
Abstract
Introduction
F
Current indications of this technology have been further extended in order to include nonvascular lesions that have vascular structural involvement, which makes them amenable to be treated with such laser. FPDL is not always the first line treatment for scars; these can be successfully treated using different methods, such as ablative lasers or plastic surgery.
Potential adverse events include postinflammatory pigmentary changes (especially in darker-skinned patients), immediate postlaser purpura, recurrence, and infection. Sun exposure can drastically affect pigmentary changes, and sun avoidance/protection is essential to optimizing outcomes. Blistering, crusting, and, rarely, hypertrophic or atrophic scarring may also occur. Surface cooling has markedly diminished this side effect. Swelling and erythema are frequently present immediately after treatment, especially around the eyes, but resolve within 24–48 h.
To better understand FPDL's mode of action on different skin lesions, Karsai et al. classified dermatological disorders into vascular lesions, vascular dependent lesions, and nonvascular lesions. 1
Vascular lesions include port-wine stains, superficial hemangiomas, and teleangectasis in which FPDL is considered the gold standard therapy, as well as angiokeratomas and Bourneville–Pringle syndrome.
Vascular dependent lesions can be divided into: viral infections such as verrucae vulgares and genital viral warts, inflammatory dermatosis such as localized psoriasis and lupus erythematosus, connective tissue diseases such as striae rubrae, neoplastic dermatosis such as basal cell carcinoma, Kaposi's sarcoma, and angiolymphoid hyperplasia. Hypertrophic scars and keloids may be classified within this group.
As pointed out by Tsao et al., 2 there are three types of scars: (1) atrophic scars (most commonly seen in acne and chickenpox scars), (2) exophytic scars (hypertrophic scars and keloids), and (3) flat scars, which are normal scars that gradually become imperceptible with time.
Abnormal wound healing results in hypertrophic scars and keloids, all characterized by a supporting vascular structure.
As has been widely reported, FPDL may also be used on nonvascular lesions, including viral infections such as molluscum contagiosum, or hyperplastic lesions such as xanthelasma palpebrarum. 3 –17
Materials and Methods
During 2012 and 2013, 59 patients with hypertrophic and keloid scars were selected. Patients gave their consent to be treated with the FPDL.
The study design was approved by the local institutional review board, according to the Helsinki Declaration, and patients were enrolled after giving a detailed personal history (skin type, clinical manifestations, health conditions, previous medications, lifestyle) and informed consent. A series of 59 hypertrophic scars and keloids were treated treated in 33 males and 26 females, mean age 37.5 years, skin types I–IV, with no contraindication to laser treatment (pregnancy, photosensitivity, history of skin tumors). Lesions were the result of abdominal and thoracic surgery (33/59), acne (10/59), caesarean sections (11/59), or earrings (5/59). Lesions were treated in four to six sessions, with intervals of at least 30 days and follow-up at 6 months from the last treatment.
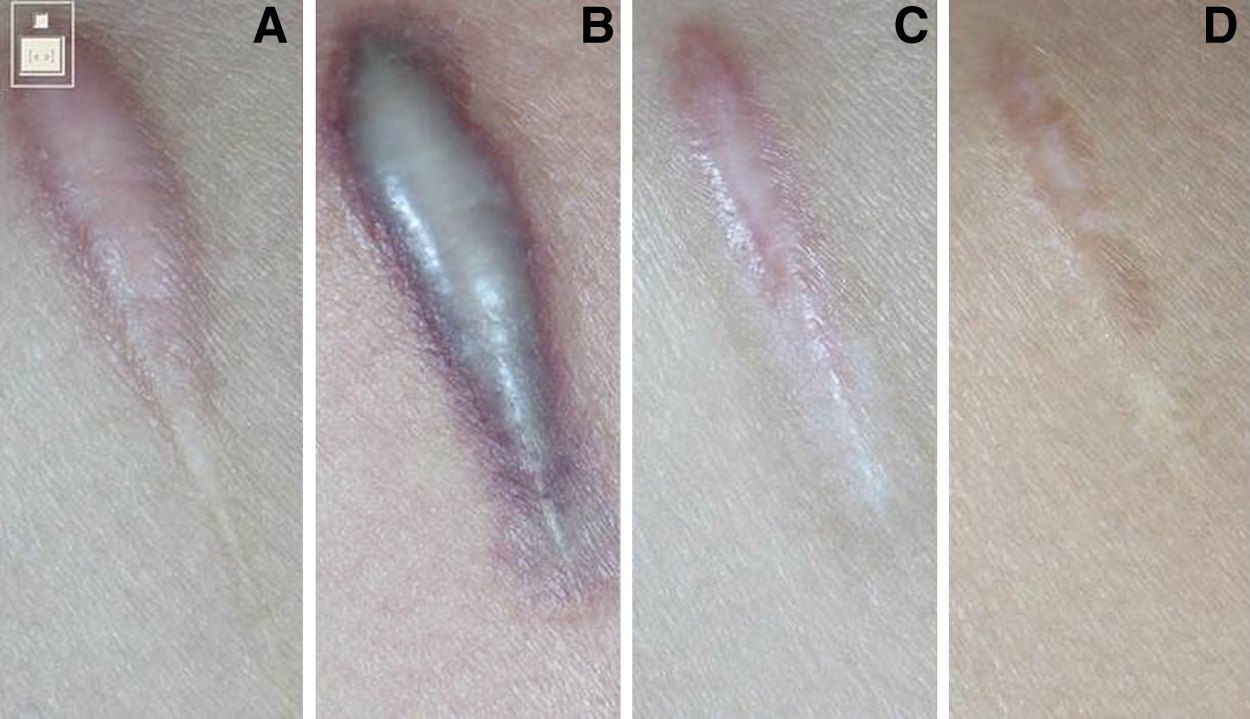
Patients underwent from six to eight monthly laser treatments (Synchro Vas-Q, Deka M.E.L.A., Florence, Italy). Non-overlapping laser pulses with fluences of 6–7 J/cm2 with a 12 mm spot were performed. Pulse duration was 0.5–1.5 ms. Only 3 out of 5 earring keloids (see Fig. 1) and 5 out of 33 postsurgical scars were vaporized with a CO2 ultrapulsed laser before the first FPDL session. All the other lesions (see Fig. 2) were treated with FPDL alone.

Lesions were treated without anesthesia. We limited its use, because the procedure itself was not very painful for the patient, and also because local anesthesia could cause edema and hinder the “visual feedback processing” during treatment. An effective cooling device was always used during each laser session, decreasing the patient's discomfort. Patients were instructed to avoid sun and cosmetics during the immediate postprocedural periods and to apply cool compresses, emollient creams, and sunscreens until complete recovery. Daily application of cool wraps, for the following 3 days, was suggested as being useful in preventing the appearance of vesicles and blisters.
An antibiotic ointment containing Fucidic Acid, was also applied to the target areas for 7 days after each laser session, preventing potential cutaneous infections and crustings.
Photographs were taken with a Canon digital camera and a polarized flash (Anthology system, DEKA-M.E.L.A., Calenzano, Italy), before and after each treatment, and 6 months and 12 months after the final treatment. Photographs were standardized using the same camera, shooting setting, twin flash, ambient light, and chin holder to guarantee the same distance and to observe the results achieved in the best way.
Results obtained were judged by three dermatologists, blinded investigators, 6 months after the last session; they had not taken part in the treatments and they assessed the performance of this device by ranking the results into four categories, a quartile scale of lesion clearance, in terms of improvement of the scar color, height, pliability, and texture: 1=no or low results (0–25% of the lesion area improved), 2=slight improvement (25–50% of the lesion area cleared), 3=moderate-good improvement (50–75%) and 4=excellent improvement (75–100%).
Photographs were used by blinded observers to also evaluate the removal of the lesions and the possible recruitments as well as by the patients, who were asked for a subjective evaluation of the perceived overall results by means of the following score: disssatisfied, not very satisfied, satisfied, very satisfied.
Results
All patients observed global improvements. All the lesions were removed except in three cases.
A total of 29 out of 59 (49.1%) achieved excellent clearance, 15 patients (25.4%) achieved good-moderate clearance, 12 patients (20.4%) obtained slight clearance, and 3 patients (5.08%) had little or no removal of their lesion (Table 1).
Patients were asked for a subjective evaluation of the results: 37/59 patients (62.7%) were very satisfied, 18 (30.5%) were satisfied, and 4 (6.7%) were not very satisfied with the results. No patients were dissatisfied (Table 2); low satisfaction was probably the result of purpura produced by the use of higher parameters, which did not allow the patient to have a normal lifestyle up to 10 days after treatment. Relevant side effects as blisters, crusts, atrophy, and scars, were absent in all conditions; the most common adverse side effect was purpura, which occurred in 37/59 patients and took 7–10 days to resolve. Hyperpigmentation was seen in seven cases. Transient hypopigmentation and blistering were also reported in two and one cases, respectively.
Figures 1 and 2 show cases of successful treatment of the ear lobe and the breastbone, respectively.
Discussion
Although intense PDL is a nonablative technology normally used in vascular malformation therapy, our clinical experience and other reports allowed us to treat patients with typically nonvascular lesions such as keloids.
The crucial point we must assess is whether the observed patient improvement after FPDL treatment could provide the means for a valid alternative to other excellent and less expensive strategies or that its use might more likely result in response variability if extended to other patients. In our study, the choice of an appropriate therapy was based on patient age, condition, compliance, sites of the lesions, contraindications, and potential adverse events. Children, for example, may become alarmed by treatment and refuse painful procedures, resulting in poor patient compliance. 18 Cardiopathic patients, subjects using anticoagulant drugs, or those unable to receive anesthesia have great difficulty in undergoing surgical treatment, and are thereby more likely candidates for PDL treatment. Pregnant women as well have limitations in the use of certain local, systemic, or surgical treatments.
Lastly, surgery is not recommended in certain areas, such as the face, the breast, the tip of the nose, or the nasal wings, because of the risk of new scarring.
Most of the lesions we treated contained a large number of dilated blood vessels, which were the target of the device.
In other dermatological conditions, there is uncertainty about the modality of action. In instances of keloids and hypertrophic scars, the hypoperfusion and hypoxia provoked by PDL may result in neocollagenesis, collagen fiber heating with dissociation of disulfide bonds and subsequent collagen fiber realignment, release of histamine, or other biochemical factors that influence fibroblast activity. 16 –18 Biochemical studies performed by Kuo et al. 18 have shown a decrease in the induction of transforming growth factor-beta1 (TGF-β1) and upregulation of matrix metalloproteinase (MMP) expression in keloid tissue treated with a 585 nm PDL. This would favor collagen degradation and fibroblast apoptosis. These authors reported 50% improvement in 26 of 30 patients with keloids after five to six treatments using 585 nm, 0.45 ms pulse, 5 mm spot, and 10–18 J/cm2. According to previous unpublished experience, keloid treatment results are very promising, with an excellent rate of success after 5 years of follow-up, especially for the treatment of the earlobe keloids, which is hat's why, in our opinion, it may also be considered a smart alternative or complementary treatment for hypertrophic scars and keloids that are usually resistant to other therapies.
Similarly to other studies, the most common adverse side effect of 585 nm FPDL treatment was purpura, which took 7–10 days to resolve. Hyperpigmentation was seen in seven cases. Transient hypopigmentation and blistering have also been reported.
Conclusions
PDL has been found to be as safe and effective as the main or complementary treatment for various dermatological disorders in which an alteration of skin microvessels may play a role in pathogenesis. Its usage however, is limited to select cases in which main-stain therapy have not proven to be effective or when patients are unable to undergo such treatments. Although the high cost of PDL therapy limits its usage, it is particularly effective for its extraordinary aesthetic results and can be considered a valid treatment option. Future multicenter studies with additional patients, however, are desirable, with possible harmonization of methodologies.
Footnotes
Author Disclosure Statement
No competing financial interests exist.