on muscle performance with EMG analyses. 18,19 However, these studies used only one muscular preconditioning, and, possibly, it was not sufficient to stimulate muscle cells. We believe that our protocol of LLLT applied over muscles between sets of exercise and after the last series possibly improved mitochondrial function, stimulated blood flow, decreased lactate production, and promoted its fast removal as reported previously. 27,29 In addition, LLLT possibly promotes positive modulations on the excitability of muscle fibers, as hypothesized by our research group previously. 9
The majority of the studies reported in the literature up to now have shown an improved muscle performance when LLLT is applied immediately (5 min) before a bout of exercise (muscular preconditioning). However, few studies reported LLLT's effects on muscle performance after 48 h of irradiation. 16 For this reason, this study had also this time as a purpose of investigation.
Acute and chronic exercise's effects on skeletal muscles are already well described in the literature. 32,33 These acute and chronic adaptations can be summarized as muscle hypertrophy, fatigue resistance, learning the exercise and consequently improved strategies of muscle recruitment, and muscle recovery, including management of inflammation. LLLT has been used to manage pain and inflammation, and repair biological tissue, and, recently, this therapy has shown good effects in preventing muscle damage in intense exercises 11 and accelerating muscle recovery. 9,10 We suggest that LLLT possibly protected against exercise-induced muscle damage and promoted a fast muscle recovery, based on the primary and secondary effects of the LLLT on biological tissue. 6
Some authors have suggested that stressed cells can produce better responses for LLLT, 9,14,15,34 corroborating the idea of our study with LLLT irradiation between sets of exercises (mechanical and metabolic stress) and after the last series. In summary, our findings are consistent with previous studies, 9,14,22,27,28 and contributes to literature reporting more effects and ways of LLLT irradiation to enhance muscle performance. However, as was already reported in previous studies, 27,35 the small sample size of participants enrolled in this study was a limitation, although adequate in accordance with the statistical power and effect size calculated.
Conclusions
Our study applied LLLT over quadriceps femoris muscles between sets of RM performed using an isokinetic dynamometer. After 2 days of LLLT irradiation, the final evaluation analyzed the maximum number of RM and EFI for the VM, VL, and RF. LLLT increased the maximum number of RM and reduced EFI for the VM and RF compared with the placebo group.
Our results suggest an extended time effect for LLLT in decreasing muscle fatigue. This result was possibly the result of exercise-induced muscle damage prevention, and/or fast muscle recovery promoted by LLLT. Our results can open a new window of investigation into time response for LLLT. In addition, our findings could be useful for high performance sports that require fast recovery and less fatigue.
Footnotes
Acknowledgment
Cleber Ferraresi would like to thank FAPESP (Fundação de Amparo à Pesquisa do Estado de São Paulo) for PhD scholarships (2010/07194-7 and 2012/05919-0).
Author Disclosure Statement
No competing financial interests exist.