
Abstract
Introduction
T
Researchers and clinicians have worked to solve this clinical dilemma over the past few decades. Ultrasonic and EndoActivator (Dentsply Tulsa Dental Specialties, Tulsa, OK) irrigation systems have been developed as adjunct procedures to enhance the removal of Ca(OH)2 remnants after needle irrigation. 19 Because of its activation of irrigants and its clinical availability, ultrasonic irrigation is now commonly used. However, the effectiveness of ultrasonic irrigation in removing Ca(OH)2 varies greatly depending upon the irrigating solution and paste vehicle used. 16,19
Recently, photon-induced photoacoustic streaming (PIPS), a laser-activated approach, has shown more efficiency in fluid interchange and in removing debris from root canal systems than other techniques. 20 –22 PIPS generates peak power spikes and intensive shockwaves in water with minimal thermal effect, using low-energy levels and short (50 μs) pulse rates. Divito et al. reported that PIPS resulted in significantly better root canal debridement than traditional irrigation techniques. 20 Contaminated isthmus areas, which harbor bacteria and serve as an intracanal medicaments reservoir, account for many endodontic treatment failures. 23 Theoretically, PIPS photoacoustic streaming can travel three dimensionally wherever fluid is present in the root canal, to effectively debride the entire root canal system with placement of the tip into the coronal portion only. 20 This advantage may enable PIPS to clean isthmus regions better than conventional irrigation techniques. To our knowledge, no studies have investigated the effectiveness of PIPS in removing Ca(OH)2 residues from the isthmus areas of root canals.
The aim of this in vitro study was to use high resolution micro-computed tomography (micro-CT) and scanning electron microscopy (SEM) to evaluate the effectiveness of four different irrigation techniques (PIPS, ultrasonic, EndoActivator, and needle) in removing Ca(OH)2 residues from the main root canals and isthmus areas of premolar teeth.
Materials and Methods
Sample collection and selection
Approval for this study was obtained from the Research Ethics Committee, Chinese PLA Air Force General Hospital. Thirty-two freshly extracted maxillary first premolars were randomly selected from the native Chinese population. Teeth were extracted for reasons not related to this study. Samples with immature apical foramina, endodontic treatment, non-carious cervical lesions, or root fracture were excluded. All samples were rinsed with tap water and stored in neutral-buffered formalin solution until further use. Soft tissues and dental calculus were removed by hand with a periodontal scaler. All samples were scanned with micro-CT (Skyscan, Aartselaar, Belgium) at an isotropic resolution of 20 μm. The X-ray tube was operated at 80 kV and 100 mA. Image slices were reconstructed and 24 samples containing an isthmus, according to Weller's criteria, were selected for further study. 23
Root canal instrumentation
A conventional access cavity was prepared and an endodontic explorer was used to detect the pulp chamber anatomy and canal orifices. A size 10 K-file (Dentsply Maillefer, Ballaigues, Switzerland) was introduced into the canal until the file tip reached the apical foramen, to establish apical patency. The working length was registered as 0.5 mm shorter than the length to the foramen. The canals were instrumented with size 15 and size 20 hand files. Next, the canals were instrumented with ProTaper rotary instruments (Dentsply Maillefer, Ballaigues, Switzerland) according to manufacturer's instructions; the final instrument was an F2 file. A 30 gauge blunt-tip needle (Terumo Corporation, Leaven, Belgium) was used to fill the root canal with 3% sodium hypochlorite solution irrigant. Pulp chamber and root canals were filled with irrigating solution during canal instrumentation. The canals were flushed with 3 mL of 3% sodium hypochlorite solution between instruments. After instrumentation, 6 mL of 17% ethylenediaminetetraacetic acid (EDTA) solution was used to irrigate the canal for 3 min as the final rinse. The irrigation solution in the pulp chamber was aspirated and the canals were dried with paper points.
Intracanal Ca(OH)2 filling
Sterile Ca(OH)2 is a radiopaque, water-soluble root canal medicament with 8.33 wt% barium sulfate (Nordiska Dental, Angelholm, Sweden). Ca(OH)2 paste was injected into the root canal until paste was extruded from the apical foramen. Lentulo spiral fillers (Dentsply Maillefer) were used to pack the slurry into the canals. A cotton pellet was placed over Ca(OH)2 paste and the coronal access cavities were sealed with Cavitron temporary filling material (GC, Tokyo, Japan). The root apex was covered with sticky wax to replicate the surrounding periodontal tissues and their effect on the dynamics of the irrigating solution. All samples were stored at 37°C and 100% humidity for 1 week.
Removal of Ca(OH)2
After removing the temporary coronal filling material, Ca(OH)2 was removed by a standard protocol, including an F2 instrument and 3 mL of 3% sodium hypochlorite (NaOCl) irrigating solution via a 30 gauge needle at 1 mm short of the working length of the canal. The samples were then randomly divided into the following four groups of six each, according to irrigation protocol. All operating procedures were performed by the same endodontist.
Group 1: Needle irrigation
Each root canal was irrigated with 6 mL of 3% NaOCl solution for 60 sec using a 30-gauge blunt-tip needle (Ultradent, South Jordan, UT) situated 1 mm short of the working length. Irrigating solution was delivered at a flow rate of 6 mL/min.
Group 2: EndoActivator irrigation
Each root canal was irrigated with EndoActivator for 60 sec (setting: headpieces 10,000 cycles per min). A sonic tip (size 20, taper 0.02) was inserted into the canal and agitated 2 mm short of the working length without touching the walls. The root canal was filled with 2 mL of 3% NaOCl, and then activated by EndoActivator for 20 sec. The procedure was repeated three times.
Group 3: Ultrasonic irrigation
Each root canal was irrigated with an ultrasonic device for 60 s (setting: E mode 25% power) (EMS, Le Sentier, Switzerland). An ultrasonic tip (size 20, taper 0.02) was inserted into the canal and agitated 2 mm short of the working length. The root canal was filled with 2 mL of 3% NaOCl solution, and then activated by the ultrasonic device for 20 sec. The procedure was repeated three times.
Group 4: PIPS irrigation
Each root canal was irrigated with an Er.YAG laser (Fidelis AT, Fotona, Ljubljana, Slovenia; 2940 nm wavelength, 0.3 W, 15 Hz, and 20 mJ without water or air) for 60 sec. A 14 mm long, 300 μm diameter quartz tip was used. The root canal was filled with 2 mL of 3% NaOCl solution, then the laser tip was put into the coronal part of the canal and activated for 20 sec. When the irrigant in the coronal reservoir dropped, the pulp chamber was refreshed with 3% NaOCl solution. Three 20 sec activation procedures were performed.
Micro-CT scan and measurement
All samples were scanned with micro-CT three times: before instrumentation (scan 1), after Ca(OH)2 filling (scan 2), and after irrigation (scan 3). Image data processing was performed with MeVisLab 2.6.1 software package (MeVis Medical Solution AG, Bremen, Germany). The region of interest (ROI) was selected from the cementoenamel junction (CEJ) layer to the root apex layer. The CEJ layer was defined as where enamel occupied half of the tooth perimeter in cross-section. 24 Image data from scans 2 and 3 were registered and used to evaluate Ca(OH)2 removal in the coronal two thirds of the root. Image data from scans 1 and 2 were registered and used to segment Ca(OH)2 in the isthmus region before irrigation. Image data from scans 1 and 3 were registered and used to segment residual Ca(OH)2 in the isthmus region after irrigation.
SEM evaluation
After canal irrigation, two longitudinal grooves were prepared with a diamond disc, one on the buccal and one on the lingual surface of the root. Next, the root was longitudinally split with a bone hammer. Samples were dehydrated step by step with absolute alcohol, dried at the critical point, and sputter-coated with gold (Magnetron Ion Sputter Metal Coating Device, Msp-2S, IXRF System, Inc. MA, Japan). The presence of Ca(OH)2 remnants in the coronal, middle, and apical thirds of each sample were assessed with SEM (Hitachi, Tokyo, Japan; magnification 1000×). Two calibrated examiners evaluated the cleanliness of the root canal walls according to the following scoring system: 0, no residue; 1, small amount of residue (covering ≤20% of the surface); 2, moderate amount of residue (covering 20–60% of the surface); 3, large amount of residue (covering >60% of the surface). 25
Statistical analysis
Data were analyzed with repeated-measures Kruskal–Wallis and Mann–Whitney–Wilcoxon U tests. All analyses were conducted using SPSS software (SPSS 20.0 for Windows, SPSS, Chicago, IL). The level of significance was defined as p<0.05.
Results
Micro-CT imaging study and quantitative evaluation
In the coronal third of the root canal, the mean reduction in volume of Ca(OH)2 after irrigation with needle, EndoActivator, ultrasonic, and PIPS was 94.24±9.84%, 98.54±1.55%, 100.00±0.00%, and 100.00±0.00%, respectively. In the middle third of the root canal, the four groups showed a similar trend, but the mean Ca(OH)2 reduction percentages were all less than in the apical third. There were no significant differences among the four groups in Ca(OH)2 reduction in the coronal and middle thirds of the root canal (both p>0.05). In the apical third, ultrasonic irrigation and PIPS eliminated a higher percentage of Ca(OH)2 than did needle and EndoActivator irrigation (p<0.05) (Table 1). There was no significant difference between the ultrasonic and PIPS groups (p>0.05), or between the needle and EndoActivator groups. However, none of the techniques completely eliminated Ca(OH)2 from the apical third of the root canal (Fig. 1).
Three-dimensional reconstruction of micro-CT scans showing Ca(OH)2 in the apical third of root canal before and after irrigation. Needle (A1, before irrigation; A2, after irrigation), EndoActivator (B1, before irrigation; B2, after irrigation), ultrasonic (C1, before irrigation; C2, after irrigation), and photon-induced photoacoustic streaming (PIPS) (D1, before irrigation; D2, after irrigation).
Ranking: there were significant differences (p<0.05) in the means between subgroups with different ranks.
PIPS, photon-induced photoacoustic streaming.
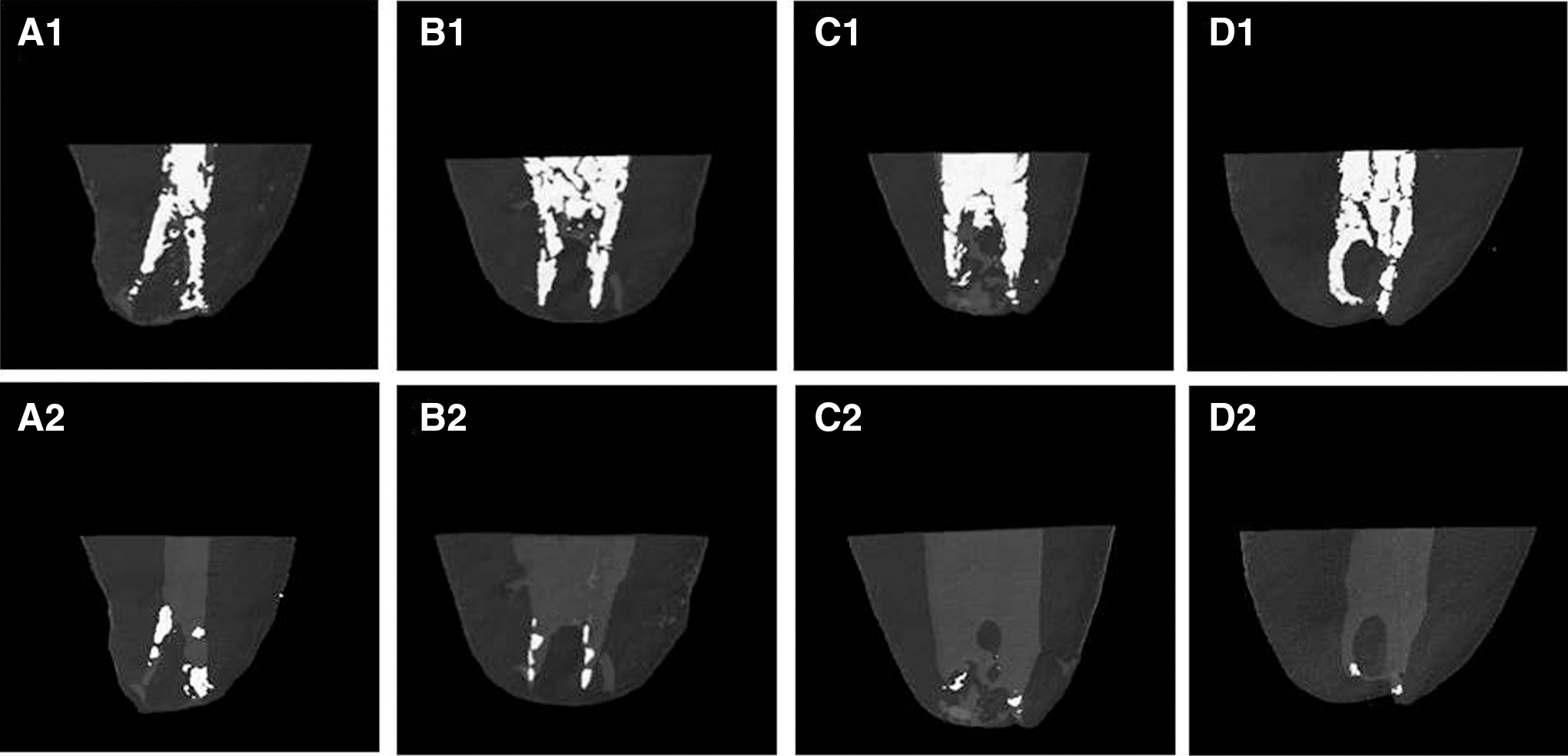
The mean Ca(OH)2 volume reductions in the canal isthmus regions with each removal technique are shown in Table 2. Ultrasonic and PIPS irrigation were more effective than the needle and EndoActivator irrigation (p<0.05) (Table 2, Fig. 2). There was no significant difference between the ultrasonic and PIPS groups (p>0.05) or between the needle and EndoActivator groups (p>0.05).

Micro-CT images of Ca(OH)2 in the isthmus region before and after irrigation. Needle (A1, before irrigation; A2, after irrigation); EndoActivator (B1, before irrigation; B2, after irrigation); Ultrasonic (C1, before irrigation; C2, after irrigation) and photon-induced photoacoustic streaming (PIPS) (D1, before irrigation; D2, after irrigation).
Ranking: there were significant differences (p<0.05) in the means between subgroups with different ranks.
PIPS, photon-induced photoacoustic streaming.
SEM observation and quantitative evaluation
SEM images representative of Ca(OH)2 residues in the coronal, middle, and apical thirds of the root canals in each group are shown in Fig. 3. Root canals in the ultrasonic and PIPS groups generally had less Ca(OH)2 residue than did those in the needle and EndoActivator groups. Within each group, Ca(OH)2 residues were present in the following order: apical>middle>coronal. None of the methods completely eliminated Ca(OH)2 from the apical-third canals. Figure 4 shows SEM images representative of the assigned residue scores. Ca(OH)2 residue scores in each region of the root canal in each treatment group are summarized in Table 3. In all areas of the root canal, ultrasonic and PIPS irrigation were more efficient than EndoActivator and needle irrigation in removing Ca(OH)2 (all p<0.05). There was no significant difference between ultrasonic and PIPS groups (p>0.05) or between needle and EndoActivator groups (p>0.05).
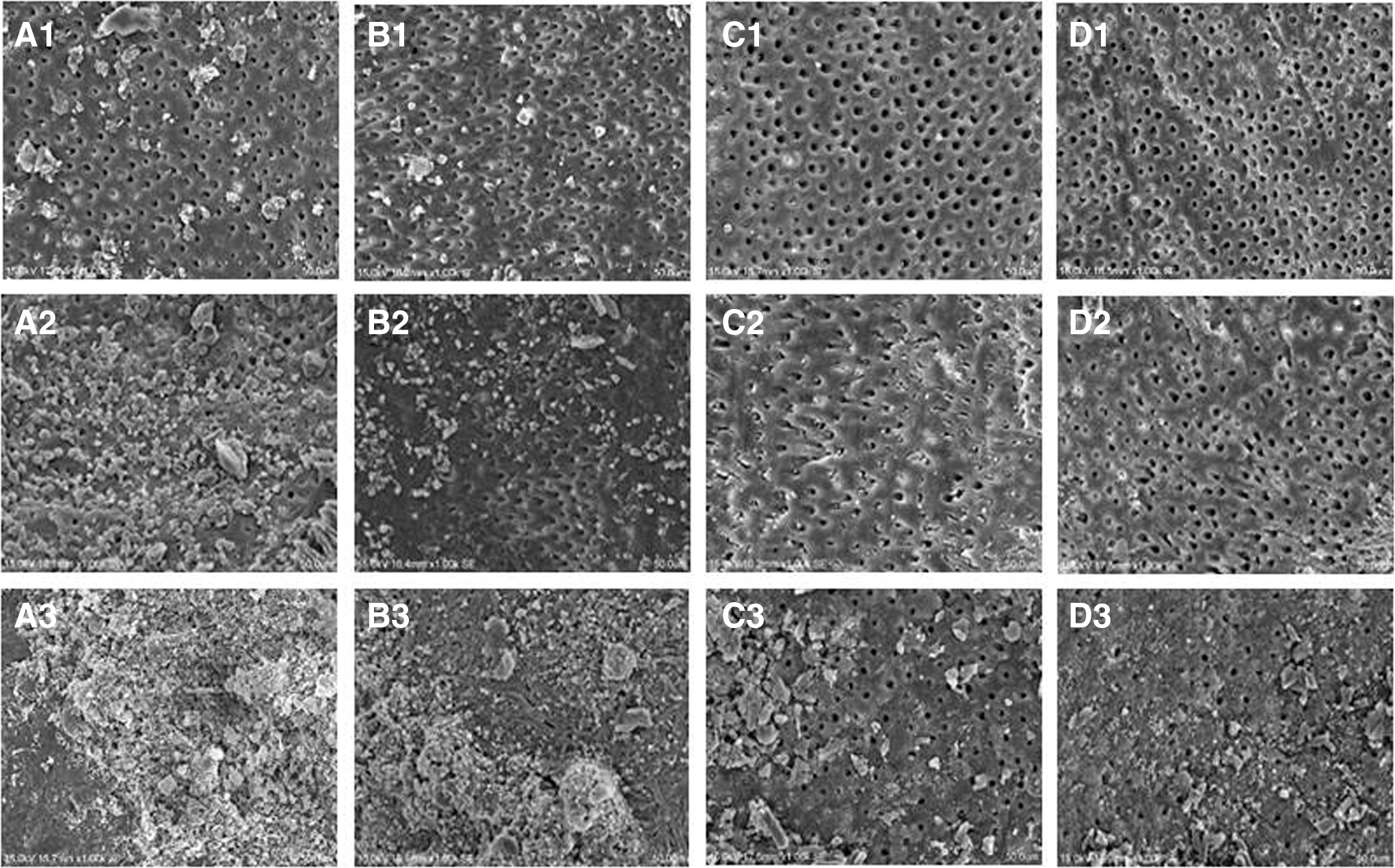
Scanning electron microscopic (SEM) images of Ca(OH)2 residues in the coronal, middle, and apical third of root canal after irrigation with four different irrigation techniques. Needle (A1, coronal third; A2, middle third; A3, apical third), EndoActivator (B1, coronal third; B2, middle third; B3, apical third), Ultrasonic (C1, coronal third; C2, middle third; C3, apical third), and photon-induced photoacoustic streaming (PIPS) (D1, coronal third; D2, middle third; D3, apical third).
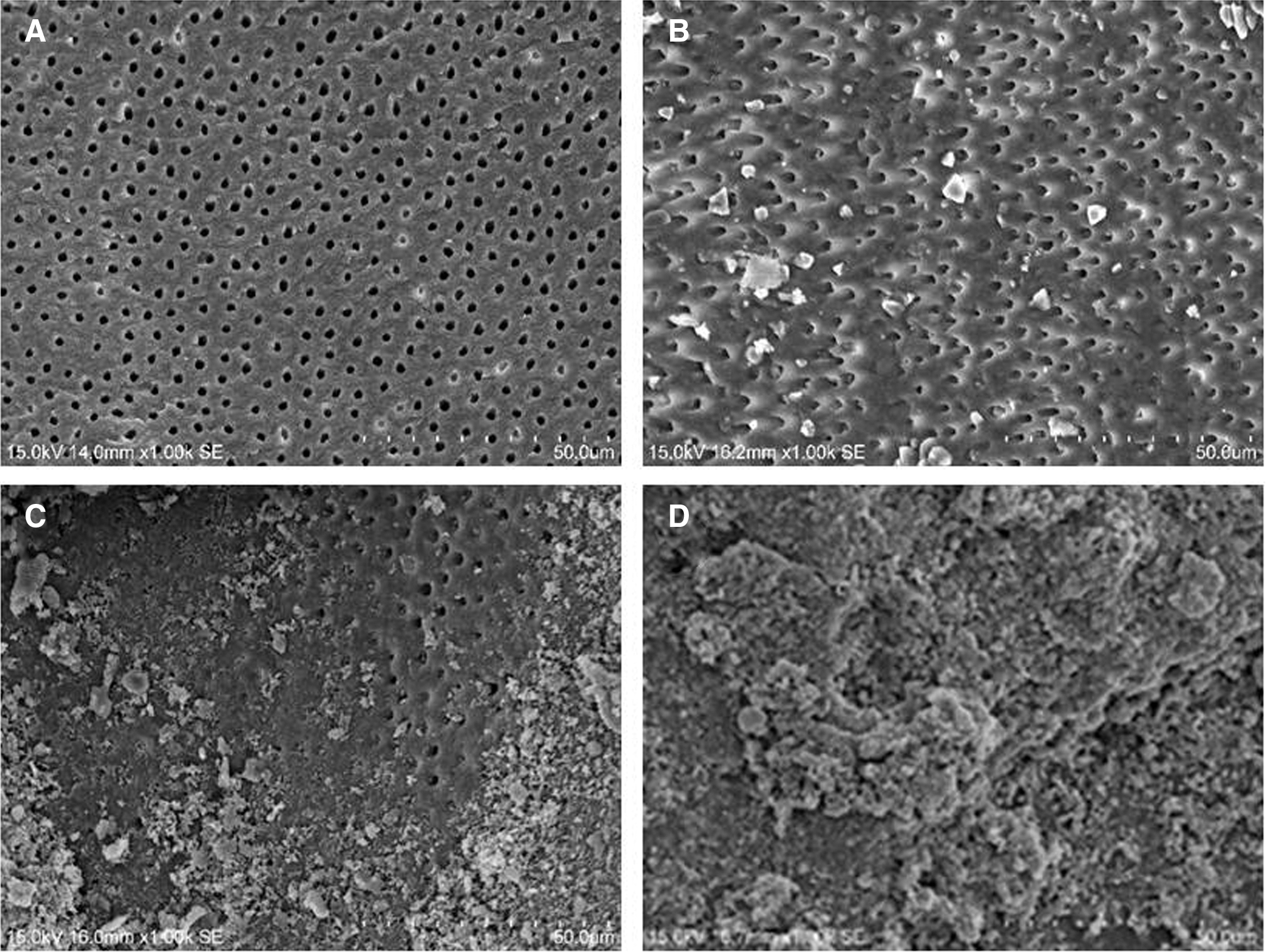
Scanning electron microscopic (SEM) images representative of Ca(OH)2 residue scores.
Ranking: there were significant differences (p<0.05) in the means between subgroups with different ranks.
PIPS, photon-induced photoacoustic streaming.
Discussion
Application of Ca(OH)2 paste to disinfect the entire root canal system, especially irregular areas such as the isthmus regions and apical deltas, greatly contributes to the success of endodontic treatment. 26 Ca(OH)2 paste in its flowable form can penetrate canal irregularities, which increases the difficulty of subsequent Ca(OH)2 removal. 27 It has been clearly shown that residual Ca(OH)2 present in the main root canal and/or its isthmus prior to final canal obturation compromises hermetic root canal sealing by root canal filling materials. 28 Therefore, complete removal of Ca(OH)2 is crucial. However, conventional irrigation techniques such as needle irrigation do not effectively remove Ca(OH)2 from the isthmus area and apical delta. 29 In the present study, we compared currently available devices (EndoActivator, ultrasonic, and PIPS) with needle irrigation to determine appropriate protocols for removing Ca(OH)2 from the main root canal and isthmus.
Based on micro-CT data analysis, we found that ultrasonic and PIPS irrigation were superior to EndoActivator and needle irrigation in removing Ca(OH)2 from the isthmus regions of the root canal of maxillary premolars. This finding supports that of a previous study, which found that PIPS eliminated significantly more organic debris from the canal isthmus than did needle irrigation. 21 PIPS was developed as a novel laser agitation irrigation technique to clean and debride the root canal system after instrumentation. PIPS employs Erbium:yttrium-aluminum-garnet (Er:YAG) laser energy at subablative parameters (lower power 0.3 W, 20 mJ at 15 Hz) with a newly designed radial and stripped tip to create peak power spikes. 20,22 Er:YAG laser energy exhibits the highest absorption by water and hydroxyapatite of any laser, causing three-dimensional agitation of fluid throughout the root canal. 20 Additionally, Er:YAG laser can produce cavitation effects through formation of explosive vapor bubbles, enhancing the effectiveness of Ca(OH)2 and debris removal from intricate anatomy, including the subcanals and isthmus regions. 30
Most endodontists recommend a final ultrasonic irrigation as a routine step in root canal cleaning. This additional step results in more efficient debridement in the isthmus region than the needle technique alone. 31 Similarly, the present study showed that ultrasonic irrigation produced a cleaner root canal surface than other techniques, with less Ca(OH)2 remaining in the main canal and isthmus areas. Ultrasonic vibration activates irrigants and enhances fluid movement and exchange. 32 The highly mobile irrigant molecules can penetrate the irregular isthmus region and remove Ca(OH)2 located there. Continuous delivery of fresh irrigant and prolonged ultrasonic activation may have synergistic cleaning effects. However, the optimal parameters of the combination need further study.
Micro-CT revealed no difference in Ca(OH)2 volume reduction among the four irrigation groups in the coronal and middle thirds of the root canal. Needle, EndoActivator, ultrasonic, and PIPS irrigation all effectively removed Ca(OH)2 from the coronal and middle thirds of the root canal of the maxillary premolars. However, in the apical third, the PIPS and ultrasonic groups had significantly higher Ca(OH)2-removal percentages than did the EndoActivator and needle groups. A possible explanation for this difference in the case of PIPS is that the system generates a strong and significant photoacoustic shock wave, which could enhance three-dimensional spreading of irrigants into the apical third. The higher efficacy of ultrasonic irrigation likely resulted from transmission of ultrasonic energy to the irrigant, producing high shear stress in the root canal system. 22 In contrast, needle irrigation and EndoActivator did not clean the apical third or the isthmus areas effectively, even when their tips were placed close to the root apex. It has been reported that trapped air in the apical area creates a vapor lock and block, which prevents fluid movement and exchange. 29 Unlike PIPS and ultrasonic irrigation, neither needle nor EndoActivator irrigation can produce adequate fluid movement to suck air from the apical region or destroy the dead block. Furthermore, the needle delivers irrigants no further than 1 mm beyond the needle tip, and therefore the apical third is inaccessible for flushing. 33,34 EndoActivator, delivering insufficient volume of irrigants to the apical area and lacking cavitation, resulted in low efficiency of Ca(OH)2 removal. 35,36
Although micro-CT has been widely used in dentistry and has several distinct advantages, including the non-destructive nature of the imaging, the lack of sample staining preparation needed, and the rapid speed of data acquisition, one disadvantage is its poor assessment of less radiopaque materials and tissues; such as the smear layer and Ca(OH)2 particles on the root canal wall. SEM reveals the detailed morphology of the root canal surface and allows quantification of radiolucent materials present on the root canal wall. 37 Therefore, we used SEM (1000×) to observe and categorize Ca(OH)2 removal from the root canal wall with a four scale scoring system, which has been described previously and was well calibrated in a series of studies. 25
Ca(OH)2 residue scores in the PIPS and ultrasonic groups were significantly lower than those in the EndoActivator and needle groups in the coronal, middle, and apical thirds of the root canals. These SEM results were not completely consistent with the micro-CT findings. SEM imaging revealed that PIPS and ultrasonic irrigation removed Ca(OH)2 significantly more thoroughly than EndoActivator or needle irrigation in the coronal and middle thirds of the root canal, whereas micro-CT showed no difference among the four groups in Ca(OH)2 volume reduction in these regions. Micro-CT did not reveal the difference, because the technique is not sensitive enough to reveal Ca(OH)2 particles.
Notably, our study showed that no irrigation technique completely eliminated Ca(OH)2 from the entire canal system. This finding is in agreement with those of previous studies. 19,38 Because the PIPS tip was placed in the orifice area, the irrigant flow generated might not have been strong enough to travel into the apical third, because of declining fluid flow capacity. Alternatively, the energy of PIPS may not have been sufficient to activate irrigant flow in the apical third. 39 Similarly, acoustic microstreaming and/or cavitation significantly decreases or disappears when the activated tip leaves the irrigant and enters the apical vapor lock. 40 Therefore, more effective methods of completely cleaning the apical portion need to be developed.
Conclusions
In summary, PIPS and ultrasonic irrigation techniques more effectively removed Ca(OH)2 from the main canal and isthmus areas in maxillary premolars than did EndoActivator or needle irrigation, but did not completely remove Ca(OH)2 from the apical third of the root canal.
Footnotes
Author Disclosure Statement
No competing financial interests exist.