
Abstract
Introduction
A
In 1955, Buonocore was the one who effectively gave a start to the transformations that changed the restorative techniques. The author observed that the application of phosphoric acid to human enamel could increase the retention of acrylic resins to the substrate. 8 Since then, many changes have been observed in restorative dentistry, both by researchers and practitioners. 9
Nowadays, with the fast development of adhesive systems and within the concepts of minimally invasive dentistry, direct restorations with composite resins are conservative procedures capable of rehabilitating the oral cavity, and should provide sufficient bond strength to the tooth to withstand the forces in the oral environment. 10
Since the studies of Nakabayashi et al., it has been known that a sufficient bond to dentin can be achieved by the formation of a hybrid layer. 11 The mineral phase of dentin is removed by acids, and the exposed collagen fibrils are infiltrated by hydrophilic monomers and polymerized in situ. According to the literature, strong bond strength values can then be achieved for resin composites. 5,7 Nevertheless, the heterogeneous, organic, moist nature of dentin and its morphological variations make it a complex substrate. 12,13 These aspects, concerning substrate morphology, lead to greater discussion in restorative dentistry.
The introduction of laser technology in dentistry opened new possibilities and strategies to conventional treatment with high and low speed rotary instruments. 14 –16 Considering the clinical aspects of the use of erbium lasers for caries removal and cavity preparations, some authors reported that treatment performed with lasers can be considered an efficient and feasible technique in clinical practice, without prejudice to the pulp tissues, and with wide acceptance by patients because of the reduced noise and vibration, reduction of pain sensitivity levels and, in some cases, lack of need for anesthetics. 17 –19 These advantages should be considered when adopting an erbium laser for cavity preparation, but correct parameters are recommended and mandatory to avoid an increase in temperature that can possibly damage the tooth structure. 20
Therefore, the aim of the present study was to conduct a review of the literature about adhesion on erbium laser prepared cavities, related to the specific conditions of the irradiated dentin substrate and the effects on bond strength values.
The literature review was conducted from 2002 to 2015 to identify sources of the importance of erbium lasers in bond strength. Electronic search engines for the Internet such as MEDLINE®/PubMed and Science Direct were used using the following search terms: high-power lasers AND (dentin OR enamel OR bond strength OR Er,Cr:YSGG OR Er:YAG) AND bond strength (dentin OR enamel OR laser high-power) AND dentin (bond strength OR high-power lasers) AND adhesion (high-power lasers). Only complete articles in English were taken into consideration. Reviews of the literature and original research articles were added. Articles related to deciduous teeth were excluded, similarly to those that studied indirect composite resins or ceramics.
Basic Principles of Lasers
Theodore Maiman introduced lasers in 1960. Since then, the application of lasers in various areas of health has gained importance among researchers and clinicians as having potential clinical benefits. The word “laser” is an acronym for Light Amplification by Stimulated Emission of Radiation. The acronym comes from the mechanism used for the production of laser light, which is based on the theories of spontaneous and stimulated emission of radiation, proposed by Albert Einstein in 1917. Understanding the mechanism of generation of laser light is essential, and allows understanding of the peculiarities of this radiation, compared with other available light sources. 21
As it is an electromagnetic radiation, photons of laser light propagate in space according to the trajectory of a wave. 21 –23 Electromagnetic radiation in the electromagnetic spectrum is classified according to wavelength (which is the distance between consecutive corresponding points of the same phase). 22 Observing the electromagnetic spectrum, lasers used in dentistry are primarily located between 500–1064 and ∼3000 nm, which comprises visible electromagnetic radiation (400–700 nm) and infrared (700–1060 nm). 21
Three important features differentiate laser from the other light sources: the monochromatic beam (photons emitted by a laser feature all the same wavelength), coherency (photons that make up the laser beam traverse exactly the same path in space and time, and therefore are synchronized), and collimation (laser light can be emitted unidirectionally, resulting in the propagation of the beam in one direction). These three characteristics are responsible for the interaction of this source of light with biological tissue. 21 –23
Laser interaction with tissue can occur in different ways: reflection, transmission, absorption, and scattering. Among these processes, the absorption is more important, because it is essential for the laser to induce the desired biological effects. The absorption depends on the affinity between the laser wavelength and the target tissue composition, occurring in the presence of substances capable of absorbing incident wavelength, called “chromophores.” 21 –23
Laser and Dental Hard Tissues
Biophotonics is an area of technological innovation that has been increasingly associated with dentistry, and its use is based on the various applications of lasers and light-emitting diodes (LEDs) as adjuncts in promoting health and minimally invasive intervention. Among these applications, the selective removal of caries in minimally invasive cavity preparations and the conditioning of enamel and dentin are included. 24 –27
The tooth structure removed is based on the principle of ablation, and uses photochemical, plasma-mediated and phototermal mechanisms. However, at present, tooth structure removal is based on the principle of thermal ablation. 26,28
Contrary to the commonly used method, laser irradiation involves minimal loss of dental tissue without vibration and heat, reducing the need for local anesthesia and increasing the patient's comfort, thereby making it an attractive option for patients and professionals. 17,19
Concerning the erbium lasers, there are two types for clinical use in the preparation of dental hard tissues: the Er:YAG (2.94 μm), and the Er,Cr:YSGG laser (2.78 μm
As mentioned previously, dental hard tissues can be effectively removed with the ablation process, which involves microexplosions, absorption by water vaporization, and removal of mineralized dental hard tissue. Microexplosions, however, produce the ejection of both organic and inorganic tissue particles, providing an irregular dentin surface with open dentinal tubules and no smear layer formation. 24,27,31 –34 These effects also extend to the dentin subsurface, forming a layer that is laser-modified by thermal denaturation. 31,34,35 This denatured layer created through laser irradiation has been considered to be responsible for the decrease in bond strength of adhesive systems to irradiated dentin. 32,36 –41
As erbium laser is mainly absorbed by water and other hydrated organic components of the tissue, and the difference in water content between peri-and intertubular dentin is responsible for the selective ablation of intertubular dentin by this wavelength, producing protruding dentinal tubules with a cuff-like appearance. 24,28,34,36,38,42
In enamel, laser irradiation promotes the exposure and/or removal of the prisms. 27,28,43,44 This modification in enamel is not as challenging as the changes produced in the surface of dentin, which can potentially affect adhesion to resinous materials, as will be describe in the next section.
Adhesion to Irradiated Tooth Structure
The mechanism of action of erbium lasers in mineralized tissues is associated with the phenomenon of ablation in which the incident laser beam is absorbed by the water molecules present in the dental tissue, causing rapid heating and evaporation of water, followed by successive microexplosions with the ejection of mineralized tissue. 28,45 Therefore, because of its wavelength, closed to the optimum absorption of water and hydroxyapatite, it is possible to use erbium lasers in conservative cavity preparations and selective caries removal. 15,24,27,28
The bond strength to laser-prepared dental hard tissues cited in the literature is often contradictory. Whereas some studies have shown that if a specific parameter is used, lasers can promote selective removal of carious dentin, bacterial reduction, conditioning of the tooth surface, and a microretentive morphological pattern that could possibly favor the bonding procedure, without thermal damage or signs of heating and melting, others have shown that these characteristics are not enough or could present a substrate less receptive to adhesive procedures than conventional bur-cut cavities. Figures 1 and 2 show the microretentive pattern of the surfaces ablated with erbium lasers (Er:YAG and Er,Cr:YSGG) and the formation of long, numerous resin tags with lateral branches that was possibly attributed to a satisfactory bond strength. De Moor and Delmé in 2010 reported that the heterogeneity in measuring energy outputs in the literature also complicates any interpretation and comparison of the current literature on this subject. 26

Cavities prepared with Er:YAG laser in dentin (Kavo Key laser 3).
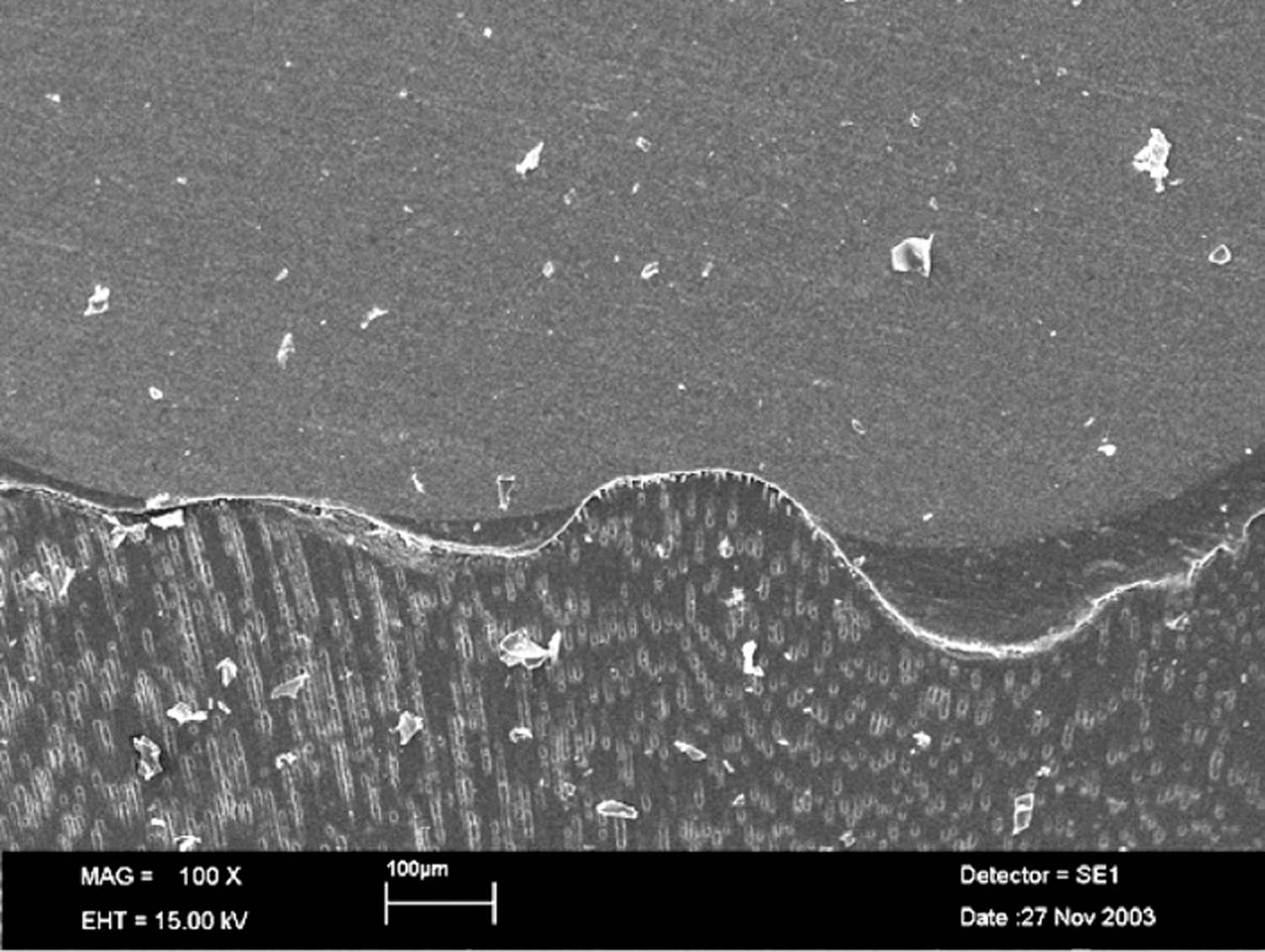
Dentin-resin interfaces of cavities prepared with Er,Cr:YSGG laser in dentin (Waterlaser, Biolase). Note the irregularities promoted by dental ablation (×100).
To begin with this topic, it should be stated that according to the parameter used and the condition of the tissue being irradiated, erbium lasers can promote the conditioning of the tooth surface or the removal of mineral-irradiated tissue for cavity preparation. 25,26
The conditioning of the surface, also named as “laser etching,” is a cavity pretreatment, usually performed at lower fluences that have been proposed as an alternative to acid etching of enamel and dentin. 14,46 –51 Bahrami et al. stated that dentin conditioning at a low fluence of 12.58 J/cm2 per pulse, with 80 mJ output energy and 50 μs pulse duration, can significantly improve tensile bond strength of a composite bonded to Er:YAG laser-prepared dentin. 52 The study of Gisler and Gutknecht 53 is in agreement with the previous one, stating that the only way to get an optimal microretentive bond pattern is by using laser fluences just above the ablation threshold, mainly in sclerotic dentin. The discussion clearly showed that in altered (sclerotic) dentin; for example, for class V fillings of elderly patients, bond strengths in conventional dentin adhesion are constantly reduced, whereas for Er:YAG-conditioned dentin, the only way to obtain an optimal microretentive bond pattern is a laser fluence just above the ablation threshold of sclerotic dentin. 53 Chen et al. showed that Er:YAG laser preparation did not compromise the efficacy of one step self-etch dentin adhesives, and that pretreatment with phosphoric acid or low-fluence Er:YAG laser can significantly increase the tensile bond strength of adhesion to this irradiated dentin. 48 Acid etching significantly increases the adhesion in laser-treated enamel and dentin, and this operative step should not be skipped. 54,55
Ramos et al. showed that surface treatment with Er,Cr:YSGG laser irradiation (at 4.5 J/cm2/50 mJ/30 Hz/140 μs) prior to bonding with a self-etching adhesive system significantly increases adhesion to eroded dentin, as compared with conventional treatment. 56
As mentioned, the difference in the composition of mineralized dental tissues results in a lower threshold for ablation for dentin in comparison to the enamel, since the former has a higher organic content. 28 Several studies assessing the quality of bonding in irradiated enamel to restorative adhesive materials have positive outcomes, showing that adhesion to enamel is not as problematic as adhesion performed in dentin. 38,57 –59
Amaral et al., when evaluating the bond strength of the restored cavities prepared with an Er:YAG laser, reached similar results to those found for cavities in dentin prepared with rotary burs, even after thermocycling and water storage conditions. 57 Ramos et al. also showed that the use of Er:YAG laser for ablating human dentin did not alter the main adhesion parameters when compared with those obtained by conventional methods, thus reinforcing its use in restorative dentistry. 60 Moreover, in 2012, Akin et al. also concluded that, within the limitations of their study, the bond to Er:YAG laser-irradiated dentin was similar to that of the bur-cut dentin. 61
According to Shahabi et al., the findings of the study showed that the tensile bond strength of the Er:YAG laser group was significantly higher than that of the bur-cut group, and that Er:YAG laser with the mentioned irradiation parameters could be an effective tool for dental hard tissue removal and cavity preparation. 62 Further, the bond strength of composite resin to dentin in Er,Cr:YSGG-lased cavities was approximately the same as that to bur-cut cavities. Da Silva et al. indicated that the tested adhesive systems promote similar shear bond strengths, whether the dentin was prepared with a diamond bur or an Er:YAG laser, and that an Er:YAG laser is a suitable cavity preparation method that promotes an adequate surface for a posterior adhesive procedure. 63 Ergücü et al. showed similar microtensile bond strength values to those of conventional bur treatment, regardless of the adhesive system and type of treated dentin. 64
Some other articles agree with the previously mentioned ones, supporting the clinical use of lasers in adhesive dentistry. 65 –67
On the other hand, many studies that focused on the quality of the bond strength of the new adhesive materials in lased dentin, found results that do not recommend the use of lasers in restorative dentistry due to negative results. 30,31,37,38,68,69 The resulting microscopically rough surface without demineralization, open dentinal tubules, lack of smear layer formation, and satisfactory sterilization of the cavity are described as advantageous for dentin bonding procedures. 70 –72 Figures 1 and 2 show the microretentive pattern of the surfaces ablated with Er:YAG and Er,Cr:YSGG lasers. However, Er:YAG and Er,Cr:YSGG irradiation interact with dental hard tissue, resulting in a specific morphological pattern of dentin and collagen fibrils, which negatively affects the bond strength to composite resin. 31,32,34,60,68 The statement that the microretentive pattern resulting from irradiation could favor the bonding procedures was not accepted in these articles. Table 1 presents the descriptions and results of the articles in which research was performed with Er:YAG and/or Er,Cr:YSGG lasers in dentin and enamel adhesion (from 2009 to 2015).
De Oliveira et al. showed that a nonuniform hybrid layer was created on laser-irradiated dentin surfaces regardless of laser irradiation protocol for all adhesive systems used, whereas regular and uniform hybrid layers was observed in the control groups. 34 “Stretch mark”-like red lines were found within the hybrid layers as a result of resin infiltration into dentin microfissures, which were predominantly observed in the 200 mJ/pulse groups regardless of the adhesive system. Poor resin infiltration into peritubular dentin was observed in most regions of adhesive interfaces created by all adhesives on laser-irradiated dentin, resulting in thin resin tags with neither funnel-shaped morphology nor lateral resin projections. 34 These data were also described by other articles. 36,47
Koliniotou-Koumpia et al. showed that dentinal surfaces treated with Er:YAG laser displayed lower bond strength values in almost every combination of the adhesive system and dentin depths used. 73 The authors stated that cavities prepared by laser seemed less receptive to adhesive procedures than did conventional bur-cut cavities. 73 Cardoso et al. revealed that mixed failures were more frequently observed in the laser-irradiated groups because of the prominent irregularities presented on laser-irradiated dentin. 5 De Munck et al. found cohesive fractures in dentin for the Er:YAG laser groups. Moreover, subsurface damage produced by laser can cause increased hybrid layer thickness and less remaining collagen to be exposed, and consequently, to be hybridized; therefore, an adhesive failure mode was observed in this study. 37
Many publications also report poor marginal adaptation with a high degree of microleakage. 26,74 –77
To overcome the low bonding values found for the irradiated dentin, some procedures were recommended. Initially it was observed that the lower values were the result of an increase in acid resistance, and that the time necessary for acid conditioning was not enough to demineralize and expose the collagen fibrils. However, recent studies show that this difference in the bonding interface pattern is not related to an increase in acid conditioning time, 78 but is possibly the result of the microcracks that can form in the subsurface of the irradiated dentin, when certain irradiation parameters are used. 35,79
Another point to be discussed is the different types of adhesive systems available for the clinicians (Table 1). De Oliveira et al. showed that the superficial changes promoted by surface treatments modified the way the different types of adhesive system interacted with treated dentin. 79 The laser-modified layer can impair the mineral dissolution by acid etching and resin adhesive diffusion into intertubular dentin subsurface, leading to a deficient hybridization and, consequently, to a lower bond strength. 32,37,80,81 De Oliveira et al. showed that the bond strength results for laser-irradiated dentin were the lowest values for Single Bond and Clearfil SE Bond adhesive systems. However, for Unifil Bond and Tyrian systems, the bond strength was similar to other means of dental preparations. 82 Also, it was observed that the laser-irradiated dentin samples tended to fail more cohesively in dentin, which is explained by the damage in subsurface that exceeded the thickness of hybridization, leaving a weakened substrate. 83 Some other studies also stated that dentin surfaces prepared with Er:YAG laser may provide comparable composite resin bond strengths, depending upon the adhesives used. 69,84
Benefits of Laser Irradiation: Minimally Invasive Dentistry, Decontamination, and Safe and Comfortable Interventions
On the other hand, even after the contradictory results presented and negative aspects of laser treatment in enamel and dentin, erbium lasers, in addition to selectively and conservatively promoting caries removal, are able to reduce the local microbiota because of an increase in temperature values, generated during irradiation. 70 –72 It is important to state that even if lasers are able to induce specific increases in temperature values, the absorption of energy by the chromophores present in the tissue, and the mandatory use of a water/air cooling system, are responsible for the low heat transfer to the adjacent tissues, avoiding unwanted effects that may compromise the pulp vitality, and hence the bonding procedures. 85
According to Shahabi et al., laser irradiation is capable of eliminating the microbial content of infected dentin, because the bacteria existent in the water can absorb the irradiation, and this results in cell death. In addition, physical changes in dentin surfaces associated with coagulation of dentinal fluid proteins after laser irradiation could reduce permeability and, consequently, dentin sensitivity, which occurred after cavity preparation in vital teeth. 62 Further, laser beams are able to penetrate into areas deeper than the ablated area and damage nerve terminals, resulting in pain reduction in cavity preparation with laser. 44,62
Also, the possibility of having a wider range of performance parameters, lower pulse durations, and smaller handpieces with a large number of different tips has made this technique easier to use for the operator, while at the same time providing better results in terms of quality. According to Fornaini et al., the use of erbium lasers has given great satisfaction to patients, particularly in comparison with conventional treatments, because of the reduced pain and greater comfort, both during and after the intervention, compared with traditional techniques. 86,87
Final Considerations
Taking into consideration that there is no defined standard protocol concerning the information that articles must provide, it was very difficult to compare the results of the literature in the present study. Data varied regarding the type of adhesive system and resin composite used, the substrate, mean power, energy density, pulse duration, irradiation time, distance, cooling system (water or air spray), adhesives systems used, and the bond strength methodology as observed in Table 1. These variables resulted in conflicting results, which complicates any interpretation and comparison of the current literature on this subject.
Based on the results and discussions presented, it can be said that further studies are necessary in order to define a standard protocol with positive results for similar or higher bond strength values of erbium lasers. Detailed information concerning laser parameters should be provided in the reported literature.
Also, longitudinal clinical studies should be developed with erbium lasers that have high affinity for mineralized tissues, in search of new parameters for irradiation and bonding to restorative materials that behave favorably in the irradiated substrate.
Conclusions
There are few studies with sufficient information and protocol data about laser irradiation in dentin, and the existing articles show conflicting results. The acid-etch technique remains mandatory even after laser conditioning, for both enamel and dentin. Microleakage, in general, is significantly higher in association with Er:YAG enamel/dentin preparation, compared with conventionally prepared substrates. There is no gold standard for the optimal preparation of enamel and dentin, and for conditioning of these surfaces using Er:YAG and Er,Cr:YSGG lasers. Despite the favorable advantages of erbium lasers, clinical studies should be conducted to observe the clinical behavior of adhesive restorations made with erbium lasers.
Footnotes
Acknowledgments
The authors thank the Special Laboratory of Lasers in Dentistry (LELO) from the Department of Restorative Dentistry of the School of Dentistry of the University of São Paulo (USP) and the National Counsel of Technological and Scientific Development - CNPq (Grants # 304198/2010-2 and # 307375/2010-2).
Author Disclosure Statement
No competing financial interests exist.