
Abstract
Introduction
P
A broad array of proinflammatory macrophage and fibroblast cytokines, including IL-1, IL-6, IL-15, IL-18, TNF-α, various chemokines, and many soluble factors are essential in the inflammatory pathogenesis of RA. 1 These proinflammatory cytokines induce RA progression and in synergy, the production of high levels of matrix metalloproteinases (MMPs) by synovial cells and chondrocytes. 3 Therefore, proinflammatory cytokines have been widely interpreted to be involved in joint swelling as well as in joint inflammation and the cartilage and bone erosion through osteoclast formation and activation. 1 Therefore, downregulation of proinflammatory cytokines may be an appropriate therapeutic strategy for RA.
MMPs, the most important matrix-degrading enzymes in RA, act as key mediators of the resorption of cartilage, bone, synovial fluid, and adjacent soft tissue, which occurs as part of the pathological destruction of joint tissue. 4,5 Among dozens of MMPs, MMP3 (stromelysin 1) whose synthesis and activation is induced by proinflammatory cytokines, has been reported to be the major enzyme produced by synoviocytes, and the level of MMP3 is significantly higher in synovial fluids of RA. 5 –7
Studies have shown that low-level laser therapy (LLLT) is capable of acting on the inflammatory process in various joint inflammation situations. 8 –10 It can modulate proinflammatory mediators, thereby decreasing the expression of cytokines such as IL-1β, IL-6, and TNF-α, and it also can decrease the number of inflammatory cells (macrophages and neutrophils). 8,11 LLLT was introduced as an alternative noninvasive treatment for RA approximately two decades ago. The effectiveness of LLLT for RA is still controversial, and one of the reasons can be the inappropriate application of laser energy in some trials that revealed no beneficial effect of LLLT. 12
Therefore, this study aimed to evaluate the effects of LLLT at lower and higher fluences (LF and HF) of 4.5 and 72 J/cm2 in a rat model of experimental arthritis induced by injection of complete Freund's adjuvant (CFA) on the changes in TNF-α, MMP3 expression, the numbers of inflammatory cells and FLS, and synovial apoptosis in the inflamed synovium at the early phase of arthritic inflammation.
Materials and Methods
General design
Arthritis was induced in rats (n=50) by intra-articular injection of CFA. Following 3 days of CFA induction, the arthritic animals were randomly divided into five groups (each group containing 10 animals) according to five treatments named: LF group, animals treated with laser at 4.5 J/cm2; sLF group, animals treated with sham-LF laser irradiation at 0 J/cm2; HF group, animals treated with laser at 72 J/cm2; sHF group, animals treated with sham-HF laser irradiation at 0 J/cm2; and CFA-only group, animals kept as a treatment control and administered CFA alone and without laser treatment. The treatments using laser or sham irradiation were given on the 3rd day after CFA induction for 10 consecutive days. After completing the treatments, the animals were euthanized for histopathology assessment and immunoassays. A flow diagram of the experimental design is presented in Fig. 1.

Experimental design. Three days after injection of complete Freund's adjuvant (CFA), animals were treated with laser by outputs of lower fluence (LF, 4.5 J/cm2), sham-operated LF (sLF, 0 J/cm2), higher fluence (HF, 72 J/cm2), sham-operated HF (sHF, 0 J/cm2), and none of these treatments (CFA-only). After the 10 day treatment, the animals were euthanized for histology, terminal deoxynucleotidyl transferase dUTP nick end labeling (TUNEL), immunohistochemistry (IHC), and immunofluorescence (IF) assays.
Animal preparation
Adult male Sprague–Dawley (CD®[SD] IGS BR; purchased from BioLASCO Taiwan Co., Ltd.) rats weighing 250–300 g were kept in the Laboratory Animal Center of China Medical University. Effort was made to minimize discomfort and keep the number of animals used to a minimum. All animal experiments were conducted with the procedure approved by the animal care and use committee of a university in accordance with the guidelines for animal experimentation.
Induction of monoarthritis
Monoarthritis was induced by an injection of CFA into the randomly selected unilateral ankle. The rats were briefly anesthetized with 4% isoflurane (AERRANE, Baxer Healthcare Corporation, Puerto Rico). A 28-gauge needle was vertically inserted distally into the articular cavity from the gap between the tibiofibular and tarsus bone. CFA with volume of 50 μL (10 mg mycobacterium, F5881, Sigma, MO) was then injected. The monoarthritic animals were separately placed in clear acrylic containers (27 cm W×48 cm D×20 cm H), allowing free movement for at least 24 h to let them adjust to these conditions before any experimentation was performed.
Low-level laser irradiation
A continuous 780 nm GaAlAs diode laser (Aculas-Am series, Multi-channel laser system; Konftec Corporation, Taipei, Taiwan) was used in the treatment. After sterilization, the handheld delivery probe was lightly placed on the skin surface directly above the arthritic site at four spots per area. The spot size was ∼0.2 cm2. The laser irradiation at low fluence was 30 mW per session for 30 sec per spot (energy density: 4.5 J/cm2) and at high fluence was 80 mW per session for 180 sec per spot (energy density: 72 J/cm2). The output of the equipment was routinely checked using a Laser Check Power Meter (Coherent Inc, Santa Clara, CA). A similar procedure was applied to the sham operation group using sham irradiation such that the contact time of laser application corresponding to the fluences of 4.5 and 72 J/cm2 for the sLL and sHL groups were 30 sec and 3 min, respectively, but the laser powers were set at 0.
Tissue preparation and histopathological evaluations
Animals were euthanized by anesthetic overdose after treatments, and then their hind ankles were collected for histological, immunohistochemical, and immunofluorescent analyses. The specimens were fixed in 4% phosphate-buffered saline (PBS)-buffered paraformaldehyde for 48 h and decalcified in PBS-buffered 10% ethylenediaminetetraacetic acid (EDTA) for 14 days at 4°C. Specimens were frozen with liquid nitrogen immediately after decalcification and kept at −80°C until analysis. The ankle joint tissues were frozen, and sagittal sections of 4 μm thickness were cut serially with a freezing microtome. Each specimen produced ∼60 sections. Each staining assay was examined in 10 alternate sections per ankle joint per rat, which were selected by a systematic random series with a random start for analysis. Histopathological evaluation was performed using hematoxylin and eosin (H&E) for each animal.
Immunohistochemical and immunofluorescent analyses
The frozen sections were incubated overnight at 4°C with mouse monoclonal antifibroblast antibody (5B5, a biomarker of FLS) (Abcam, Cambridge, UK), rabbit polyclonal anti-TNF-α antibody (Abcam, Cambridge, UK), or rabbit polyclonal anti-MMP3 antibody (Abcam, Cambridge, UK) followed by the secondary antibody. The sections with anti-5B5 were incubated with biotinylated antimouse immunoglobulin G (IgG) (Jackson Immunoresearch, PA), and then visualized as brown precipitates by 3,3′-diaminobenzidine (DAB, Pierce, Rockford, IL) and counterstained with hematoxylin. The sections with anti-TNF-α and anti-MMP3 were incubated with Alexa Fluor 594-conjugated goat antirabbit IgG (Molecular Probes, Inc. Eugene, OR) and Alexa Fluor 488-conjugated goat antirabbit IgG (1:500, A11008, Molecular Probes, Inc. Eugene, OR), respectively, and counterstained with 4′,6-diamidino-2-phenylindole (DAPI, Life Technologies, Carlsbad, CA). Normal mouse and rabbit IgGs (Jackson Immunoresearch, PA) were used to replace the primary antibodies as negative controls.
Terminal deoxynucleotidyl transferase dUTP-mediated nick-end labeling (TUNEL) assay
Unstained sections were obtained for the detection of apoptosis using the TUNEL reaction mixture (Roche Applied Science, Indianapolis, IN) according to the manufacturer's instructions. Then, the DAPI was added for displaying the nucleus position. TUNEL-positive nuclei (fragmented DNA) were fluoresced by bright green light at 450–500 nm.
Quantitative analysis
The slides were examined and photographed at five randomly selected fields at 200× magnification using a light microscope (BX43, Olympus America Inc. NY) and a cooled digital color camera with a resolution of 1360×1024 pixels (DP70, Olympus America Inc., NY). The digital images were analyzed using a computer-based morphometry, Image-Pro Plus 4.5 software (Media Cybernetics, Silver Spring, MD). Based on the automatically calculated parameters, the labeled area by DAB-, Alexa- or TUNEL-positive staining cells in each section was measured. The percentage of positive and strong immunoreactivity-positive pixels to total counterstained pixels in synovium (%) was analyzed. All counts were performed by at least two independent individuals in a blinded manner.
Statistical analysis
All data are expressed as mean±standard deviation (SD). One way analysis of variance (ANOVA) was used to determine the differences in the levels of inflammatory cells, 5B5-, TNF-α-, and MMP3-like immunoreactivities, and TUNEL-positive cells among CFA-only, LF, sLF, HF, and sHF groups. Scheffe's method was used to examine post-hoc for comparisons between groups. A p value of<0.05 was considered statistically significant. All data were analyzed using SPSS version 17.0 for Windows (SPSS Inc., IL).
Results
Histopathological assessments
Synovium from LF groups analyzed by H&E staining showed that they were less inflamed, as revealed by the decreased number of inflammatory cells in the synovial membrane (Fig. 2A). Conversely, thickening and widening of the synovial membrane and infiltration of inflammatory cells were apparent in rats from the sLF, HF, sHF, and CFA-only groups (Fig. 2B–E). There were significant differences in infiltration of mononuclear cells observed among the ankle joint synovium from the CFA-only, LF, sLF, HF, and sHF groups (p<0.05). Infiltrations of mononuclear cells in the synovium were significantly reduced in the LF group when compared with those in the sLF group (p<0.05). There were no significant differences between the HF and sHF groups (p>0.05). Moreover, significantly fewer inflammatory cells existed in the LF group than in the HF group (p<0.001, Fig. 2F).
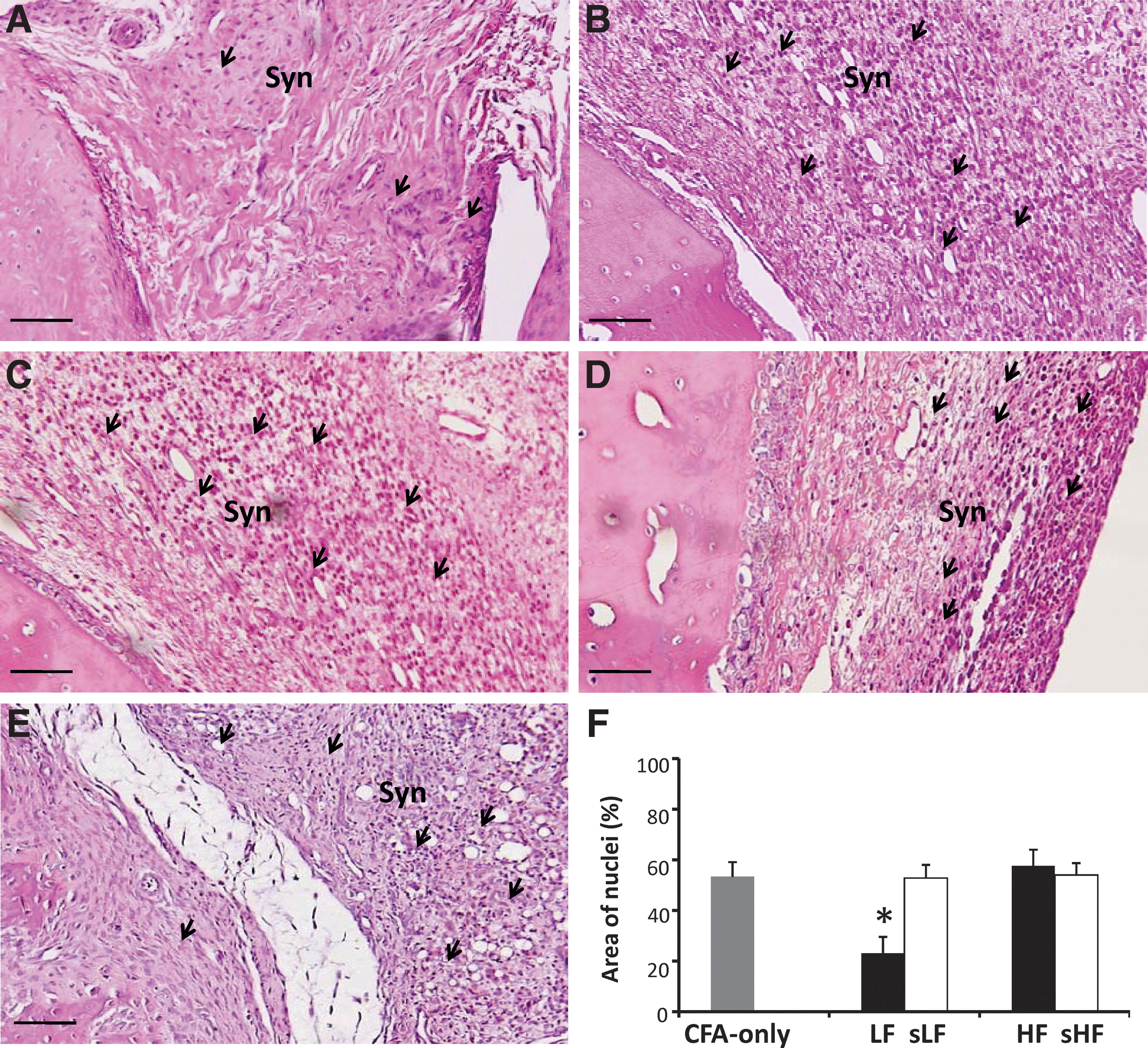
Histopathological analysis in complete Freund's adjuvant (CFA)-induced arthritic rats treated with laser. All CFA-treated synovium showed synovial hyperplasia (Syn) and infiltration of inflammatory cells (arrows). Representative hematoxylin and eosin staining for the sequential joint sections from rats treated with laser in the lower fluence (LF)
Quantitative assessments on 5B5-, TNF-α- and MMP3-like immunoreactivities
Synovial lining cells labeled with 5B5 with CFA-induced arthritic synovium were seen in all cases in the CFA-only, LF, sLF, HF, and sHF groups. Intimal cell labeling with 5B5 showed the presence of DAB reaction product localized mainly to cells beneath the surface of the intimal layer. These cells correspond to type B synoviocytes (i.e., FLS) in their distribution. After LF laser treatment, the expressions of 5B5 immunoreactivities were reduced (Fig. 3A). Overexpressions of 5B5 immunoreactivity were found within the synovial tissues in the, sLF, HF, and sHF and CFA-only groups (Fig. 3B–E). There were significant differences in 5B5 immunoreactivities observed in the ankle joint synovium among the CFA-only, LF, sLF, HF, and sHF groups (p<0.05). The cells labeled with 5B5 were significantly reduced after LF laser treatment compared with those treated with sLF laser (p<0.05, Fig. 3F). There were no significant differences between the HF and sHF groups (p>0.05). Moreover, significantly fewer 5B5-labeled synoviocytes were found in the LF group than in the HF groups (p<0.05, Fig. 3F).
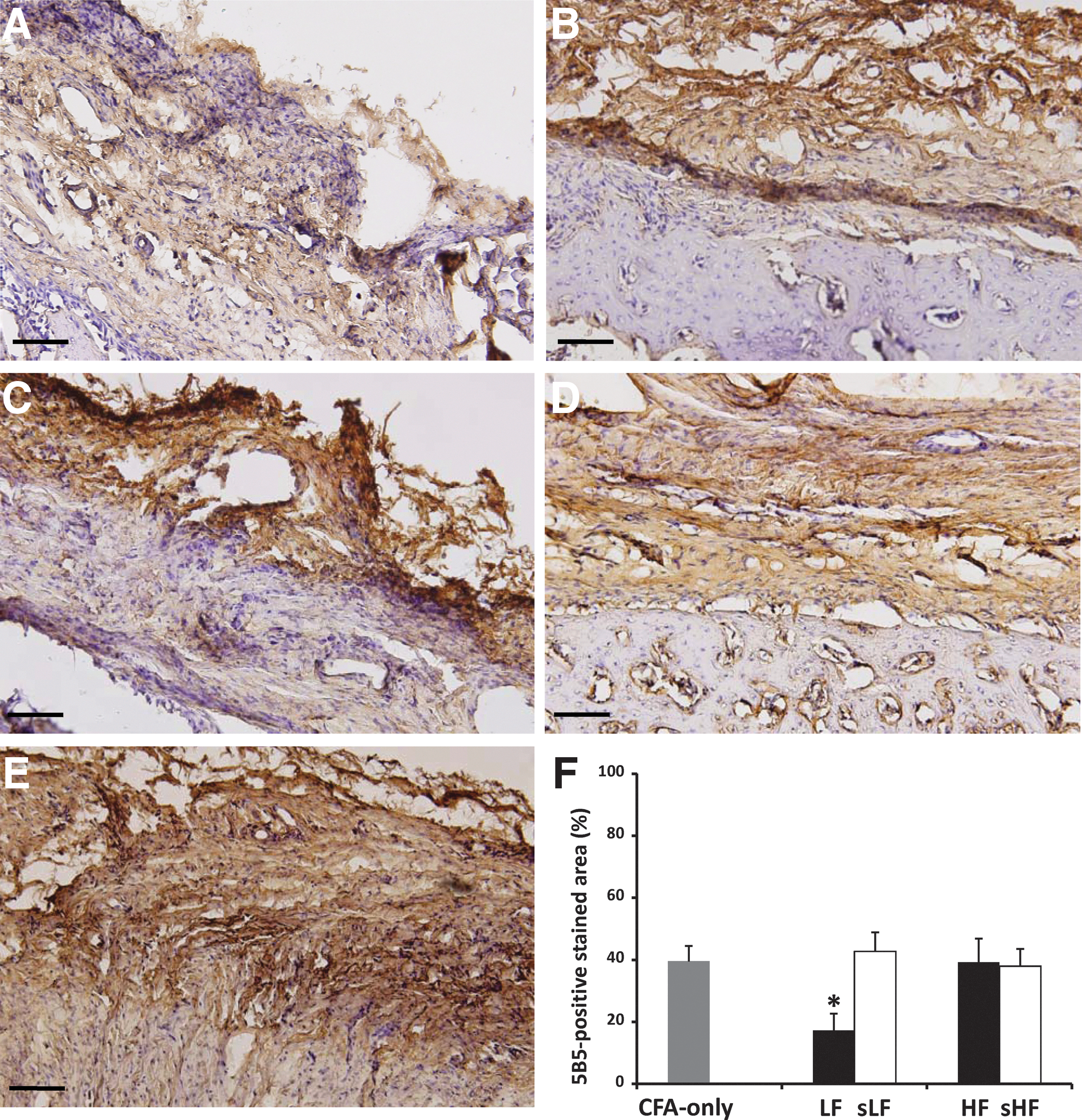
The immunohistochemical expressions of 5B5-labeled synoviocytes in complete Freund's adjuvant (CFA)-induced arthritic rats treated with laser. Representative 5B5 immunohistochemical staining for the sequential joint sections from rats treated with laser in the lower fluence (LF)
Immunofluorescent staining revealed reduced expressions in TNF-α- and MMP3 -like immunoreactivities in the LF group (Figs. 4A and 5A) compared with those in the sLF, HF, sHF, or CFA-only groups (Figs. 4B–E and 5B–E). At higher-power magnification, it was evident that these positive immunoreactivities were clearly localized in both the nucleus and cytoplasm of the arthritic synovium. The primary cells exhibiting specific TNF-α and MMP3 immunofluorescent activities were morphologically consistent with inflammtory cells, mainly in the synovial joint. After laser treatment, the significant differences in the extent of TNF-α and MMP3 immunoreactive expressions were significant among the LF, sLF, HF, sHF, and CFA-only groups (TNF-α, p<0.001; MMP3, p<0.001). Significantly lower expressions of TNF-α and MMP3 immunoreactivity existed in LF group than in the sLF group [TNF-α: p<0.001 (Fig. 4F); MMP3: p<0.001 (Fig. 5F)]. In addition, lower expressions of TNF-α- and MMP3-like immunoreactivities existed in the LF group than in the HF group (p<0.05).
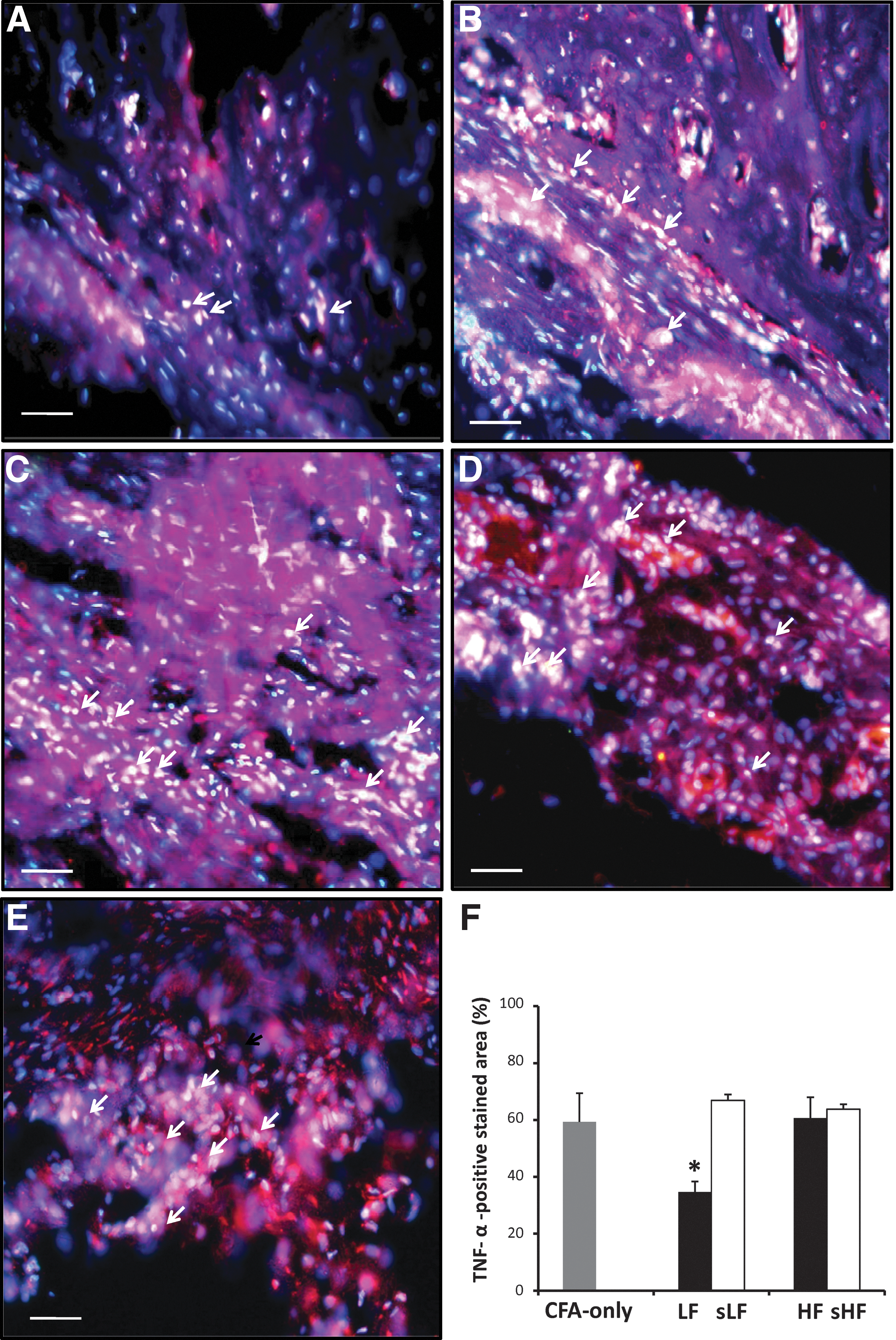
The immunofluorescent expressions of tumor necrosis factor (TNF)-α-like immunoreactivity in the synovium of complete Freund's adjuvant (CFA)-induced arthritic rats treated with laser. Representative TNF-α-positive immunofluorescent staining (Alexa Fluor 594-red) for the sequential joint sections from rats treated with laser in the lower fluence (LF)

The immunofluorescent expressions of matrix metallopeptidase (MMP)3-like immunoreactivity in the synovium of complete Freund's adjuvant (CFA)-induced arthritic rats treated with laser. Representative MMP3-positive immunofluorescent staining (Alexa Fluor 488-green) for the sequential joint sections from rats treated with laser in the lower fluence (LF)
TUNEL-positive apoptotic cells of synovium tissues
To reconfirm if apoptotic activity took place in hyperplasia synovium after LLLT, we examined the apoptotic synovial cells in each group by TUNEL assay. There were fewer apoptotic activities in the synovium of the CFA-only, sLF, HF, and sHF groups than in the LF group. After LF laser treatment, more TUNEL-positive apoptotic cells were observed in the inflamed synovium of the LF group, but they were significantly higher than those in the sLF and HF groups (all p<0.05, Fig. 6).
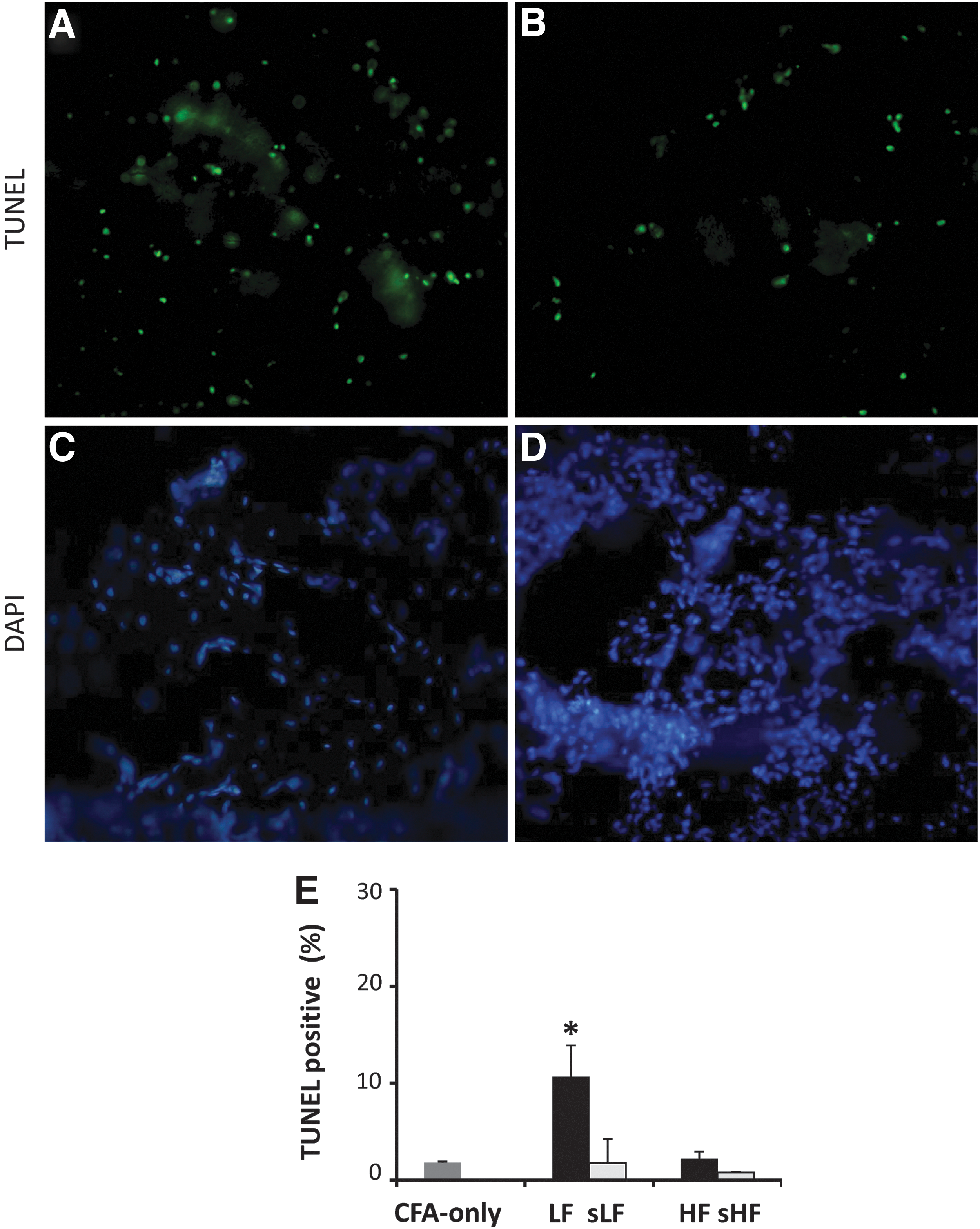
The apoptotic activity in the synovium of complete Freund's adjuvant (CFA)-induced arthritic rats treated with laser. CFA-treated synovial sections were stained for apoptosis using the terminal deoxynucleotidyl transferase dUTP nick end labeling (TUNEL) assay (green, upper panel). 4′,6-diamidino-2-phenylindole (DAPI) (blue, lower panel) was used to stain for nuclei. Representative TUNEL-positive and DAPI stainings for the same joint sections from rats treated with laser in lower fluence (LF) (
Discussion
Numerous studies indicate the positive clinical performance of LLLT as a treatment modality in the relief of pain and morning stiffness for RA patients. 12,13 However, several research articles regarding the clinical performance and treatment efficacy of LLLT in RA showed conflicting and controversial results, because the suitable therapeutic parameters of laser such as energy dosage and treatment duration in the management of RA are still not clearly defined. This study demonstrated the comparative effects of 780 nm LLLT with two different fluences, 4.5 J/cm2 (LF) and 72 J/cm2 (HF) in rats with synovitis at the early phase of CFA-induced inflammation.
In the present study, CFA-induced arthritis led to persistent synovial inflammation and hyperplasia because of increased expression of TNF-α, MMP3, and inflammatory cell infiltration in the synovium. LLLT with 4.5 J/cm2 induced reduction in inflammatory mediators in the synovium apparently via a reduction in inflammatory cell infiltration and FLS markers. Moreover, TNF-α and MMP3, the two important mediators involved in the pathogenesis of RA, were also significantly reduced after LF laser therapy when compared with the untreated counterpart (CFA-only group). The levels of TNF-α and MMP3 were reduced by ∼30% and 50%, respectively, in the synovial tissue from the LF laser-treated ankle compared with the two counterparts, the sLF and HF groups. These results further supported the beneficial effect of LF laser therapy on the treatment of CFA-induced RA, especially for the reduction in inflammation and numbers of FLS.
Several studies involving the use of LLLT as a therapeutic approach demonstrated the ability of laser light to modulate inflammatory biomarkers in various osteopathic situations. 10,14 –17 An 810 nm LLLT at 5 J/cm2 can decrease the mRNA levels of TNF-α and IL-1β in FLS from RA patients. 17 Also an 810 nm LLLT with 50, 150, and 300 J/cm2 was able to inhibit the total numbers of leukocytes and mononuclear cells, as well as mRNA levels of IL-6 and IL-1 in rats with carrageenan-induced knee arthritis. Significant reduction particularly occurred at the lower energy density of 50 J/cm2. 16 An 808 nm AsGaAl laser at doses of 2 and 4 J can reduce the numbers of inflammatory cells (neutrophils and macrophages), TNF-α protein expression, as well as IL-1β and IL-6 mRNA expression on joint inflammation in rats induced by papain. 10
These results also indicated a higher efficiency for the 2 J laser irradiation in attenuating the general inflammatory process, in particular with regard to the expression of TNF-α and the migration of neutrophils during the initial inflammatory phase of osteoarthritis. 10 A 660 nm InGaAIP laser at 2.5 J/cm2, which immediately irradiated 1 and 2 h after zymosan administration, significantly inhibited leukocytes influx and the release of IL-1 and IL-6 into the joint cavity on acute zymosan-induced arthritis in rats. 18 However, in the other experimental study, a 660 nm LLLT with higher energy density, 214 J /cm2, which irradiated at the 72th h after tenotomy of the Achilles tendon, also significantly reduced the IL-6 level, but not IL-1 in the acute phase of inflammation in rats. 15 In another experimental model, a 685 nm LLLT with 3.0 J/cm2 also significantly reduced the expression of TNF-α and IL-6 in the saliva of subjects with burning mouth syndrome. 19 These previous studies, which involved the analysis of several inflammatory mediators, including TNF-α, IL-1β and IL-6, demonstrated the effectiveness of LLLT in treating the inflammatory process, and also indicated the property of laser light on modulation of these proinflammatory mediators, especially for the LLLT with LF in attenuating the general inflammatory process and the expression of TNF-α. This can probably be explained by different applications of various wavelengths and fluences in these experimental trials.
The proinflammatory cytokine TNF-α has been shown to play an important role in the pathophysiology of arthritis development in animal models and humans. TNF-α was the major dominant regulator of the other proinflammatory cytokines, leading to the new concept that the proinflammatory cytokines were linked in a network with TNF-α at its apex. This led to the hypothesis that TNF-α was of major importance in RA and was a therapeutic target. 20 This hypothesis has been successfully supported by CFA-induced arthritic animal models, 21,22 and also provided the rationale for clinical trials of anti-TNF-α therapy in patients with RA. 23,24 Moreover, TNF-α is expressed in the lining of the synovial membrane at the time of arthritis onset. 20 Therefore, various strategies to modulate and inhibit TNF-α activity and expression are now being clinically applied and have been shown to be effective in the early phase of arthritic inflammation in RA. In this sense, we aimed to examine the effect of 780-nm GaAlAs laser with two fluences, 4.5 and 72 J/cm2, as a modulatory tool on TNF-α expression in the CFA-induced arthritic synovium. Our results point to a significant decrease in the modulation of expression of TNF-α and inflammatory cells when they are irradiated by LLLT at a fluence of 4.5 J/cm2 72 h after the induction of inflammatory arthritis in the rat ankle. This was consistent with several studies that showed the modulation of TNF-α by LLLT with LF. 17,19
Currently, there is a growing consensus that various proinflammatory cytokines produced by stimulated synovial macrophages are partly responsible for triggering the morphological changes that are found in joint cartilage caused by MMPs. 25 Therefore, MMPs and cytokines (IL-1, IL-6, and TNF-α) are responsible for the inflammatory signals that occur in the breakdown of cartilage. Among the MMPs, MMP3, which is a key enzyme involved in RA-associated destruction of cartilage and bone, may be considered as one of the biological markers used to diagnose RA. 7 In the CFA-induced arthritic model used in this study, the expression of MMP3 in synovium decreased after LLLT at 4.5 J/cm2, showing the same extent of reduction of TNF-α. This result may suggest delayed destruction of cartilage and bone by decreasing the activity of MMP3. Our results were similar to a previous study 18 that found thatInGaAIP (660 nm, 2.5 J/cm2) significantly decreased the activity of MMP2 and MMP9 after zymosan injection, showing a decrease in MMPs, and suggesting less degradation of collagen tissue after LLLT with LF.
The mechanism for relieving joint pain in RA by LLLT may involve reducing the level of proinflammatory cytokines/chemokines produced by synoviocytes (FLS and macrophage-like synoviocyte). Therefore, the mechanism in the reduction of FLS proliferation may be more general, and may underlie the beneficial effects of LLLT on RA inflammatory conditions; 5B5, considered a typical fibroblast marker, reacts with human prolyl 4-hydroxylase and is an intracellular enzyme related to collagen biosynthesis. 26 Previous studies demonstrated that 5B5 appeared to be a marker of type B synoviocytes and contained a relatively large proportion of proline, but this is in addition to its marking of other collagen-producing cells. 27 –29 Hence, we investigated 5B5 levels to evaluate the counts of FLS after laser irradiation, and found that LLLT significantly reduced 5B5 expression at 4.5 J/cm2. Among the groups, the LF laser group showed significantly better results in reducing FLSs compared with the other irradiation groups. We also observed that the LF group treated with 4.5 J/cm2 fluence had lower inflammatory cell counts observed via the histological analysis compared with the HF group with 72 J/cm2. Moreover, for the effect of LLLT in apoptotic induction, the LF group had a more TUNEL-positive nuclei (fragmented DNA) than those in the HF group. This also indicates that LLLT with 4.5 J/cm2 does not reduce merely the FLS, but also reduces the infiltration of immune cells during the initial inflammatory phase.
Laser fluence, depending upon output power, mode, irradiation time, and power density, is one of essential parameters to determine the interaction of laser and tissue. The most critical limitation of this study is the difficulty in confirming the correlation between of all laser fluence parameters from 4.5 to 72 J/cm2, and joint inflammation in CFA-induced arthritic rats. Our study determined that the lower-fluence LLLT provided by shorter irradiation time and lower output is a practicable way to modulate arthritic inflammation, FLS, and synovial apoptosis. However, it is still unknown whether these effects exist for other fluences or modes when the same irradiation time is given, and, therefore, further studies are necessary in the future.
Conclusions
Our results provide evidence of laser fluence-dependent reductions in TNF-α and MMP3, and of the ability of LLLT to inhibit the proliferation of inflammatory FLS. This makes LLLT with LF a suitable treatment for synovitis that is associated with the early stages of inflammation in RA. Our results also indicate a better understanding of the role of laser fluence in modulating these mediators that could be a basis for future therapeutic interventions. We conclude that a single application of LLLT with a fluence of 4.5 J/cm2 is more efficient in modulating inflammatory mediators and inflammatory cells, and its effects can be observed by histological signs of attenuation of the inflammatory processes. In addition, there are significant improvements in reduction of inflammation and FLS proliferation found in animals treated with 4.5 J/cm2, but not with 72 J/cm2.
Footnotes
Acknowledgments
This study was supported by the National Science Council of Taiwan (Grant number: NSC 101-2314-B-241-039-003MY2) and China Medical University (Grant number: CMU101-S-35).
Author Disclosure Statement
No competing financial interests exist.