
Abstract
Introduction
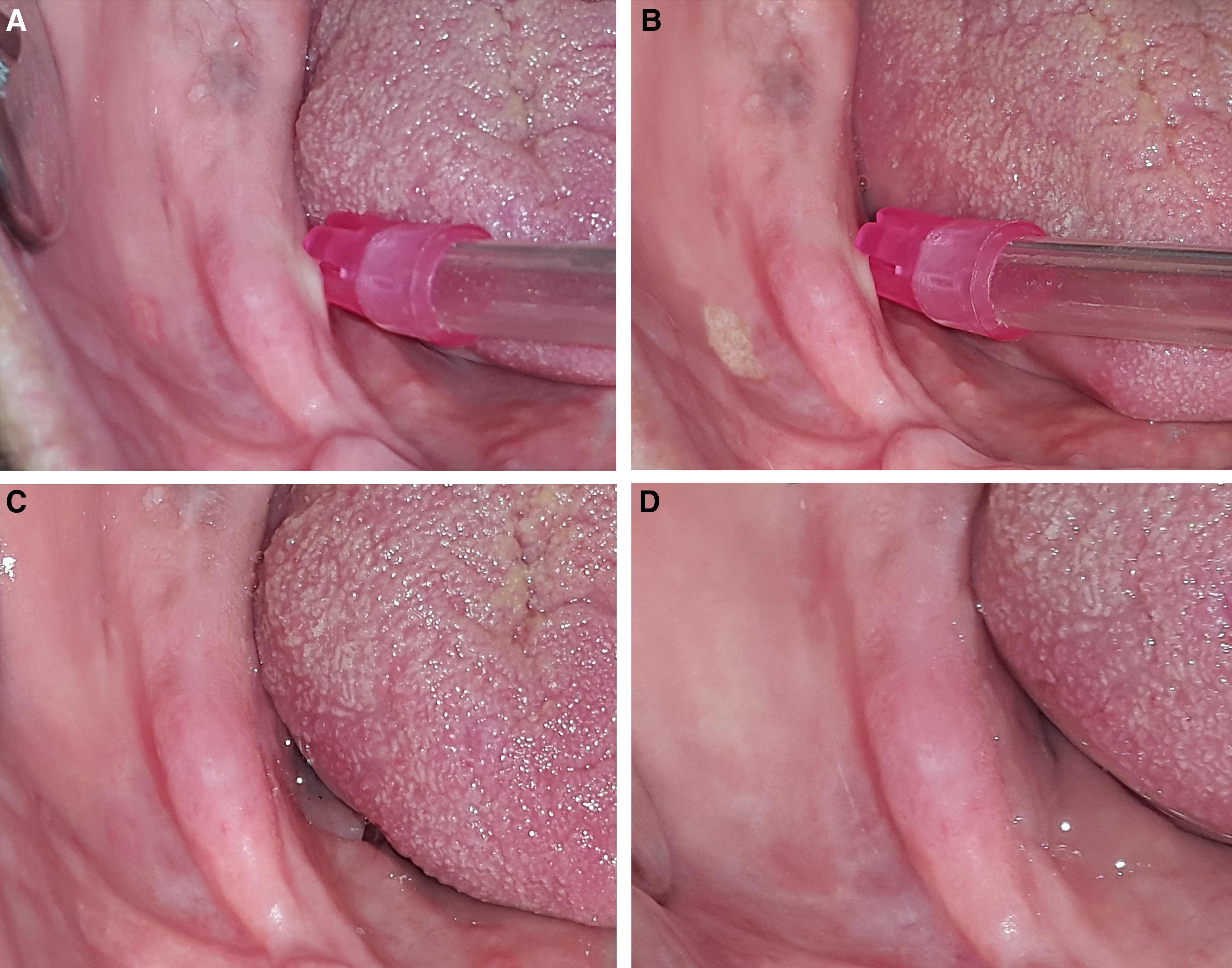
B
Currently, the treatment of denture-related traumatic ulcers includes adjustment of the margins and occlusal adaptation of the dentures. However, ulcers are painful and result in patient discomfort. Therefore, patients do not want to wear their dentures. Reduction of ulcer inflammation and relief of pain with the use of topical agents are widely acknowledged as important. The types of therapy given usually include topical anesthetics, and triester glycerol oxide gel (TGO). 9,10 Although laser therapy is performed in dentistry as a therapeutic agent for aphthous stomatitis, mucous membrane pemphigoid, and other mucosal lesions, 11 –14 to the best of our knowledge, there is no study evaluating laser irradiation for the treatment of denture-induced mucosal ulcerations.
The purpose of this randomized controlled clinical study was to evaluate the efficacy of Er,Cr:YSGG laser irradiation in reducing pain and on the healing rate of denture-induced mucosal ulcerations during a 2-week period after placement of new complete dentures.
Materials and Methods
A total of 30 edentulous (18 female 12 male) patients between the ages of 48 and 74 (mean age: 58±8.6 years) who were scheduled to be treated with complete maxillary or/and mandibular dentures were recruited for this study. For inclusion in the study, the subjects had to have one or more pairs of denture-related ulcerative lesions. Exclusion criteria were having any systemic diseases, xerostomia, hypersalivation, pregnancy, smoking, and using analgesics/anti-inflammatory drugs at the time of the study. Patients were orally informed regarding the treatment plan and possible discomforts, and the potential risks of the treatment. Afterwards, patients were asked to sign the informed consent form. Study protocol and written consent forms were approved by the Research and Ethics Committee of Near East University.
Maxillary and/or mandibular complete dentures were fabricated for all patients by two clinicians with at least 10 years of experience. Both of the clinicians used the same techniques and materials for the fabrication. One day after placement, all the subjects were recalled and asked to record their pain and discomfort level with their new dentures by marking a point on a 10 cm visual analog scale (VAS). Prosthetic parameters such as occlusion, stabilization, and tissue adaptation were evaluated by the two clinicians, and overextended flanges or any sharp parts causing tissue irritation and ulcerations were removed with the use of a tungsten carbide bur.
In each of these patients, a minimum of two ulcers as measured by the investigator, with a minimum dimension of 5 mm and a maximum dimension of 1 cm were selected in symmetrical locations in the oral cavity. In this split-mouth study for each subject, selected ulcerations were randomly assigned to the test or the control group by the toss method. After randomization, half of the ulcerations (in the test group) were irradiated with Er,Cr:YSGG laser (Waterlase MD, Biolase, Irvine, CA) with a MG6 sapphire tip (600 mm diameter, 6 mm length) using a noncontact mode at 0.25 W energy level, 20 kHz frequency, and a pulse duration of 140 μs with 0% water and 10% air at 5 J/cm2 energy density on hard tissue. The treatment time was 20 sec per surface by scanning the ulceration area (Fig. 1). For the control group, the same Er,Cr:YSGG laser without laser emission was used (Fig. 2). If any patients had more than two ulcerations, all ulcerations on the same side received the same treatment. It was a single-blind study; therefore, the subjects were unaware as to which of the ulcerations was going to be treated with laser and which would be selected as a control. All active and placebo treatments were performed only at the first visit after the placement of dentures.

Pain and discomfort were assessed with VAS scores, and VAS scores were recorded at five examination periods: immediately, at 1, 3, 7, and 14 days after treatment. The healing of ulcerations (HU) was evaluated at the follow-up sessions by the investigators using a four-point scale (range 1–4) based on the methods of Geckili et al. 10 with some modifications. Grade 1 represented total healing, grade 2 represented moderate healing (≥50% of ulceration was epithelialized and healed), grade 3 represented slightly healing (<50% of the ulceration was epithelialized and healed) and grade 4 represented no healing.
Mean values of the clinical parameters were calculated for all groups. A Shapiro–Wilk test was performed to detect if the scores were distributed normally. To evaluate the changes over time within the groups, one way repeated analysis of variance was used, and when significance was detected, post-hoc comparisons were performed by using the Tukey test. A paired t test was used for comparison between groups at each time point. Values of p<0.05 were accepted as statistically significant.
A calibration session was performed to determine interexaminer consistency, and six subjects' data were included in this session. Reliability of HU scores was determined by using Cohen's k, and the k value for HU evaluation was found as 0.82±0.08. The range of mean errors for VAS scores were 0.14–0.18, and indicated consistent reliability during the evaluation period.
Results
All 30 patients completed the 2-week study period. No complications such as soft tissue damage were observed. A total of 94 ulcerations were observed in all of the patients, and distribution of these ulcerations can be seen in Table 1 (34 in the maxilla, 60 in the mandible). The ulcerations were most often observed at the anterior vestibule sulcus (52%) or tuberosity (38%) in the maxilla, and at the posterior lingual sulcus (47%) or posterior buccal sulcus (35%) in the mandible. No complications were determined in any group during the entire evaluation period. The mean VAS and HU scores before and after treatments of ulcerations can be seen in Tables 2 and 3, respectively. When compared with the control group, in the Er,Cr:YSGG laser group, laser irradiation provided a pain-reducing effect immediately after treatment that was maintained throughout the study (p<0.001, Table 2). In the control group, baseline VAS scores were not statistically significant immediately or 1 day after treatment. Intergroup comparisons revealed that the differences of VAS scores immediately, and 1, 3, 7 days after treatment were statistically significant (p<0.001, Table 2). Evaluation of HU scores showed that Er,Cr:YSGG laser irradiation provided a significantly healing effect 1 day after treatment, which was maintained throughout the duration of the study (p<0.01, Table 3). In the control group, HU scores were statistically significant 3, 7, and 14 days after treatment (p<0.05, Table 3). Intergroup comparisons revealed that the differences in HU scores were statistically significant for all time periods after treatment, except day 14 (p<0.01, Table 3).
n.a., not applicable
Different letters show statistical significance at intragroup comparisons, p<0.05, repeated ANOVA.
The differences immediately, and 1, 3, and 7 days after treatment were statistically significant between the laser group and the control group; p<0.05, paired t test.
VAS, visual analog scale.
Different letters show statistical significance at intragroup comparisons, p<0.05, repeated ANOVA.
The differences at 1, 3 and 7 days after treatment were statistically significant between the laser group and the control group, p<0.05, paired t test.
HU, healing of ulcerations.
Discussion
Treatment of edentulism with complete dentures is still employed widely because of its relative inexpensiveness and simplicity. The border extensions of dentures play a key role in retention. Kivovics et al. 15 investigated the mucosal tissues of edentulous patients following the placement of complete dentures, and reported that it not always possible to record the depth of vestibule sulcus exactly, and this may cause overextended denture flanges. Overextension of denture borders can cause ulceration and pain. Also with increasing age, oral epithelium becomes thinner, because the collagen synthesis decreases. 1 Also, the resilience and tissue regeneration capacity of mucosa diminishes, and, therefore, it becomes more vulnerable to mechanical traumas and can be easily irritated. 1,8 The ulcerations were seen mostly at the maxillary tuberosity in the maxilla, and at the posterior portion of the alveololingual sulcus in the mandible. 8,10
Consistent with these results, in the current study, the most frequent appearances were at the anterior vestibule sulcus and tuberosity in the maxilla, and the posterior lingual and buccal sulcus in the mandible. Although patients had spontaneous healing within 7–10 days after the adaptation of dentures, treatment was indicated to reduce fever and control pain. 4 Reducing pain and healing time for traumatic ulcers restores patient ability to eat, swallow, and talk, thus improving patients' quality of life. Therefore, effective treatment approaches are needed to promote rapid pain reduction and the healing process of denture-related ulcers and prevent their consequences.
Geckili et al. 10 have evaluated the use of TGO gel in the treatment of denture-related mucosal injuries and reducing pain. They reported that TGO gel is not effective in the treatment of mucosal injuries and reduction of pain that occurs after the placement of complete dentures. Graser 9 evaluated the effectiveness of three topical anesthetic gels in the reduction of soreness caused by denture irritation, and stated that all three gels showed limited effect. Recently Jivanescu et al. 16 investigated the efficacy of a hydrogel patch wound dressing on the healing rate of denture-induced lesions of the oral mucosa, and its effectiveness on the reduction of pain. They reported that the hydrogel patch accelerated the healing process and reduced the pain of ulcers induced by the complete dentures. However, they stated that the study was not randomized and that the researchers assigned the larger lesion as the test lesion. Therefore, this allocation may have affected the results and could have introduced some bias. The results of the current randomized controlled study demonstrate that treatment with the Er,Cr:YSGG laser not only reduced the size, erythema, and degree of exudation associated with traumatic ulcers, but also helped resolve patient pain immediately, and that this effect was maintained through the healing of ulcerations. However, as a limitation of this study, although symmetrical locations were selected in the split-mouth design, the anatomy and occlusion of each patient may have had an important influence. Therefore, studies with a larger sample size are needed for the elimination of this issue.
Lasers were considered as the choice of alternate treatment because of some of their promising properties, such as an excellent water absorption property, and their effective absorption by biological tissues with minimal disturbance of surrounding structures. Many lasers, including galium–aluminium–arsenide (GaAlAs) diode laser, neodymium-doped: yttrium, aluminium and garnet (Nd:YAG), and carbon dioxide (CO2), were used in the treatment of different kind of mucosal lesions. 11 –14 Lasers are especially used in the treatment of recurrent apthous stomatitis, 12,13 because it is a painful lesion, has a relatively long healing period, and cannot be treated completely with conventional methods. However, a review of literature shows that there are no published data available concerning the clinical outcome of the use of laser therapy for traumatic ulcerations.
Er,Cr:YSGG lasers are currently used for a wide range of dental applications, including endodontics, periodontics, preventive dentistry, and oral surgery. 17 –20 The interaction of Er,Cr:YSGG laser with atomized water droplets on the tissue interface results in the ablation of the tissue, which provides a precise cut of hard and soft tissues. 17 In addition to the existing water in tissue, the Er,Cr:YSGG laser uses exogenous water for ablation; 21 therefore, in the present study, Er,Cr:YSGG laser was used without water to avoid the ablation. The higher water absorption coefficient causes rapid vaporization and microexplosions that creates high pressure on the surrounding cells. Also, in comparison with near infrared (810–1064 nm) and Nd:YAG lasers, Er,Cr:YSGG laser (medium infrared: 2780 nm) has the advantage of causing minimal tissue distortion because of less thermal deep or lateral damage as the heat escapes by means of vaporization. 11 Thus, Er,Cr:YSGG laser produced a relatively thin coagulation layer on the lesion surface because of the laser's penetration and thermogenesis. This coagulation layer may desensitize the underlying tissues.
However, further histological studies are needed for the evaluation of this coagulation layer and a detailed explanation of this desensitizing mechanism. It is also known that erbium laser irradiation can generate reactive oxygen species, which have sterilization effects and stimulate fibroblast, collagen, and extracellular matrix formation in the tissue. 22 The high bactericidal potential of Er,Cr:YSGG laser 23 is also important, because bacteria have the ability to lower pain thresholds at injured tissues as a result of increased inflammatory mediator synthesis and infection. Another possible mechanism of the Er,Cr:YSGG laser in the reduction of pain is its effect on the neural receptor transient receptor potential cation channel subfamily V member 1 (TrpVl), which is known to be stimulated by heat. It has been reported that thermal-sensitive TRPs in nerves may serve as pain sensors. In a recent article, Ryu et al. 24 tested the effects of Er,Cr:YSGG laser on cultured trigeminal neurons and cell cultures overexpressing TRPVl, and they showed that Er,Cr:YSGG laser irradiation blocks the TRPV channel function in sensory neurons rather than damaging cells. Thus, Er,Cr:YSGG laser treatment may cause analgesia via TRPVl inhibition.
In the current study, VAS was preferred, because it is frequently used, and is sufficient for the assessment of pain. 9,10 Also patients can easily understand a VAS, and it is sensitive in discriminating the effects of various types of treatments. Therefore, VAS can be a suitable method for the evaluation of the pain level in the presence of ulcerations 9,10,12 However, VAS evaluation may be inadequate if the test and control sides are close to each other. Therefore, in the current split-mouth study, symmetrical lesions were selected, and if any subjects had more than two ulcerations, all ulcerations on the same side received the same treatment.
Conclusions
Within the limitations of this study, it may be suggested that Er,Cr:YSGG laser application could be suitable for pain reduction and acceleration of the healing process of traumatic ulcerations because of its rapid clinical effectiveness and lack of adverse reactions.
Footnotes
Author Disclosure Statement
No competing financial interests exist