
Abstract
Introduction
O
Since the first description of the oval window fenestration by Shea 1 in 1956, several surgical techniques and materials have been used in stapes surgery to reduce inner ear damage as much as possible. After the introduction of the laser in otology in 1967 by Sataloff, 2 many articles on the use of different lasers in otosclerosis surgery 3 –5 have been published. In the literature concerning diode laser in stapedotomy, only a few works are available: Feng et al. 6 compared diode laser and microdrill for stapedotomy, and Nguyen et al. 7 and Gerard et al. 8 described a low-power nonexclusive diode laser stapedotomy. After analysis of the characteristics and physical tissue interaction of this kind of laser, we decided to use it in stapedotomy with a high power and short time single pulse approach. This choice aimed to use the right amount of energy to ablate the footplate, ideally in one shot, minimizing thermal damage in the inner ear.
The diode lasers used had a wavelength of 940 (Dornier Medilas D 940 nm 60 W) and 980 nm (DEKA SmartXide2 diode module 980 nm 50 W) delivered through a 0.6 mm fiber diameter tip providing maximum handling and accuracy on the target structures. The aim of this study was to evaluate the preservation of the inner ear function as well as its effectiveness, comparing the surgical results with those already published concerning different techniques.
Materials and Methods
This study was approved by the Review Board of the Humanitas Clinical and Research Hospital of Rozzano, Milan, Italy, in accordance with the Guidelines for Protection of Human Subjects. From January 2004 to December 2012, 179 diode laser stapedotomies were performed as primary procedures by the same senior surgeon (A.M.P.). The population included 69 males and 110 females with an average of 45.11 years (range 23–78 years). In this group, 22 patients underwent surgery on both ears, with an interval of at least 6 months between each operation. Preoperatively, 107 patients complained of tinnitus, 27 complained of dizziness, and in 11 cases vertigo was present. Indication for surgical management of otosclerosis included conductive or mixed hearing loss with a >25 dB pure tone air-bone gap (PTA-ABG). Otoscopy and tympanometry were normal, and the stapedial reflex were absent in all cases. A preoperative high-resolution computer tomographic (CT) scan of the middle ear was performed in all cases, no anatomical variation was detected, and all patients were classified in Symons/Fanning 9 grade 1. Hearing was represented at four frequencies: 0.5, 1, 2, and 4 kHz. Postoperative hearing evaluation was: bone conduction only the day after surgery, air and bone conduction at 1 month, and up to 8 years annually.
We made a comparison between the preoperative and 1 month postoperative pure-tone bone conduction thresholds (PTA-BC pre, PTA-BC post) and observed the ABG pre/post at 4 kHz, the high frequency sensorineural hearing changes at 4 kHz (variation in BC), and 8 kHz air conduction (8 kHz AC pre, 8 kHz AC post) and PTA-ABG pre, PTA-ABG post. The residual ABG after surgery was subdivided into three groups: group A with ABG <10 dB, group B with ABG between 10 and 20 dB, and group C with ABG >20 dB. Records of the patients were also analyzed for tinnitus, vertigo, and dizziness.
Diode laser physical properties
We used a diode laser that emits in the near-infrared spectral region (λ = 940 nm) and from 2011 we used also a new diode laser with λ = 980 nm. In this zone, tissue optical properties are principally characterized by diffusion and, as a consequence, the depth of penetration of laser radiation, between 1 and 5 mm, is caused by the phenomenon of multiple diffusion. For the laser–tissue interactions caused by the relationship between exposure time and irradiance (W/cm2) with constant fluence (J/cm2), the therapeutic effect obtained (with 40 W and 60 ms) is essentially photothermal. Photothermal interaction is based on optical energy conversion into thermal energy. Generally, in biological tissues, different thermal effects are produced: from hyperthermia (temperature between 43 and 50°C), to denaturation of protein and collagen (55°–80°C), to vaporization and thermal decomposition (T >100°C). The laser parameters were set up as follows: 40 W laser power, 60 ms exposure time (tL), and 0.6 mm spot diameter, resulting in a fluence and an irradiance of 218 J/cm2 and 3636 W/cm2, respectively. As the bone thermal conductivity is low (K = thermal diffusivity coefficient of skull @ 0.0043 cm2/s ec 10 ), laser effects are depleted within the volume of the treated tissue. If we evaluate the propagation length of the thermal wave Lth within the selected exposure time tL, we obtain the value of Lth = (4 × K × tL)^1/2 = 321 μm, comparable with the stapes footplate thickness, ranging between 178 and 388 μm, 11 with the result of no theoretical inner ear thermal damage. Moreover, as the laser exposure time is lower than the bone tissue thermal relaxation time (tT), heat cannot spread in the bone tissue for a length greater than the typical optical penetration depth (Leff). If we assume that for bone tissue Leff = 2.84 mm 12,13 at 940 nm, and we obtain that bone tissue thermal relaxation time is tT = (Leff)2/4K = 4.70 sec, as tL (60 ms) < tT (4.70 sec), heat is confined in the irradiated volume. When using a 980 nm diode laser, the optical penetration depth is Leff = 1.87 mm 14 , resulting in a shorter relaxation time: tT = 2.4 sec.
The laser beam is conveyed by an optical fiber with an active part of 0.6 mm diameter, introduced in a malleable hand piece.
Surgical procedure
Local anesthesia was used in 23 patients, and general anesthesia was used in the remaining patients.
The diode laser stapedotomies were generally performed with the power set at 40 W, and an exposure time of 60 ms. One shot stapedotomy was performed in 23% of cases, two shots were used in 51%, three shots were used in 16%, and in the remaining 10%, more pulses were needed. The mean energy applied to the footplate was 4 ± 0.3 J. The stapedotomy diameter obtained was slightly larger than 0.6 mm, enough to place a 0.6 mm diameter fluoroplastic prosthesis. Diode laser surgical technique does not differ much from the conventional stapedotomy with a drill or manual perforator. An endaural approach is used. A skin incision between the tragus and the helix as described by Fisch, 15 canalplasty, was made, if needed. The elevation of the tympanomeatal flap was performed. The ossicular chain mobility was always checked.
The vaporization of the stapedial tendon and the posterior crus by laser was performed after incudostapedial joint separation. The anterior crus was fractured using an angled hook; the distance between the footplate and the lateral surface of the incus was then measured with a sliding rod. The diode laser stapedotomy was performed, and a 0.6 mm diameter fluoroplastic prosthesis was placed. The oval window niche was sealed with connective tissue or fresh venous blood.
Statistics
Data were tabulated using Microsoft Excel 2002 (Microsoft corp., Redmond, WA). Analysis was performed with the statistical package STATAT version 9.0 (StataCorp College Station, TX). The statistical significance of the results was expressed with the Wilcoxon test.
Results
Postoperative hearing results were obtained the day after the procedure (only bone conduction), at 1 and 12 months, and then yearly.
No bone conduction worsening was detected in the day after surgery. The mean PTA-BC pre was 24.22 dB (±8.7 SD), whereas the mean PTA-BC post was 21.11 (±9.1 SD). In our series the 8 kHz AC pre average was 56.41 dB (±22.86 SD) and the 8 kHz AC post was 52.56 dB (±24.35 SD
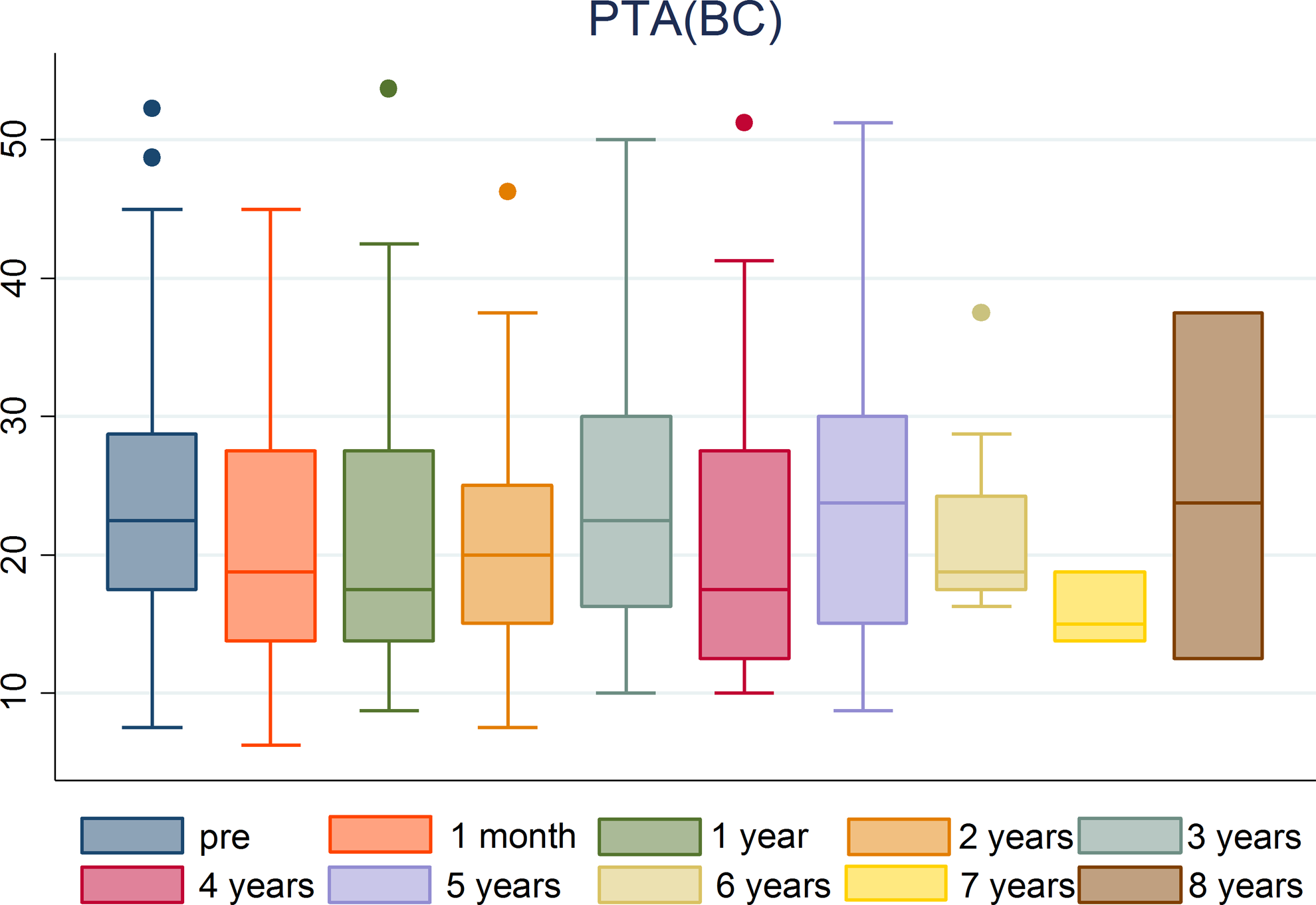
Postoperative pure tone average bone conduction (postop PTA-BC).

Postoperative air conduction (AC) 8 kHz.
The mean preoperative PTA-ABG was 27.43 dB (±7.58 SD), whereas the PTA-ABG post at 1 month was 5.23 dB (±5.00 SD). The ABG closure at 1 month (six cases lost at follow-up) within 10 dB was achieved in 89.02% of the cases, within 20 dB in 97.69%, and >20 dB in 2.31%. Late audiometric postoperative evaluations at 12 months and then yearly had no statistically significant variations over long-term follow-up (Fig. 3A). The analysis of 4 kHz shows a statistically significant improvement in postoperative ABG (Fig. 3B).

A total of 107 (59.77%) patients reported preoperative tinnitus; in 72 (67.28%), tinnitus disappeared postoperatively. We observed that two (1.11%) patients, who did not complain of tinnitus preoperatively, developed tinnitus after the surgical procedure. In both, tinnitus started a few days postoperatively and disappeared after a few months. Dizziness before the operation was present in 24 (13.4%) patients; in postoperative group a transient dizziness was noticed in 19 (10.6%) patients.
Preoperatively, vertigo was present in 11 (6.1%) patients. Postoperatively, 21 (11.73)% of patients complained of mild vertigo, and only two of these showed nystagmus: one had paroxysmal positional vertigo treated with the Semont maneuver, and in the other, vertigo appeared 4 days after the surgical procedure and completely disappeared in 2 days.
In the local anesthesia group, only three (13.04%) patients complained of transient vertigo during the operation. The vertigo was not related to the number of the spots (from one up to three spots).
The bone conduction hearing threshold, performed on these patients the day after surgery, showed no clinical variations. No postoperative sensorineural hearing loss (SNHL) occurred in this series. All the patients were discharged the day after the surgical procedure in the absence of vestibular symptoms. As a long-term complication, we observed one case of necrosis of the incus 8 years after the procedure: the patient underwent a successfully malleostapedotomy with a Fisch titanium piston; and one case of sudden hearing loss occurred 7 years after surgery.
Discussion
During the past 25 years, different laser systems have proven to be an interesting alternative to the conventional methods in stapes surgery. They allow a precise window into the footplate with less trauma to the labyrinth. Removal of the stapes superstructure is easier, a floating footplate is usually avoided, and an obliterated window can be properly approached. A recent article by Wegner et al. 16 reviews the existing literature comparing traditional versus laser footplate fenestration, stating that both footplate fractures and sensorineural hearing loss appear to occur more frequently in the conventional group than in the laser group. Therefore, laser is preferred over conventional methods for footplate fenestration in primary stapedotomy. Several authors describe the successful use of other types of laser such as carbon dioxide (CO2), 17,18 potassium–titanyl–phosphate (KTP), 4 Argon, 19 and Erbium, 20 whereas there are still only a few reports on the use of diode laser for stapes surgery. Gerard et al. 8 used an 808 nm wavelength diode laser in multiple shots and with fibers with a small diameter in continuous mode at 1 W, with the aim of weakening the footplate before creating the stapedotomy with a microdrill. Feng et al. 6 concluded that diode laser, if compared with microdrill, has better results and reduces the incidence of complications. The technique of multiple shots is called “Rosette technique,” and is the one still widely used with different kind of lasers. Nguyen et al. 7 used a 940 nm wavelength diode laser set at 3 W with 200 ms pulse duration using a 0.6 mm diameter fiber, to obtain the initial stapedotomy, and then enlarged it with a microdrill. Nevertheless, this technique, as well as the “Rosette” one, does not avoid the final use on the footplate of mechanical pressure of the microdrill, which removes all the advantages of the laser itself.
The first attempts at realizing the fenestration with a single impulse were performed with a defocused CO2 laser laser beam, 21 and then Jovanovic et al. 18 first introduced the concept of the “one shot” stapedotomy, adding the use of a scanner to the traditional micromanipulator, performing with the focused laser beam a quick single spiral motion adjustable to the desired dimension, with the CO2 laser emitting in continuous mode to avoid the acoustic effect generated by the pulsed emission. High energy over a short time was applied in order to produce the stapedotomy without the aid of other mechanical tools. In accordance with this philosophy that allows the use of the laser alone, in our series we decided to use the diode laser with a high power (40 W) and a low exposure time (60 ms) in order to avoid thermal damages. The mean energy applied to the footplate was 4 ± 0.3 J on a 0.6 mm spot (fiber diameter). The short exposure time limits the thermal conduction, and all the energy is used to vaporize the bone quickly, not heating the perilymph (that is also not the elective chromophore of these diodes' wavelengths) or reaching the inner ear organ. Fibers of different diameters can provide holes of different sizes, for various kind of prostheses, taking care to give the footplate the right amount of energy density, reducing appropriately the time of emission.
A statistically significant improvement of the PTA-BC and the hearing loss at 8 kHz AC was observed. High frequency worsening is still debated, and up to 6.5% is reported. 22,23 Too many factors are involved (surgical trauma, perilymph leakage, loud sounds generated by microdrill). We considered this frequency as an initial sign of inner ear distress, and the improvement in our series could be related to the absence of acoustic and thermal side effects of the laser setting used.
We observed that number of spots and the Joules applied at the footplate did not induce any variation in the hearing results (Figs. 4 and 5): if we analyze the relationship between the number of Joules and the footplate spot number with the preoperative/postoperative PTA (BC) at 1 month, we did not observe any significant variation. We had only six cases with a slight BC 4 kHz worsening (statistically nonsignificant). In one case with a thick footplate, we dismissed 16 J seven spots without PTA (BC) and 8 kHz worsening. Compared with CO2, advantages of this type of laser are the ease of operation without the need the use of an articulated arm, micromanipulator and scanner mounted on the microscope that increase the weight and reduce its manageability, and, principally, the need to perfectly focus the laser beam from the zoom of the micromanipulator CO2 laser. Noncontact technique remains suggested for revision stapedotomies and treatment of the floating footplate. However, with diode laser we successfully treated two floating cases simply placing, without pressure, the fiber tip on the footplate.
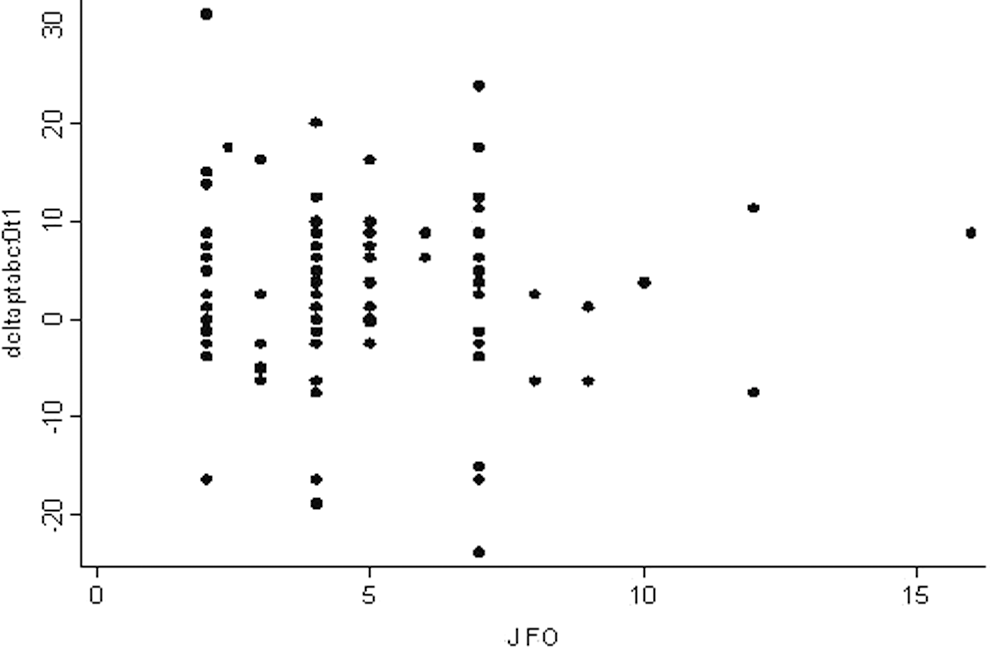
Variations in pre-postoperative bone conduction related to joules dismissed.
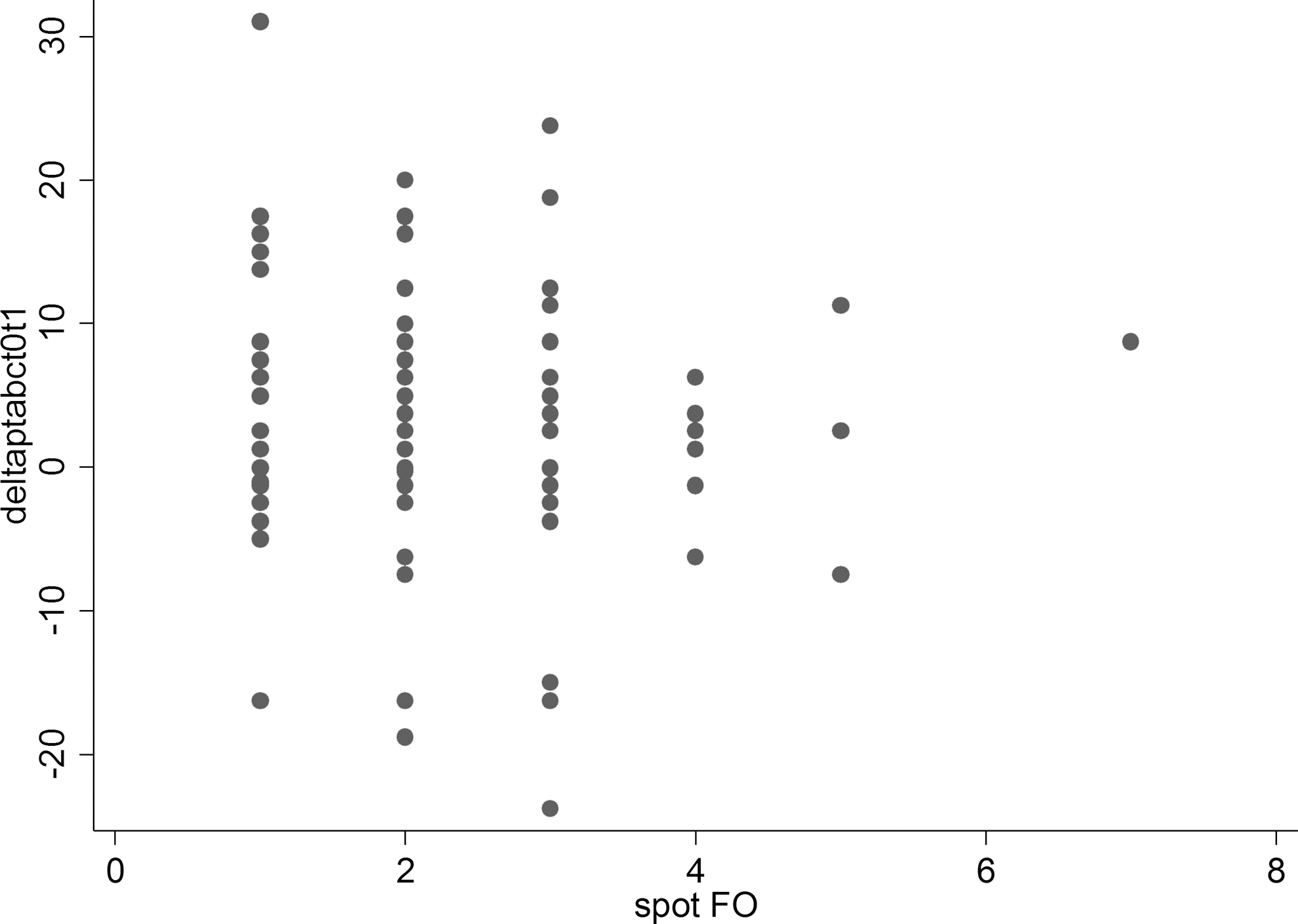
Variations in pre-postoperative bone conduction related to the number of spots.
Significant in our series is the absence of a transient lowering of the bone conduction thresholds in the immediate postoperative period, as reported in previous articles, 15 and also a statistically significant improvement of the PTA-BC post, according to the Wilcoxon test. The statistically significant improvement of the postoperative bone conduction as well as postoperative air conduction at 8 kHz and the absence of postoperative SNHL give evidence as to the safety of the procedure itself, according to other authors. 22,23 Our hearing results are coherent with those of other traditional or laser stapes surgery series reported in the literature, with stability in long-term follow-up 17,24,–33 (Table 1). In a recent article, Kamalski et al. 5 have tested the thermal, mechanical, and acoustic effects of a 980 diode laser in an inner ear model, demonstrating that these effects are limited and all within safety limits. The article also explains what was known from the studies of van Gemert et al. 34 : diode laser wavelengths from 800 to 1064 nm (especially ∼810 nm), can be dangerous in the inner ear if used in CW mode with long exposure. If this is >100 ms, the thermal relaxation time of the tissues concerned, being poorly absorbed by the water and absorbed by hemoglobin and melanin, their radiation passes the perilymph and can damage the inner ear.
Statistical significant difference: p < 0.05
Three groups: A = conventional technique; B = combination technique; C = erbium laser.
Two groups: A = 112 cases – 0.6 mm; B = 100 cases – 0.4 mm.
ABG, air-bone gap; SNHL, sensorineural hearing loss.
Conclusions
As suggested in previous works, 5,6,16 our clinical and audiological results confirm that laser stapedotomy, and this technique in particular, is safe and effective. The study allow us to exclude the possibility that diode lasers with the wavelengths and parameters used could be dangerous for the inner ear. The functional results at the short and late follow-up are coherent with those of other technique series. The lack of complications and the functional results validate the “one shot” technique, high power, and short time pulse diode laser stapedotomy (Fig. 6).
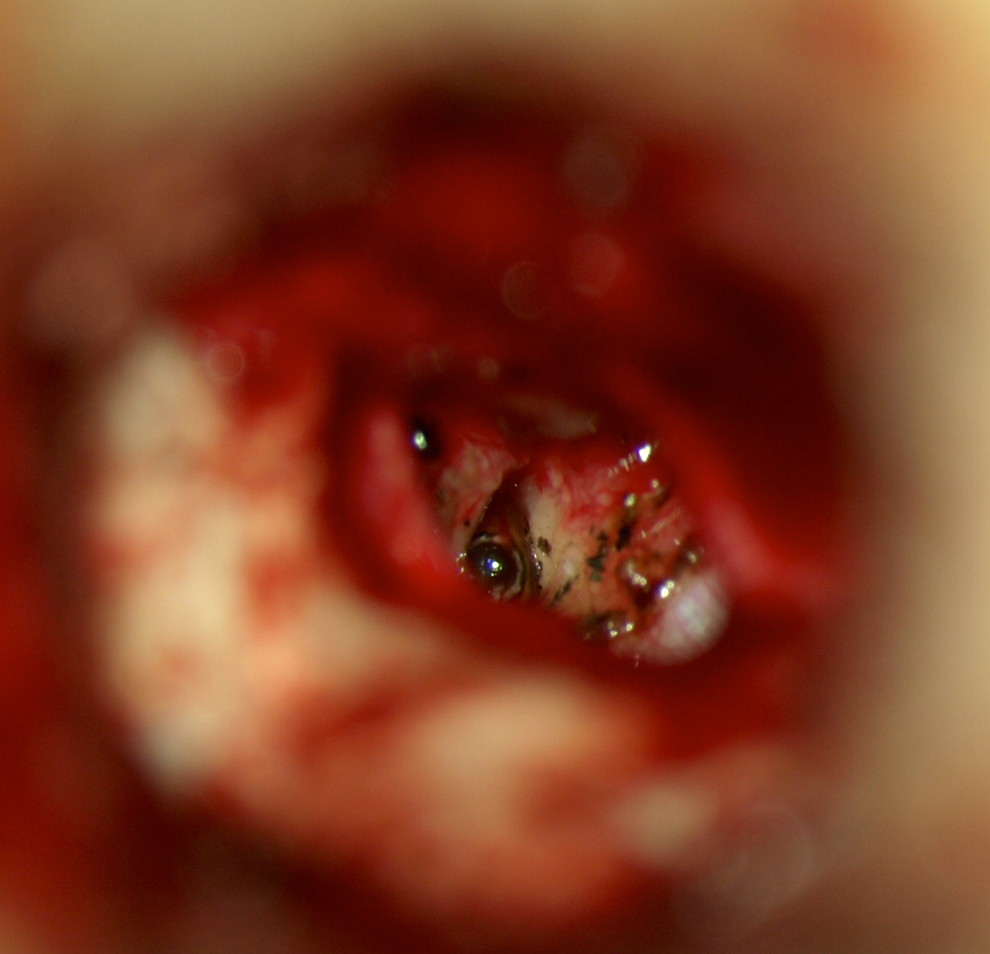
Diode laser stapedotomy.
Footnotes
Acknowledgment
The authors thank Jeane Vieira, audiologist from our department, Dr Siba Prasad Dubey of the University of Papua New Guinea, and Dr. Luca Giannoni for reviewing this article, and Dr. Emanuela Morenghi for the statistical analysis of the data.
Author Disclosure Statement
No conflicting financial interests exist.