
Abstract
Introduction
T
Even though bleaching treatment is highly standardized, including the recommendations for proper duration of the bleaching process, outcomes are quite unpredictable and usually noticeably different among individuals. In addition to overbleaching, a common side effect of the light-activated bleaching procedure is overheating. 9,10 Some other complications may occur, such as pulp irritation, tooth structure alterations, microleakage of restorations, and reduced bond strength of composite resin to previously bleached tooth structure. 11,12 Dealing with these issues imposes a need for real time monitoring of the bleaching process. To fill this gap, this study presents a newly developed bleaching device which enables performance and real-time monitoring of the bleaching process.
Materials and Methods
Specimen preparation
For this experimental setup, specially made pastilles of hydroxylapatite powder (Hydroxylapatite for analysis, ACROS Organics Co., USA) were used instead of human or bovine teeth, 13 as well as human teeth in in vitro conditions. Each pastille was made of 400 mg of hydroxylapatite powder which was compressed under the pressure of 20 bars. Afterwards, pastilles were dried in the dry sterilizer at a temperature of 150°C for 2 h to obtain the strength. Each of the pastilles was 10 mm wide in diameter and 2 mm thick.
Four extracted maxillary central incisors were used in this study. They were free of dental caries, calcifications, and restorations and had similar pulp chamber morphology. The teeth were cleaned and stored in 1% chloramine solution at room temperature immediately after extraction. The use of extracted human teeth was approved by the Research Ethics Committee of the School of Dental Medicine, University of Zagreb, Croatia. The root portions of the teeth were sectioned with a slow-speed diamond saw (Isomet, Buehler Ltd., Lake Bluff, USA) ∼2 mm below the cementoenamel junction perpendicular to the long axis of the teeth, and stored in deionized water until used. The pulpal chamber was cleaned of remanent pulpal tissues. The labial surfaces of the teeth were thoroughly pumiced for 2 min, rinsed in distilled water, and dried with clean, compressed air.
To create stained specimens, pastilles and teeth were immersed in the tea solution for 4, 6, 8, or 10 h. The solution was made from 2 g of green tea (Cedevita, Croatia) boiled in 100 mL of distilled water for 5 min. 14 Bleaching was performed using 25% HP gel (ZOOM 2, Discus Dental, USA). Bleaching gel was applied to the surface of pastille as well as to the surface of teeth specimens in a layer ∼2 mm thick.
Experimental bleaching setup with real-time monitoring of the bleaching process
The point of the experiment was to show that this newly developed setup is capable of separately monitoring the bleaching of several pastilles/teeth at the same time and in situ. Complete setup for this new type of bleaching device was assembled and developed in the laboratory for femtosecond laser physics of atoms and molecules at the Institute of Physics, Zagreb, and is patent pending.
15
The same setup was used for pastilles as for human teeth. The setup is depicted in a simplified schematic on Fig. 1a, and it consists of the following parts: 1. Holder for pastilles/teeth (developed at the Institute of Physics, Zagreb) 2. White LED for monitoring (YSL-R547W2C-A13; China Young Sun LED Technology Co., Ltd.) 3. Ultraviolet LED (UV LED) for bleaching, with center wavelength of 405 nm (YSL-R547P4C-E3; China Young Sun LED Technology Co., Ltd.) (Hereafter LED405) 4. Multitrack optical fiber and wires (from laboratory supplies) 5. Camera (DCC1240C - High Sensitivity USB2.0 CMOS Camera, 1280×1024, Global Shutter, Color Sensor; THORLABS Inc.) 6. Controller (developed at the Institute of Physics, Zagreb) 7. Computer
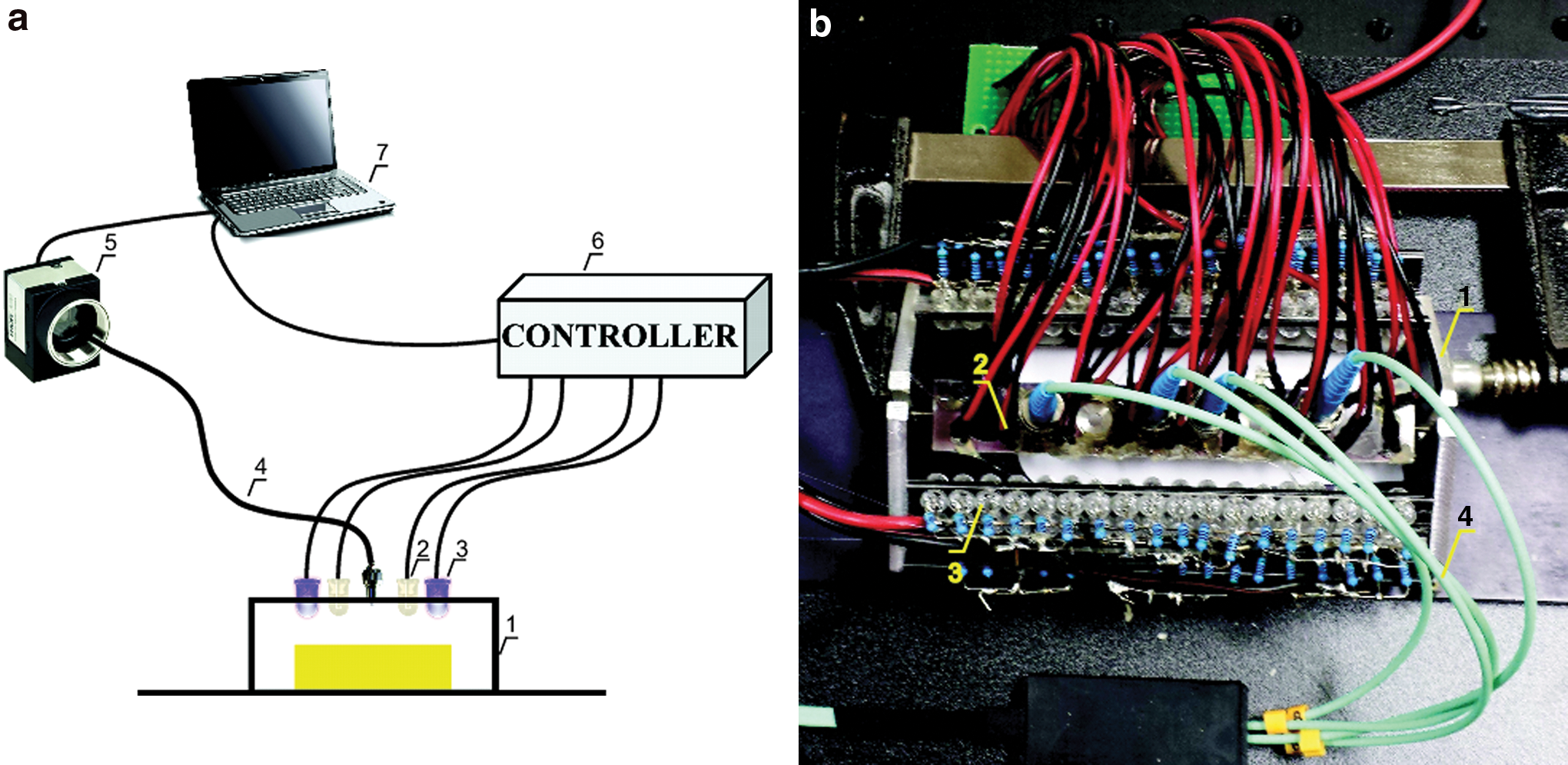
Part of a real setup showing pastilles holder, LEDs and optical fibers is presented in Fig. 1b. Pastilles/teeth cannot be seen, because they are under the plate holding UV LEDs and optical fiber connections. For easier visualization, the scheme in Fig. 1a shows the experimental bleaching process for only one pastille/tooth (yellow rectangle), whereas the experiment was simultaneously conducted on four pastilles/teeth. Each pastille/tooth was illuminated with 18 UV LEDs, whereas only two are displayed in the scheme (in violet color). The setup for each pastille/tooth also consists of two white LEDs for monitoring (displayed in white) and one multitrack optical fiber. The wires, camera, controller, and computer are also shown (Fig. 1b). In the real experiment, with four pastilles/teeth, all LEDs were connected to the same controller and all fibers were connected to the same camera.
The controller has the function to independently switch the UV LEDs on and off for bleaching on different segments, to provide a faster or slower bleaching process within a specific segment; that is, each pastille. In that way, the bleaching process can be specified individually for each pastille/tooth. A multitrack optical fiber was used to guide a light from all pastilles/teeth to the camera at the same time. The optical fiber was positioned in such a way as to prevent coupling light directly from the white LEDs for monitoring, and to enable only coupling light, which is reflected from the pastille/tooth. That light was guided to the camera. When taking a snapshot, the controller turned off the UV LEDs and activated the white LEDs for monitoring. Recorded data were sent to the computer for analysis. Because the controller was connected to the computer doing the analysis, it was possible to form a feedback loop for controlling the process.
A K-type thermocouple with digital thermometer (Termopar Digital Multimeter, Tektronix DMM 916, USA) was used to measure the temperature increase on the surface of extracted upper incisors, obtaining the average for each specimen. The tip of the K-type thermocouple was in close contact with whitening gel on the tooth surface. The temperatures were recorded at 5 time points: before, and 5, 10, 15, and 20 min during light activation. The collected data were monitored in real time. Measurements were made at a room temperature of 24°C.
Color change measurements and data analysis
Several sets of differently stained pastilles/teeth (n=4 in each set) were bleached for 20 min, during which the camera recorded pictures at specified intervals. Pictures were taken before the beginning, and afterwards every 5 min, until the end of bleaching process, leading to five images in total for each set of samples. The four regions of interest were located in each picture and are represented by a matrix of 30×30 pixels. Each matrix was assigned to a corresponding pastille. Analysis was performed using the program Wolfram Mathematica, which converted the data to corresponding RGB components. In order to facilitate data interpretation, the RGB index was formed as the sum of colorimetric values R+G+B (red+green+blue). 13 RGB-based measurements are widely used for color determination in dentistry. 16,17
Results
The resolution of a camera is 1280×1024 pixels, but region of interest that belongs to four pastilles is 382×41 pixels, and shows four light points recorded on the dark background. Each light point corresponds to a light reflected from each of the four pastilles during the bleaching process. The diameter of the region of interest for individual pastilles was set to ∼30 pixels, which resulted in an area of the region of interest for each individual pastille of ≈103 pixels. Statistically, RGB components for those ≈103 pixels were averaged, which was enough for defining the shade of a certain pastille. A total of five images (the first one made a few seconds before the beginning and then after 5, 10, 15, and 20 min of bleaching) were produced showing the changes in shade for all four pastilles. During bleaching with 25% HP activated by UV LED light, each of the five regions of interest (each region is a picture with a resolution of 382×41 pixels) was becoming lighter. Those regions of interest for one set of four pastilles are presented in Fig. 2 in black and white, for easier visualization of the change in contrast. Real images were recorded in color.

Reflections of white light from the set of four pastilles (shown in separate columns) before the bleaching process and after 5, 10, 15, and 20 min of bleaching (shown from top to bottom).
Figure 3a shows change in the individual R, G, and B components of a single pastille during the bleaching process. After 20 min of bleaching, these values increased by 42%, 56%, and 50%, respectively, compared with their baseline values. Fig. 3b shows measurements for one set of four pastilles where the change in the RGB index during 20 min of bleaching was presented. Results show an increase of the RGB index for all pastilles. The RGB index of 575 was determined as a desired color shade (Chromascop shade guide, Ivoclar Vivadent, Liechtenstein), and was marked as reference color A1. This reference color then determined the bleaching critical stopping time for each individual pastille. For this set of pastilles, the duration of bleaching to achieve A1 reference color for pastille 1 was almost exactly the predetermined bleaching time of 20 min. However, for the other pastilles, the optimal bleaching time was quite different. The desired value of the RGB index was reached after only 8 min for pastille 2 and after ∼14 min for pastille 3 (Fig. 3b, marked by vertical dashed lines). On the other hand, the bleaching process for pastille 4 should have lasted for >20 min to achieve a satisfactory result. In this experiment, the feedback loop was not operational, and all pastilles were bleached for 20 min to demonstrate dramatic differences in the final result.

To demonstrate the possibility of this setup to monitor the bleaching process of human teeth in real time, the same experiment was conducted using four human teeth (Fig. 4). Figure 4 shows the change in the RGB index during the 20 min bleaching process. The observed change in the RGB index was smaller than for the pastilles; however, it was still detectable. For both pastilles and teeth, the reference color was set to A1 (RGB index of 575). Tooth 3 reached the reference color A1 after a full 20 min of bleaching, whereas tooth 4 reached this value after only 3.5 min of bleaching (Fig. 4 dashed line). Teeth 2 and 1 did not reach the reference color A1 during 20 min of bleaching. It is interesting to note that teeth 2 and 3, which at the beginning had almost the same RGB index value (ΔRGB=5), had, at the end of the bleaching process, significantly larger difference in RGB index (ΔRGB=13). A similar and even more pronounced effect can be noted for pastilles 1 and 3 in Fig. 3a.
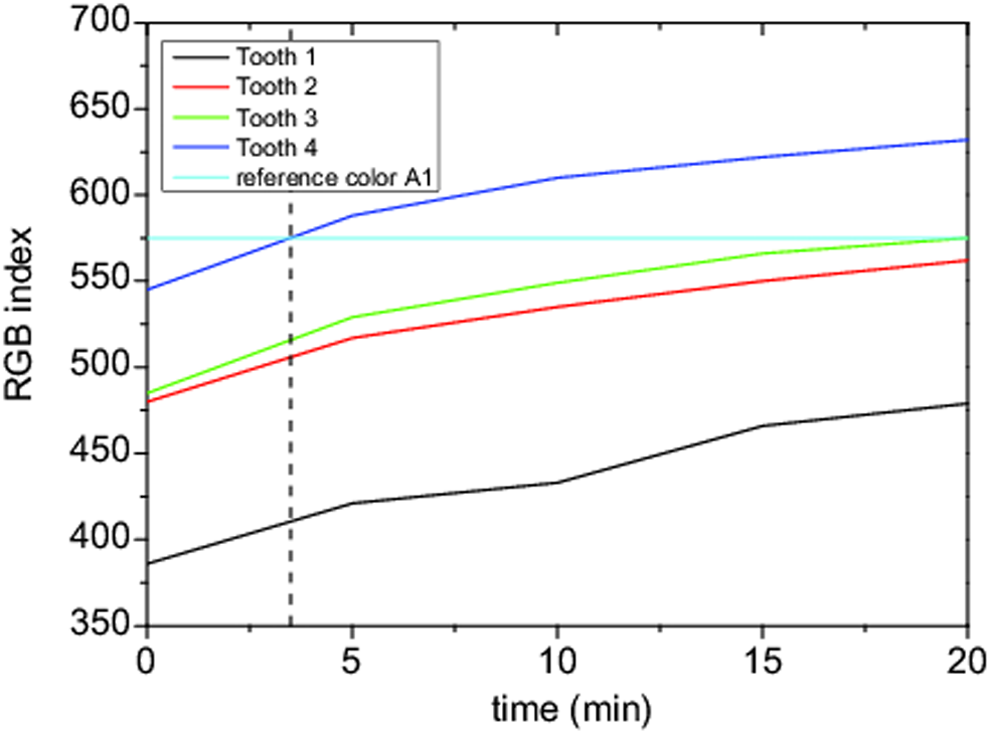
The change in the values of the red, green, and blue (RGB) index during the 20 min bleaching process for the set of four teeth.
The average temperature increase from baseline (24°C) was ∼4°C during treatment with UV LED light source and application of a 25% hydrogen peroxide bleaching agent to the tooth surface.
Discussion
Human and bovine teeth are quite different in their color, composition, size, and shape; therefore, standardized bleaching procedures are subject to a number of external factors that affect the results, in addition to the bleaching procedure itself. None of the existing studies provided a reliable solution to the deviating outcomes of bleaching or ensured local control accommodating variations in the tooth-to-tooth characteristics. These issues could be addressed by real-time local monitoring of the bleaching process, which is presented in this study.
In this in vitro study, hydroxylapatite pastilles as well as human teeth were used to demonstrate the potential of the presented experimental setup. Pastilles, which have a makeup similar to the greatest part of hard dental tissue, served as experimental objects because they are almost equal in their composition, size, and shape, and therefore are more reliable in testing the bleaching effect. As pastilles have an even and smooth surface, which is required for testing by some of the most advanced instruments (e.g. spectrophotometers), the color change measurement could be more precise. Nevertheless, real human teeth were used to corroborate the effectiveness of the setup.
The setup used was designed to accommodate four samples, either pastilles or teeth, where the LEDs for whitening had the potential to switch on and off independently on each segment, providing local control. The color change on each sample was recorded using optical fibers for every sample connected to a camera, thus ensuring local monitoring. The pastilles/teeth used in each measured set were stained differently, mimicking the naturally occurring discolorations of human teeth. The change in the sample color, that is, the RGB index value, for the set of four pastilles and the four teeth is presented in Fig. 3b and 4, respectively. Both graphs, as expected, show a similar trend of increase of the RGB index value during bleaching. The difference between pre- and post-RGB index value is somewhat higher for the measurements involving pastilles than for the results for human teeth. Nevertheless, the effect of bleaching on teeth is clearly detectable and measurable.
RGB index value versus bleaching time in Figs. 3b and 4 also demonstrates that the difference in the color between individual pastilles/teeth prior to the bleaching remains even after the bleaching, in the case of a non-locally performed process, and without feedback. This consequently results in a discoloration between pastilles/teeth. For example, in the case of tooth 4 in Fig. 4, the bleaching should have ended after 3.5 min. Tooth 3 required 20 min of bleaching, whereas teeth 1 and 2 needed >20 min of bleaching to reach the desired color (reference color A1). Additionally, even when the starting colors of two or more teeth/pastilles were similar, the final difference in the RGB index may be great as was visible for teeth 2 and 3 in Fig. 4, and, even more dramatically, as as visible for pastilles 1 and 3 in Fig. 3b. The difference in color between pastilles/teeth is very common during the bleaching process, and can be easily avoided using this setup. By connecting the controller and the camera to the computer, the feedback loop can be created to turn the LEDs on and off at each moment, for analyses and bleaching locally (individually) every tooth. The process of analyzing can be performed very frequently (>100 times) during bleaching, because of the extremely short time required for analysis (<1 sec). In addition, the apparatus can be allocated to any number of locations (for example on each tooth).
Measurements were performed on several sets of pastilles and teeth, and each set consisted of four samples. The measured effect of the rising RGB index value during bleaching was observed in all sets of samples. It is important to note that the statistical analysis of these measurements, such as to average the RGB index of several pastilles, is meaningless here. The aim was to show the ability to measure the RGB index of each pastille/tooth prior, during, and after the bleaching process. Additionally, we wanted to show that it was possible to determine the time required for each pastille/tooth to reach the desired reference color.
Application of 25% hydrogen peroxide gel in combination with UV LED light resulted in an average surface temperature increase of ∼4°C. Zach and Cohen 18 found in a monkey model that a 5.5°C temperature rise in the pulp chamber was likely to cause irreversible pulpal damage. Baldissara et al. demonstrated that an intrapulpal temperature rise between 8.9°C and 14.7°C in humans did not produce pulpal pathology, and that the cause of the postoperative sensitivity was the result of modification of the dentine. 19 The light source tested in this study resulted in a temperature increase below the mentioned thresholds; therefore, there is no potential danger when using this type of light activation. Temperature rise was measured on the tooth surface, not in the pulp chamber, which is difficult to achieve, especially in vivo, but the isolation effect of the enamel and dentin between the tooth surface and the pulp chamber served as an isolation layer; therefore, the assumed intrapulpal temperature should be even lower. Also, the effect of an intact pulpal circulation is being able to dissipate some of the applied heat. 20 Michida at al. 21 concluded that the mean temperature in the group activated with laser Nd:YAG (4.3°C) was significantly higher than that in the group activated with halogen light (1.8°C) and the group activated with LED light (0.9°C). Asmussen and Peutzfeldt 22 concluded that halogen light induced a higher temperature than LED, whereas Eldeniz et al. 9 found that the diode laser induced significantly higher temperature increases than any other curing unit (11.7°C). The LED unit produced the lowest temperature changes (6.0°C). Klaric et al. 10 found that the surface or intrapulpal temperature for commercially used whitening appliances such as ZOOM2 can be very high (16–23°C), whereas for the UV LED, the temperature in the pulp chamber as well as on the surface was 3°C, which was in accordance with the results of this study (4°C). Bleaching activation with UV LED promotes low temperature variation on the tooth surface, and can be used safely, without risk of overheating.
In addition to the lack of local color and temperature control, today's bleaching procedures suffer from a mostly subjective determination of tooth color when the shade guide is used. The shade guide and the tooth are observed at the same time under the same lighting conditions. Conditions such as environmental circumstances, light, experience, age, and tiredness of the human eye, and potential physiological characteristics of the observer such as color blindness, can lead to discrepancy, partiality, and inconsistencies among different observers. 23,24 Such subjective determination of the primary tooth shade and the time to reach the desired shade can easily lead to overbleaching. On the other hand, instruments such as spectrophotometers and colorimeters, which by themselves do not provide real-time monitoring, are primarily intended to measure the color on even and flat surfaces, and the surface of a tooth is rarely like that. 25,26 The setup presented in this study not only provides reliable and reproducible determinations of the tooth color, but it also functions on uneven surface of the tooth, and provides real-time monitoring of each tooth separately. In this way, effects such as overbleaching, color variations among teeth, and even some effects of long- term bleaching such as excessive heat, pulp irritation, necrosis, and postoperative sensitivity, can easily be avoided.
This setup could be additionally miniaturized and technologically improved to fit into a patient's mouth, and provide real-time monitoring and control over the color of each tooth, making for easier device handling and usage during both in-office and at-home bleaching treatments.
Conclusions
Contrary to the so-far known bleaching procedures that cannot simultaneously monitor and perform the bleaching process, or provide any local control over bleaching, the experimental setup presented in this article could fill that gap. The setup shown in this study ensured local and real-time monitoring of the bleaching process, while not being limited to flat surfaces such as spectrophotometers or colorimeters, and can be reproducibly used on any type of surface. By using such a setup, the bleaching process can be completely responsive to the characteristics of every individual, leading to more satisfying results. It provides essential information about when to stop the bleaching process if the surface temperature is too high, or to achieve the desired results. Furthermore, the bleaching process can be adjusted to accommodate the needs of a specific segment; that is, a particular tooth. In that way, faster or slower bleaching processes within each segment can be performed. Therefore, the setup presented here could ensure uniform bleaching of teeth, and prevent excessive and unwanted bleaching effects such as inconsistent bleaching, overheating, or postoperative sensitivity.
Footnotes
Acknowledgments
This study was supported by agency BICRO project No. PoC4_01_15, and Croatian Science Foundation (Project 08/31, Evaluation of new bioactive materials and procedures in restorative dental medicine).
Author Disclosure Statement
No competing financial interests exist.